Article Text

Abstract
Background Untreated sexually transmitted infections (STIs) and bacterial vaginosis (BV) cause genital inflammation and increase the risk of HIV infection. WHO-recommended syndromic STI and BV management is severely limited as many women with asymptomatic infections go untreated. The purpose of this cross-sectional study was to evaluate genital cytokine profiles as a biomarker of STIs and BV to identify women with asymptomatic, treatable infections.
Methods Concentrations of 42 cytokines in cervicovaginal lavages from 227 HIV-uninfected women were measured using Luminex. All women were screened for BV by microscopy and STIs using molecular assays. Multivariate analyses were used to identify cytokine profiles associated with STIs/BV.
Results A multivariate profile of seven cytokines (interleukin (IL)-1α, IL-1β, tumour necrosis factor-β, IL-4, fractalkine, macrophage-derived chemokine, and interferon-γ) most accurately predicted the presence of a treatable genital condition, with 77% classification accuracy and 75% cross-validation accuracy (sensitivity 72%; specificity 81%, positive predictive value (PPV) 86%, negative predictive value (NPV) 64%). Concomitant increased IL-1β and decreased IP-10 concentrations predicted the presence of a treatable genital condition without a substantial reduction in predictive value (sensitivity 77%, specificity 72%, PPV 82% and NPV 65%), correctly classifying 75% of the women. This approach performed substantially better than clinical signs (sensitivity 19%, specificity 92%, PPV 79% and NPV 40%).
Conclusions Supplementing syndromic management with an assessment of IL-1β and IP-10 as biomarkers of genital inflammation may improve STI/BV management for women, enabling more effective treatment of asymptomatic infections and potentially reducing their risk of HIV infection.
- BACTERIAL VAGINOSIS
- WOMEN
- DIAGNOSIS
- GENITAL TRACT INFECT
- INFLAMMATION
Statistics from Altmetric.com
Introduction
The prevalence of sexually transmitted infections (STIs) and bacterial vaginosis (BV) in developing countries is unacceptably high, particularly in populations at the highest risk of HIV infection.1 ,2 STIs and BV cause genital inflammation2 that potentially facilitates HIV infection by recruiting HIV target cells,3 ,4 promoting HIV replication5 and reducing epithelial barrier integrity.6 Johnson et al7 estimated that ∼50% of new HIV infections in South African women were attributable to other STIs in 2010.
In resource-limited settings, STIs and BV are managed syndromically, according to the presence of clinical signs and symptoms, rather than by more costly laboratory-based diagnosis.8 However, a large proportion of women with STIs or BV are asymptomatic and are thus left untreated.2 ,9 Women with asymptomatic STIs have comparable levels of genital inflammation to symptomatic women, which are elevated compared with women without an STI or BV.2 Previously, we found that women with chlamydia or gonorrhoea, who were mostly asymptomatic, had the highest genital cytokine concentrations, while women with BV had upregulated proinflammatory cytokines but downregulated chemokines and haematopoietic cytokines.10 Many women in resource-limited settings are thus likely to have STI-related inflammation that remains unresolved, placing them at increased risk of HIV infection and reproductive complications.11 There is an urgent need to improve STI management for women in resource-limited settings to identify asymptomatic infections more effectively.
Laboratory-based nucleic acid amplification tests (NAATs) are the gold standard for STI diagnosis. Compared with syndromic management, NAATs are costly and require experienced laboratory personnel and specialised equipment, which are often lacking in resource-limited settings.8 In addition, these tests do not offer immediate results and transmission of STIs or acquisition of HIV may occur while patients await results. Patients often do not return to the clinic for treatment, with return rates as low as 37% in some studies.12 Rapid point-of-care (POC) tests have been under development for several years. A rapid test for chlamydia with moderate sensitivity (63%) would result in more patients being treated than a laboratory test with a sensitivity of 94%, if the return rate were less than 65%.13 However, several antigen-detecting rapid tests for STIs have yielded inconsistent predictive value.14–18 POC NAATs for Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis have been developed and show comparable predictive value to laboratory NAATs.19 ,20 Currently, however, POC NAATs are likely too expensive for implementation in resource-limited settings.
