Article Text

Abstract
Objectives The objective of this study is to assess the effect of reminder text messages 6 months after the initial treatment on retest and chlamydia reinfection rates in young heterosexuals compared with a historical control group and to assess factors associated with both outcomes.
Methods Heterosexual people (aged 16–23 years), testing positive for urogenital chlamydia, were offered a retest after 6 months. Participants received a text message reminder at 6 months after the initial chlamydia diagnosis. Rates of retest uptake and the result of the retest were analysed using Cox regression. Prevalence ratios (PRs) were calculated to identify factors associated with these outcomes. Furthermore, the retest rate was compared with the retest rate of a historical control group.
Results 30.6% (253/838) of the study group returned within 5–8 months compared with 9.2% (140/1530) in the historical control group. Women and persons who were not notified for a sexually transmitted infection (STI) at inclusion were more likely to return for a retest. 20.4% (56/275) of participants had a chlamydia reinfection upon retesting. Reinfection was higher in participants reporting STI-related symptoms (PR 3.2, 95% CI1.8 to 5.6) and in participants who were notified for an STI at retest (PR 5.3, 95% CI 2.4 to 11.5).
Conclusions A text message reminder appeared to have a clear, positive impact on the resulting retest rate. These results also indicate that retesting is necessary to identify chlamydia reinfections.
- CHLAMYDIA TRACHOMATIS
- COMMUNITY SERVICES
- PUBLIC HEALTH
- ADOLESCENT
- EPIDEMIOLOGY (GENERAL)
Statistics from Altmetric.com
Introduction
In the Netherlands, a significant part of sexually transmitted infection (STI) care is provided by the freely accessible, low-threshold STI clinics, where one can have an STI test free of charge and anonymously. Most of these clinics are based within the public health services, providing STI care additional to first-line care by general practitioners. The STI clinics are government funded aiming to reach high-risk groups, including young people (aged below 25 years) and men having sex with men (MSM), who might otherwise not seek timely STI care.1
Of all the heterosexual individuals who visited a municipal STI clinic, 15.2% (8252/54315) of young heterosexuals (aged 15–24 years) were diagnosed with chlamydia in 2012.2 Therefore, chlamydia remains the most commonly diagnosed bacterial STI. The majority of chlamydia infections are found among young people below the age of 25 years.2 There are a number of international studies that conclude that young people with chlamydia are at risk for reinfection and should, therefore, be retested.3–5 Retesting is crucial because chlamydia infections, especially repeated episodes, are associated with pelvic inflammatory disease and other reproductive sequelae.6 In a database study performed in the USA among women aged 15–25 years with a chlamydia infection between 2002 and 2006, the estimated majority of reinfections occurred between 2 and 5 months after treatment of the initial chlamydia infection.7
Dutch dermatological guidelines already recommend retesting patients with chlamydia infections 6 months after the initial treatment.8 Dutch research provides evidence for high chlamydia reinfection rates at retest: a retrospective study in South Limburg, in which retesting was performed based on a clients’ own initiative, found a chlamydia reinfection rate of 19.0% in the period of 3–12 months after the initial chlamydia diagnosis.9 Other evidence for high chlamydia reinfection rates at retest was provided by a Dutch prospective study, in which clients received a home-based test or a retest at a clinic without the need for an appointment. The reinfection rate in this study was 17.3%.10 Until now, no prospective study in the Netherlands has evaluated the efficacy of sending a simple mobile phone text message to invite chlamydia-positive young individuals for a retest.
The aim of this study is to assess the effect of reminder text messages 6 months after the initial treatment on retest and chlamydia reinfection rates in young heterosexuals compared with a historical control group and to assess factors associated with both outcomes.
Methods
Study setting, study design and population
We performed a prospective follow-up study, using 10 of the 25 STI clinics in the Netherlands (see figure 1). The selected clinics were mainly situated in rural areas. People are free to go to any STI clinic in the Netherlands, but clients who participated in this study could only go to one of the selected STI clinics for a retest. All clients aged between 16 and 23 years, with a positive laboratory test for urogenital chlamydia, diagnosed at one of the study STI clinics between May 2012 and May 2013, and who were treated with Azithromycin 1000 mg, were asked to participate in the study. We excluded clients aged 24 years and older at T0, since they might have turned 25 years at retest (T1) and they are therefore not eligible for a free STI test at the STI clinic. We excluded MSM as well, as this target group already receives retest advice according to national guidelines. However, bisexual women were included in this study, since they are not offered this advice. For brevity, bisexual women are regarded as ‘heterosexual’ in this study.