Measurement of inflammatory cytokine biomarkers in genital secretions using a rapid test may prove useful to identify women with asymptomatic STIs or BV, providing immediate results. The aim of this study was to evaluate the predictive value of potential genital cytokine biomarkers of STIs or BV.
Methods
Study participants
This study included 227 HIV-uninfected women from Durban, South Africa.2 ,10 In addition, to validate this approach in HIV-infected individuals, 38 HIV-infected women from Durban were included.21 Women provided informed consent, and this study was approved by the University of KwaZulu-Natal and University of Cape Town Faculty of Health Sciences Human Research Ethics Committees (UCT REC REF: 025/2004).
Screening for STIs and BV
A gynaecological examination was performed and swabs were collected from the anterior and posterior fornices and lateral vaginal walls.2 Specimens were screened for discharge-causing STIs (C. trachomatis, N. gonorrhoeae, Mycoplasma genitalium, T. vaginalis) and herpes simplex virus (HSV) by PCR and BV using Nugent's criteria.2 Blood was screened for IgG antibodies to HSV-2 gG-2 using ELISA (HerpeSelect, Focus Diagnostics, USA). Treponema pallidum exposure was detected using Becton Dickinson Macro-Vue Rapid Plasma Reagin card and haemagglutination tests (ImmuTrep TPHA, Omega Diagnostics, UK). As HSV and T. pallidum have long periods of latency, during which time they would likely be undetectable in the genital tract by PCR or inflammatory biomarkers, except in the case of asymptomatic HSV shedding, an inflammatory biomarkers tool would not be a good strategy to manage these infections, as it would likely miss women who do not have primary infection, reactivated infection or are not shedding HSV at the time. Therefore, we aimed to identify women with treatable, discharge-causing conditions (BV, T. vaginalis, C. trachomatis, M. genitalium, N. gonorrhoeae).
Cytokine measurements
Cervicovaginal lavages (CVLs) were collected using 10 ml sterile saline, centrifuged and supernatants stored at −80°C.2 CVLs were not collected from menstruating participants. The concentrations of 42 cytokines were measured using human cytokine LINCOplex kits (LINCO Research, USA): Epidermal growth factor, eotaxin/CCL11, fibroblast growth factor-2, fms-like tyrosine kinase-3 ligand, fractalkine/CX3CL1, granulocyte colony stimulating factor, granulocyte macrophage colony stimulating factor, growth-related oncogene family (CXCL1-CXCL3), interferon (IFN)-α, IFN-γ, interleukin (IL)-1α, IL-1β, IL-1Ra, IL-2, IL-3, IL-4, IL-5, IL-6, IL-7, IL-8/CXCL8, IL-9, IL-10, IL-12p40, IL-12p70, IL-13, IL-15, IL-17, IFN-γ-induced protein 10 (IP-10)/CXCL10, monocyte chemotactic protein (MCP-1)/CCL2, MCP-3/CCL7, macrophage-derived chemokine (MDC)/CCL22, macrophage inflammatory protein (MIP-1α)/CCL3, MIP-1β/CCL4, platelet-derived growth factor (PDGF)-AA, PDGF-AB/BB, RANTES/CCL5, sCD40L, soluble IL-2 receptor α, transforming growth factor-α, tumour necrosis factor (TNF)-α, TNF-β, and vascular endothelial growth factor. Cytokine lower limits of detection ranged between 0.01 and 27.65 pg/mL. The data were collected using a Bio-Plex Suspension Array Reader (Bio-Rad Laboratories Inc, USA). The cytokines identified as the best biomarkers of STIs/BV were also measured in the same samples from HIV-uninfected women using Human Inflammation and Chemokine Cytometric Bead Array (CBA) kits (BD Biosciences, USA). Cytokine concentrations below the lower limit of detection were reported as the mid-point between the lowest concentrations measured and zero.
Y-chromosome amplification
DNA was extracted from CVL pellets using the Roche MagNAPure LC DNA Isolation Kit I (Roche Applied Science, Indianapolis, Indiana, USA). A region of the TSPY1 gene on the Y-chromosome was amplified using real-time qPCR (PrimerDesign Ltd, UK) and a Roche LightCycler 480 (Roche Diagnostics, Switzerland).