Counties covered by sexually transmitted infection clinics participating in the current study (in dark grey), the Netherlands, 2012–2013.
As a control group, we retrospectively selected clients, satisfying the same inclusion criteria, from the period January 2011 to January 2012. The control group was analysed to determine how many clients had undergone a repeat test based on their own initiative; the control group did not receive a text message reminder for retesting. The retest rate of the study group is compared with this control group. The reinfection rates and factors associated with response to the retest offer and positivity at retest were also analysed.
Data collection
For the sample size calculation, we used data of our historical control group, in which 9% (140/1530) came back on their own initiative for a retest between 5 and 8 months. We expected that after sending a text message, 20% of the participants in our study group would come back for a retest between 5 and 8 months. With an error of 5% (alpha) and a power of 90%, we would have to include a total of 211 participants in both our study group and historical control group. The historical control group was already reviewed before the start of the study and consisted of 547 persons, so ample for meaningful comparison.
Clients meeting the inclusion criteria were asked to participate in the study upon receipt of a positive chlamydia test outcome (T0). They received a letter detailing the study and were asked to complete a consent form. Five-and-a-half months after being treated for the chlamydia infection, participants received a mobile phone text message, asking them to schedule an appointment for a retest. Two weeks later, a second text message was sent as a reminder. The study allocated a 2-month period in which a retest counted as a retest in the study data (T1), starting after the second text message. Due to the fact that the inclusion period covered 12 months and the maximum follow-up period spanned 8 months, the total study period was 20 months.
In the event that clients visited the STI clinic before receiving the first retest reminder, that is, as a result of STI symptoms or notification, and the test provided a chlamydia-positive outcome, then the test was considered a retest. If the test results were found to be chlamydia negative, then the client still received the text messages 5.5 and 6 months after T0. Participants could only participate once; when participants tested positive in a retest, they could not enter the study for the second time.
All participating STI clinics used an on-line patient registration system. The following variables were used in the analyses at T0 and T1: gender, age, ethnicity (when the participant or one of his/her parents was born outside the Netherlands, the participant was regarded as having a non-Dutch ethnicity), notification by a partner, STI symptoms, living in a city or a rural area, number of sexual partners in the last 6 months and condom use during the last sexual contact.
Data analysis
The χ2 test was used for testing differences in proportions between participants and non-participants. A p value of <0.05 was considered to be statistically significant. Since our main outcomes (participation in retesting and chlamydia positivity at retest) were common (prevalence >10%), Cox regression analyses were performed to identify factors associated with the resulting outcomes. Factors associated with a p value of <0.20 in univariate analyses were further analysed by multivariate Cox regression, using the Enter method, in which we manually selected the factors to be used in the multivariate regression analyses. In the multivariate model, factors with a p<0.05 were considered to be statistically significant. Prevalence ratios (PRs) and 95% CIs were calculated to compare the proportions of the factors associated with retesting (table 1) or reinfection (table 2) between both groups. Analyses were carried out using the IBM SPSS software V.22.
Factors associated with retesting and retest rate with regard to chlamydia retesting in 10 participating sexually transmitted infection (STI) clinics in the Netherlands, May 2012–May 2013
Characteristics and chlamydia positivity rates of participants who came for retest in one of the 10 participating sexually transmitted infection (STI) clinics in the Netherlands, 2012–2013
Results
Study population
A total number of 2108 young people were eligible to participate in the study, of which 828 (39.3%) gave consent to participate. Participants differed from non-participants with respect to gender (72.9% (576/789) of participants were women vs 61.7% (806/1306) of non-participants), STI symptoms (32.4% (253/784) vs 37.5% (488/1301), respectively) and being notified for an STI (29.1% (231/788) vs 34.5% (453/1313), respectively, all p<0.05).
Response to the retest offer
Within 8 months after the initial test, 33.2% (275/828) of the participants returned for a retest. Eight per cent (22/275) requested a retest based on their own initiative (before receiving a text message reminder), tested chlamydia positive and were, therefore, considered ‘retesters’. The actual response after receiving the reminder text message was 30.6% (253/828).
As shown in table 1, the retest rate was significantly higher for women (36.5% (219/600) vs 24.6% (56/228)), for Dutch participants (34.9% (246/704) vs 23.4% (29/124)) and for participants who were not notified (at T0) (36.9% (225/610) vs 22.9% (50/218)), all p<0.05. In multivariate analyses, being women (PR 1.4, 95% CI1.0 to 1.9) and not being notified by a partner at T0 (PR 0.6, 95% CI 0.5 to 0.9) were significantly associated with retesting.
Reinfection rates
We found a total number of 56 chlamydia reinfections among those who came back for a retest before or after the text message reminder, indicating a positivity rate of 20.4% (56/275). This is higher than the overall chlamydia positivity rate among all eligible visitors of the STI clinic during the study period of 20 months (15.9%). Table 2 shows that reinfections were found significantly more often in clients who were notified by a partner (90.0% (9/10) vs 17.7%) (47/256), in clients who reported STI-related symptoms (53.7% (22/41) vs 14.3% (33/231)) and in clients who had three or more partners in the last 6 months (40.4% (21/52) vs 15.7% (35/223)) (at T1). In multivariate analyses, STI-related symptoms (PR 3.2, 95% CI 1.8 to 5.6) and being notified by a partner (PR 5.3, 95% CI 2.4 to 11.5) were characteristics at T1 associated with chlamydia reinfection.
We also analysed whether factors at T0 were predictive of having a reinfection at retest. No significant associations were found.
Comparison of the study group and the historical control group
The historical control group consisted of 1530 young heterosexual people, diagnosed with urogenital chlamydia in 2011, at the STI clinics participating in our study. The study group was compared with the historical group in age, gender and number of partners in the last 6 months. Gender differed significantly between the groups (39.1% (598/1530) men in the control group vs 27.5% (56/228) in the study group, p<0.05); no differences were found in age and number of partners between the groups. Within a period of 20 months, 547 of the 1530 infected (35.7%) returned for a retest, without receiving a text message reminder. When including all retests of our study group (not only the retests that met the definition of a retest in our study), a total of 404 participants out of 828 (48.4%) returned for a retest within 20 months.
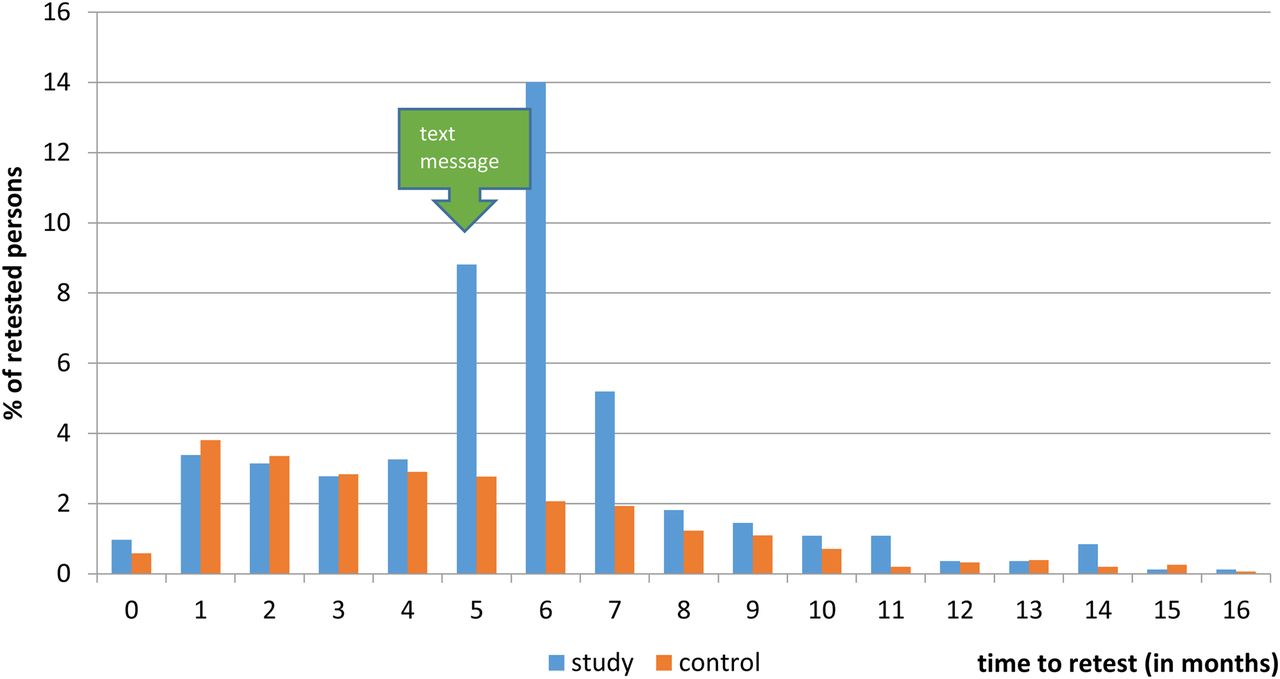
Figure 2 identifies a peak in the retest rate of the study group within 2 months after the text message (5.5 months after the initial positive chlamydia test). Retesting in the study group was concentrated in 5–8-month period, when 253 of 828 (30.6%) participants returned. This contrasts with 140 of the 1530 (9.2%) clients in the control group who returned on their own initiative within the same time frame.