Statistical analysis
Statistical analyses were performed using STATA (StataCorp, USA) and Matlab (Mathworks, USA). Nonparametric receiver operating characteristic (ROC) curves were used to compare the predictive values of each cytokine. Logistic regression was used to determine the variables that were together most predictive of the presence of an STI/BV. Youden's index was used to determine appropriate cutoffs for each cytokine, assuming that sensitivity and specificity are of equal importance. Partial least squares discriminant analysis (PLSDA)22 was used to determine cytokine profiles that best distinguished between individuals with and without an STI/BV. The data were normalised with mean centring and variance scaling. Cross-validation was performed by iteratively excluding random subsets of data during model calibration, and using excluded data to test model predictions. To identify the optimal minimum biomarker profile for STI/BV diagnosis and reduce the risk of over-fitting, the least absolute shrinkage and selection operator (LASSO) method for regression and shrinkage was used.23
Results
Description of study participants
Fifty-three percent of the 227 HIV-uninfected women had BV and 29% were PCR positive for a treatable discharge-causing STI (C. trachomatis, N. gonorrhoeae, M. genitalium, T. vaginalis). Despite the high prevalence of STIs and BV, only 34/227 women (15%) had visible cervicovaginal discharge and none had genital ulceration (table 1).
Demographic and clinical characteristics of women participating in study
Genital cytokine profiles identify HIV-uninfected women with BV and/or treatable discharge-causing STIs
A PLSDA model including all 42 cytokines distinguished between women with an STI or BV and women without STIs/BV with 78% classification accuracy, and 74% cross-validation accuracy (figure 1A). Women with an STI/BV clustered in the positive region of latent variable 1 (LV1; figure 1A), indicating their cytokine profiles were characterised by upregulation of cytokines positively loaded on LV1, and comparative downregulation of cytokines loaded negatively onto LV1 (figure 1B). The model of all 42 cytokines classified women with 74% sensitivity, 80% specificity, 86% positive predictive value (PPV) and 65% negative predictive values (NPV; table 2).
Genital cytokine concentrations as biomarkers of STIs and BV in HIV-uninfected and HIV-infected women

Identification of multivariate cytokine profiles associated with sexually transmitted infections and bacterial vaginosis (STIs/BV). A) Partial least squares discriminant analysis (PLSDA) model of all 42 cytokines classified individuals with 78% overall accuracy for classification and 74% accuracy for cross-validation (light blue: women with a STI/BV; dark blue: women with no STI/BV). B) Latent variable cytokine loadings indicate multivariate cytokines associated with STIs/BV. Since individuals with an STI/BV cluster in the positive region of LV1 (A), cytokines positively loaded on LV1 (B) are elevated in STI/BV profiles, while negative loadings are comparatively reduced. (C) To avoid over-fitting, the Least Absolute Shrinkage and Selection Operator (LASSO) method for feature selection was used to eliminate cytokines that didn't contribute to classification, and resulted in a profile of seven cytokines that performed with 77% classification accuracy and 75% cross-validation accuracy. (D) Loadings in the reduced model indicated that the STI/BV profile consists of elevated interleukin (IL)-1β, IL-1α, and tumour necrosis factor (TNF)-β, with comparatively reduced interferon (IFN)-γ, IL-4, macrophage-derived chemokine (MDC) and fractalkine.
We then used LASSO to eliminate cytokines that did not significantly contribute to group classification. A profile of seven cytokines remained, that classified with similar predictive strength (table 2: 77% classification accuracy, 72% sensitivity, 81% specificity, 86% PPV and 64% NPV), and slightly better cross-validation accuracy compared with the model including all cytokines (75%; figure 1C). In this reduced model, TNF-β, IL-1α and IL-1β elevation with comparative reduction in IFN-γ, IL-4, MDC and fractalkine was associated with the STI/BV group (figure 1D).
IL-1β and IP-10 are predictive of BV and treatable discharge-causing STIs in HIV-uninfected women
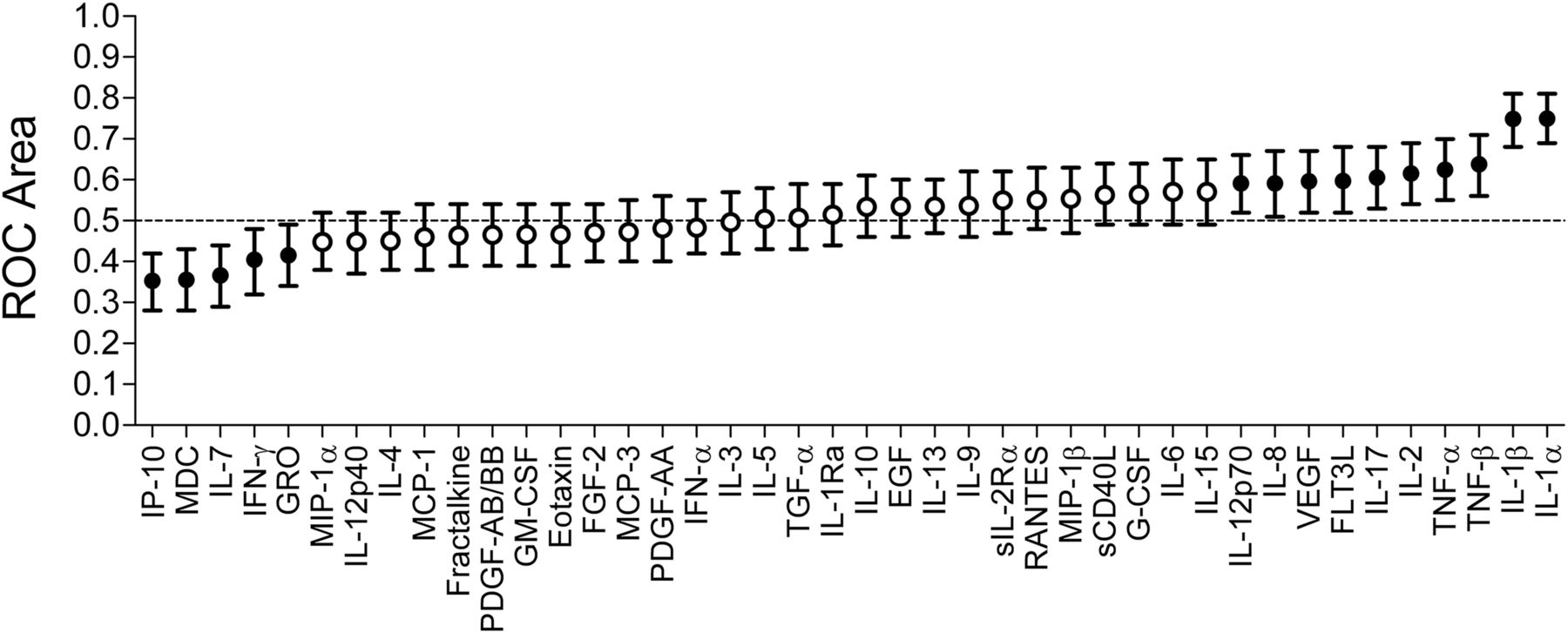
As a diagnostic test including seven biomarkers may be too expensive for implementation in resource-limited settings, we evaluated whether it would be possible to decrease the number of biomarkers included, without a substantial reduction in predictive value. The predictive value of each of the 42 cytokines was evaluated individually using nonparametric ROC analysis (figure 2). IL-1α and IL-1β had the largest ROC areas, indicating that these cytokines had the highest predictive power. Of the cytokines that were inversely associated with the presence of an STI or BV, IP-10 had the best predictive power. It was found that a marginally higher percentage of women were correctly classified using IL-1β (70.5%; cutoff ≥−0.37 log10 pg/mL) compared with IL-1α (69.6%; cutoff ≥1.96 log10 pg/mL) and IP-10 (63.9%; cutoff <1.30 log10 pg/mL; online supplementary figure S1).