{kind=link}
{kind=link}
Comparison of the monthly proportions of initial chlamydia-positive young clients who returned for a retest within the study group (2012–2013) and the control group (2011) in 10 participating sexually transmitted infection clinics in the Netherlands.
Discussion
In this study, we found that 30.6% (253/828) of the participants responded to the text message reminder by requesting a retest within the period of 5–8 months after initial positive testing. Only 9.2% (140/1530) of the historical control group returned for a retest, on their own initiative, between 5 and 8 months after initially testing positive.
Among the participants, 20.4% (56/275) were found to be chlamydia positive after retest, while the overall chlamydia positivity among all eligible visitors of the STI clinic during the study period of 20 months was 15.9%. Participants displaying STI-related symptoms at retest were more likely to have a chlamydia infection when retested, as were participants who were notified by a partner.
Strengths and limitations
This is the first study in the Netherlands to use a text message reminder system to trigger participants to request a retest. One recent Dutch study on retesting was performed in a more urban setting and made use of a home-based test or a walk-in retest drop off to stimulate retesting.10 However, this is the first multicentre study which incorporates the predominant rural areas, and uses a text message reminder to stimulate retesting.
The reasons for non-participation in the study were not recorded. It cannot be excluded that some of the chlamydia-positive clients were not offered the chance to participate in the study, due to time constraints during the STI consultation, direct treatment before diagnosis or because the client was not a local resident or (small minority) had no mobile phone. The number of clients participating in the study might have been higher if there was no time constraint during the consultation or if no direct treatment was given.
Although we had T0 data for participants who did not return for a retest, we do not have further details regarding their decision not to return for a retest. This information may provide valuable insight to explain over-representation or under-representation of a certain group in the retest population. Also, we do not have data on changed mobile phone numbers as a reason for not receiving the text message and reattending. It may have also been informative to ask additional questions at retest, that is: ‘Has your steady partner been tested and treated for chlamydia?’ or ‘Have you visited a general practitioner in the mean time?’ Questions like these could have clarified reasoning for participation in retesting and for testing positive again upon retest.
There is evidence that there is a frequent intermittent positive pattern of chlamydia test results over time after Azithromycin treatment. This positive pattern was more frequent in anorectal samples. In our study, we excluded clients with an (concurrent) anorectal chlamydia. Follow-up in these studies was performed up to only 8 weeks after treatment, while the current study retested participants after 6 months. Also, it remains unclear whether these intermittent positive patterns of chlamydia after treatment are a risk for transmission.11 ,12 Therefore, treatment failure is unlikely to have played a major role in the current study.
Comparison with other studies
Our results show that a text message, sent at 5.5 and 6 months after the initial consultation, increases participation in retesting from 9.2% in our historical control group to 30.6% in our study group. These findings confirm results of previous studies.13–15 However, a study in the UK concluded that sending a text message did not increase the retest rate after 4 months.16 This was justified by the fact that there already was a high retest rate in the control group, who did not receive a text message (35%, n=92/226), compared with the study group, who did receive a text message (32%, n=89/274). The retest rate of our historical control group isn't already high like the UK study; therefore, we cannot compare our study with the UK study.
The result indicating that young women are more likely to participate in retesting than men is also in line with other studies.9 ,10 It is worrisome that, at retest, men were more often reinfected with chlamydia than women, indicating that reinfection in men may be missed. We, therefore, recommend extra effort to motivate the male population to participate in retesting.
We do not have a clear explanation for the finding that participants who were not notified for an STI during the first consultation were more likely to return for a retest, compared with those who were notified. It may be the case that these participants do not feel that there is a need for retesting since they were not notified before retest. Also, persons who were notified at T0 could be more eager to join the study, because they are worried after being notified. It is imperative to highlight the importance of retesting in chlamydia-positive young people, even if they are not notified.