{kind=link}
{kind=link}
Genital cytokine concentrations predict the presence of sexually transmitted infections (STIs) and bacterial vaginosis (BV). Receiver Operating Characteristic (ROC) areas for each of the cytokines is shown. Cytokines with a ROC area of 0.5 have no predictive value. Cytokines with a ROC area >0.5 are positively associated with the presence of an STI or BV, whereas cytokines with a ROC area <0.5 are inversely associated. Cytokines indicated by dots were found to be significantly associated with the presence of a treatable discharge-causing STI or BV, whereas those indicated by circles were not significantly associated.
To determine whether inclusion of a second cytokine would improve the predictive value of IL-1β, each of the other 41 cytokines was stepwise added to IL-1β using a logistic regression model building procedure. A model including IL-1β and IP-10 was best predictive of the presence of an STI/BV, correctly classifying 75% of women with a sensitivity of 77%, specificity of 72%, PPV of 82% and NPV of 65% (table 2). Inclusion of a third cytokine, IL-1α, correctly classified 76% of women (sensitivity 72%, specificity 81%, PPV 86% and NPV 64%) and significantly improved the fit of the model (likelihood ratio (LR) χ2: 14.61, p=0.0001); however, this represented only a marginal improvement compared with IL-1β and IP-10 alone.
Upon evaluation of model performance by reapplication of the model to 10 randomly chosen three-quarter subsets of the cohort, 72–80% of women were correctly classified. Furthermore, the relationships between IL-1β and IP-10 and the presence of an STI/BV remained statistically significant and the directionality of the relationships remained constant, indicating that the model estimates are stable and that the biomarkers had similar accuracy in each subset. To evaluate whether the method of cytokine measurement influenced the results, IL-1β and IP-10 concentrations were measured using CBA (table 2). The predictive value of IL-1β and IP-10 was similar when these cytokines were measured using CBA (sensitivity 83%, specificity 61%, PPV 78%, NPV 69%; table 2), compared with Luminex.
To determine whether the predictive value of IL-1β and IP-10 was influenced by age, injectable contraceptive use, yeast and seminal fluid, which may influence genital cytokine concentrations,24–27 each factor was added to the model. It was found that age (LR χ2: 0.55, p=0.4601), injectable contraceptive use (LR χ2: 0.15, p=0.6945), yeast infections (LR χ2: 1.71, p=0.1912) or seminal plasma exposure (LR χ2: 2.93, p=0.0869) did not significantly influence the fit of the model. Although the number of casual sexual partners during the past 3 months was not associated with IL-1β or IP-10 concentrations, inclusion in the model marginally improved the fit (LR χ2: 5.53, p=0.0187).
Using the IL-1β and IP-10 model, 100% of women with M. genitalium, 90% of women with chlamydia, 77% of women with gonorrhoea and 70% of women with trichomoniasis were identified. Of the 24 women who did not have an STI/BV but were incorrectly classified as positive, 38% (9/24) had intermediate flora, compared with 13% of women in the whole cohort (30/227) (p=0.0048). This indicates that intermediate flora may have caused altered cytokine concentrations in some women. However, the inclusion of women with intermediate flora did not influence the predictive value of the model (sensitivity 74%, specificity 78%, PPV 89%, NPV 56%). Of the 33 women who had a STI/BV but were incorrectly classified as negative, most (31/33; 94%) had trichomoniasis or BV, which were previously found to be less inflammatory.10 One of the remaining women had chlamydia, the other had gonorrhoea and two of the women with trichomoniasis also had gonorrhoea.
Comparing cytokine biomarkers with clinical signs of an STI or BV
IL-1β and IP-10 biomarkers were found to predict the presence of an STI or BV with substantially better sensitivity compared with clinical signs (sensitivity 19%, specificity 92%, PPV 79%, NPV 40%). Although addition of clinical signs to the IL-1β and IP-10 model significantly improved the fit (LR χ2: 6.66, p=0.0099), the percentage of women correctly classified remained unchanged (75% (sensitivity 74%, specificity 78%, PPV 86% and NPV 64%)).
IL-1β and IP-10 are predictive of BV and treatable discharge-causing STIs in HIV-infected women
As the HIV status of women using a cytokine test for STIs and BV may not necessarily be known, it is important that these biomarkers are also accurate in HIV-infected women, particularly since STIs and BV are prevalent in these women. Therefore, we investigated whether IL-1β and IP-10 would identify a STI or BV in HIV-infected women (median 6 weeks post-infection).21 IL-1β and IP-10 were found to identify women with a STI or BV with similar sensitivity in HIV-infected women (80%), but improved specificity (100%), compared with HIV-uninfected women (table 2).
Discussion
The pro-inflammatory cytokine IL-1β and the chemokine IP-10 together were the most useful immunologic biomarkers that could be used to diagnose treatable discharge-causing STIs and BV. These biomarkers identified 77% of the HIV-uninfected women who had an STI or BV, while only 19% of these women were identified by clinical signs. Using these cytokines, 75% of HIV-uninfected women were correctly classified as either STI/BV-positive or negative, with a sensitivity of 77%, specificity of 72%, PPV of 82% and NPV of 65%. Similarly, in HIV-infected women, these two biomarkers correctly identified 80% of women with an STI or BV (sensitivity 80%, specificity 100%, PPV 100%, NPV 54%).
The LASSO cytokine model that most accurately classified women as STI/BV-positive or negative included seven cytokines (IL-1α, IL-1β, TNF-β, IL-4, fractalkine, MDC and IFN-γ), correctly classifying 77% of HIV-uninfected women (sensitivity 72%, specificity 81%, PPV 86% and NPV 64%). However, as reducing this model to only two cytokines, IL-1β and IP-10, only decreased the percentage of women correctly classified by 2%, the expense of including five additional biomarkers would likely outweigh the benefit. We thus propose that IL-1β in combination with IP-10 would be the most cost-effective biomarkers for a rapid POC test for identifying asymptomatic discharge-causing STIs and BV. IL-1β upregulation predicted the presence of an STI/BV, while IP-10 was inversely associated. This is because IL-1β was significantly upregulated in women with BV or an STI, while IP-10 was downregulated in women who had BV.10 IL-1β allowed for identification of women with high levels of genital inflammation, while IP-10 differentiated women with BV who had more moderate levels of inflammation.
Following the identification of women using IL-1β and IP-10, the approach implemented in the clinical setting would likely depend on resource availability. In regions where resources are not limited, women identified may be referred for comprehensive laboratory STI/BV testing. In resource-limited settings, where this may not be feasible because of the expense of laboratory testing, women with a positive cytokine POC test result could be offered immediate treatment using the same antibiotics offered to women with vaginal discharge (WHO syndromic management guidelines). Immediate treatment of these women, in the absence of aetiological diagnoses, does raise concern about possible overtreatment. However, cytokine biomarkers predicted the presence of an STI/BV with marginally higher PPVs (fewer false positives) than clinical signs, suggesting that an inflammation biomarker test would not result in increased overtreatment rates compared with syndromic management. In this study, probability cutoffs were set objectively using Youden's index. In practice, cytokine concentration cutoffs would depend on the strategy used to manage the women identified as having inflammation. Should all women identified be referred for laboratory STI/BV testing, one may wish to optimise the sensitivity by adjusting the absolute concentration cutoffs, whereas should women identified be immediately treated with antibiotics, optimisation of the specificity would reduce overtreatment.