At inclusion, participants were informed that, even when they did not engage in sex between the testing moments, they should still return for a retest after 6 months. In our study, nine participants reported not having had sex in the last 6 months, before retest, and none of them were reinfected with chlamydia. Though sexual history may not always be reliable, our study concludes that we must focus our attention on individuals displaying STI symptoms and/or those notified by a partner. Having STI-related symptoms and being notified were clear factors associated with reinfection in the current study. This finding concurs with other studies.3 ,5 ,10 ,17 ,18
In our study group, 22 participants reported having STI-related symptoms. A majority of these participants (n=13) returned before receiving a text message (data not shown), probably as a result of the symptoms. The other nine participants responded to the text message and did not attend for a retest on their own initiative. This shows that despite own initiative retesting, text reminders are necessary and can improve retest rates. Therefore, young people who previously tested positive for chlamydia infection should receive specific instructions that they are at risk for reinfection and should reattend for testing, particularly if they notice symptoms.
Interpretation
Despite the limitations, this study and other studies conclude that young people with chlamydia are at risk for reinfection and that it is important to retest them and preferably remind them of the retest.3 ,5 ,10 ,17 ,18 This study has been performed within a standard care environment, complying with the criteria for access to free STI care at STI clinics in the Netherlands, simplifying potential future implementation. If we were to implement sending a text message as a reminder of a retest as a standardised method of triggering chlamydia-positive young people, this would require little time investment and direct treatment at first consultation would not be an issue.
Higher retest participation can also be accomplished by other means; a recent Dutch study showed that by offering a home-based test or a retest at the STI clinic without making an appointment, recipients were more likely to respond to a retest offer (46% and 23%, respectively).10 However, the costs and efforts required for home-based testing are higher than simply sending a text message and the retest rate for the group that could retest without making an appointment is lower than in the current study.
The way the clients prefer to be reminded of a retest may vary and depends on the resources of the STI clinic if it is possible to offer different methods of reminders.
While sending reminders is an important method for increasing retest attendance and subsequently track and treat clients with a chlamydia reinfection, it is at least as important to put a lot of effort into motivating clients to use a condom to prevent reinfection. Sexual health education and motivational interviewing during first consultation can be effective methods in achieving future condom use.19 ,20
Conclusions
Reinfections of previously chlamydia-positive young people are common; therefore, retesting is recommended. Despite the fact that these young people retest on their own initiative, this study shows that sending text message reminders can improve retest rates. The text message reminders should especially be targeted at those at highest risk for reinfection; individuals experiencing STI-related symptoms and/or individuals who are notified for an STI by a partner. When we retest individuals at risk for reinfection timely, it may substantially reduce further spreading of chlamydia due to early case finding. Sending a text message is a small effort and feasible manner to remind people of taking a retest rather than relying on people's own initiative to retest.
Key messages
Sending a text message is an effective approach to remind chlamydia-positive young heterosexuals attending a sexually transmitted infection (STI) clinic of a retest 6 months later.
At retest, 20% (56/275) of young heterosexual participants were reinfected with chlamydia, while the overall prevalence of chlamydia during the study period was 16%.
Young individuals with STI-related symptoms and/or individuals who are notified for an STI by a partner are at higher risk for chlamydia reinfection.
Acknowledgments
We would like to thank Joyce de Goede, epidemiologist of GGD Hart van Brabant, for giving the study a kick-start and drafting the research proposal. We would also like to thank the research group ‘SOROZ’, especially Hanna Bos, who helped setting up the research and solving practical problems. Our thanks go out to all the medical staff of the 10 participating STI clinics for their efforts in motivating all potential participants. Lastly, we would like to thank Linda Howson for revising this article and adjusting the English language.
References
Supplementary materials
Abstract in Dutch
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Abstract in Dutch - Online abstract
Footnotes
Handling editor Jackie A Cassell
Twitter Follow Carolina Kampman at @karlijnkampman
Contributors CJGK has drafted the research protocol, performed data collection and contacts with the working field, performed the statistical analysis, drafted the article and processed comments made by the other authors. FDHK performed the statistical analysis and commented on the article. HCMD-H performed data collection and contacts with the working field for two specific counties and also made corrections to the article. JLAH commented on the research protocol, gave assistance to data analysis, guided the way to the medical ethical committee and commented on the article. IVFvdB assisted data analysis, performed the data analysis of the historical control group and also commented on the article. All authors gave their final approval on the final original article to be published.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The medical ethical committee of the Radboudumc University Medical Centre approved the study (nr: 2012096, 2012).
Provenance and peer review Not commissioned; externally peer reviewed.