As only common STIs and BV were evaluated, women who were “falsely” classified as positive may have had inflammation caused by other infections, including human papillomavirus, Schistosoma, Fusobacterium, Aerococcus, Sneathia, Gemella, Mobiluncus and Prevotella and other potentially inflammatory microorganisms that are not necessarily detected by the laboratory methods used in this study.28–30 Only one woman who did not have a treatable discharge-causing STI or BV was HSV PCR+ and none had a T. pallidum rapid plasma reagin >1:4 with a positive Treponema pallidum haemagglutination (TPHA) test; therefore, these infections were not the cause of the majority of false-positive results in this cohort. Although reactivation of HSV or T. pallidum, or HSV shedding, may contribute to false-positive results in other cohorts, these infections may be accompanied by genital ulcers and condylomata lata, respectively, which can be managed syndromically8 and women who have syphilis can be identified using an existing T. pallidum rapid test. We found that age, yeast infections, semen exposure and injectable hormone contraception, each previously shown to influence genital cytokine concentrations,24–27 did not influence the predictive value of the cytokine model. A limitation of this study was that we did not evaluate the impact of douching, the use of anti-inflammatories, antibiotics or antiretrovirals, menstrual cycle phase, pregnancy, cervical ectopy and vaginal practices. Although we found that IL-1β and IP-10 performed well in separate cohorts of HIV-uninfected and HIV-infected women, it would be important to evaluate these biomarkers in a cohort of both HIV-infected and uninfected women, as HIV infection may influence genital cytokine concentrations and HIV status of women using the test may not necessarily be known. Women who had an STI or BV, but were classified as negative using IL-1β and IP-10 biomarkers were not identified because they had low levels of genital inflammation and may have resolving or less severe infections, or may have been recently treated and may have PCR positive results due to the presence of dead organisms. Measurement of inflammatory cytokine biomarkers likely identifies women with severe inflammatory infections who are at the greatest risk of reproductive complications and HIV acquisition.
An inexpensive biomarker rapid test could be used together with the current syndromic management protocol, particularly in resource-limited settings where laboratory diagnosis is not feasible, to increase the number of women treated for genital infections. A reduction in the prevalence of discharge-causing STIs and BV may reduce the incidence of HIV infection and improve reproductive health.
Key messages
Interleukin (IL)-1β and IP-10 concentrations in female genital secretions predicted the presence of a genital condition with 77% sensitivity, 72% specificity, 82% positive predictive value (PPV) and 65% negative predictive value (NPV).
These cytokine biomarkers performed substantially better than clinical signs (sensitivity 19%, specificity 92%, PPV 79% and NPV 40%).
Supplementing syndromic management with an assessment of IL-1β and IP-10 as biomarkers of genital inflammation may improve sexually transmitted infections and bacterial vaginosis management for women.
This strategy may enable more effective treatment of asymptomatic infections and potentially reduce HIV incidence and reproductive complications in women.
Acknowledgments
The authors would like to acknowledge the women enrolled and the clinical members of the Acute Infection Study Team at CAPRISA for their contribution to this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Handling editor Jackie A Cassell
Contributors LM developed the hypothesis, performed the laboratory work, analysed the data and prepared the manuscript; KBA, FL, KM, DAL, LJ and DAL analysed the data and prepared the manuscript; NM, HG and SN performed some laboratory work, analysed the data and contributed to manuscript preparation; QAK and SAK conceptualised the cohort and prepared the manuscript; J-ASP developed the hypothesis, analysed the data and prepared the manuscript.
Ethical approval UCT REC REF: 025/2004; UKZN BREC: E013/04.
Funding This work was supported by a Strategic Health Innovation Partnerships (SHIP) grant from the South African Medical Research Council and grants from the Poliomyelitis Research Foundation (PRF) of South Africa and European and Developing Countries Clinical Trials Partnership (EDCTP). The cohort was supported by grants from the Comprehensive International Program of Research on AIDS (CIPRA) of the Division of AIDS (DAIDS); National Institute of Allergy and infectious Disease (NIAID); National Institutes of Health (NIH) and US Department of Health and Human Services (DHHS) (grant number U19 AI51794). LM was supported by the PRF; South African Medical Research Council (MRC); the Carnegie Corporation; the National Research Foundation (NRF) of South Africa and the UCT Clinical Infectious Diseases Research Initiative/Wellcome Trust.
Competing interests J-ASP and LM, together with the University of Cape Town, have submitted a PCT International Patent application for IP-10 and IL-1α/β use for diagnosing an inflammatory condition in the female genital tract likely caused by an STI or BV (Patent Application No: PCT/IB2014/065740).
Patient consent Obtained.
Ethics approval University of KwaZulu Natal and University of Cape Town Faculty of Health Sciences Human Research Ethics Committees.
Provenance and peer review Not commissioned; externally peer reviewed.