Article Text

Abstract
Objectives In this prospective study, we aimed to determine the distribution of genotypes by multilocus variable number tandem repeat (VNTR) analysis plus analysis of the ompA gene (MLVA-ompA) of rectal Chlamydia trachomatis among men who have sex with men (MSM) attending Brighton Genitourinary Medicine (GUM) Clinic and to examine any correlations with clinical variables, including HIV status, and to isolate rectal C. trachomatis cultures maximising the possibility of obtaining complete genotyping data.
Methods Samples were assigned genotypes by PCR and sequencing of the markers of the MLVA-ompA genotyping system. Rectal C. trachomatis was isolated in cell culture using McCoy cells. Data regarding demographics, HIV status, rectal symptoms and history of sexually transmitted infections, including C. trachomatis, were collected.
Results 1809 MSM attending the clinic between October 2011 and January 2013 took part in the study, 112 (6.2%) of whom had rectal samples that tested positive for C. trachomatis. 85/112 (75.9%) C. trachomatis-positive rectal samples were assigned 66 different genotypes. Two distinct genotype subclusters were identified: subcluster 1 consisted of more HIV-negative men than subcluster 2 (p=0.025), and the MLVA-ompA genotypes in these subclusters reflected this. Isolates were successfully cultured from 37 of the 112 specimens, from which 27 otherwise unobtainable (from direct PCR) MLVA-ompA genotypes were gained.
Conclusions The most prevalent genotypes were G, E and D representing some overlap with the heterosexual distribution in UK. Subcluster 1 consisted of more ‘heterosexual genotypes’ and significantly more HIV-negative men than subcluster 2, associated with ‘MSM genotypes’. There was a higher diversity of C. trachomatis strains among MSM in Brighton than observed in other cities.
- CHLAMYDIA TRACHOMATIS
- SEXUAL BEHAVIOUR
- HIV
- MOLECULAR EPIDEMIOLOGY
- GAY MEN
Statistics from Altmetric.com
Introduction
Rectal Chlamydia trachomatis remains one of the most commonly diagnosed bacterial sexually transmitted infection (STI) among men who have sex with men (MSM) attending GUM clinics in the UK.1 There is strong evidence for the role of rectal STIs as a risk factor in both the acquisition and transmission of HIVW1–3 and routine rectal testing in MSM is recommended in national guidelines.2
Different C. trachomatis strains determine disease outcomes. For example, there is linkage of lymphogranuloma venereum (LGV) strain L2b to proctitis in MSM.3 ,4 The majority of infections occur within transmission networks;5 ,6 therefore, knowledge of different genotypes is useful for mapping transmission within sexual networks and surveillance of emerging trends. In the past two decades, genotyping of C. trachomatis has relied on PCR and sequence analysis of the ompA gene,7–12 but within each ompA genotype, very little variation exists with respect to ompA sequences.6 ,13 ,14 Furthermore, genome sequencing data reveals that ompA must not be relied on solely as a marker for genotyping, as recombination of all or parts of this gene within and between biovars is evident.15 There are now several very highly discriminating multilocus molecular typing systems, including multi locus sequence typing (MLST), for C. trachomatis that allow differentiation and subgrouping of isolates within a genotype.13 ,16 ,17 W4–6 The multilocus variable number tandem repeat (VNTR) analysis plus analysis of the ompA gene (MLVA-ompA) high-resolution genotyping system of Pedersen et al,13 has been successfully evaluated,18 and recent work has shown that the VNTR marker sequences are stable and therefore ideal for genotyping.19 The system consists of short, easy to amplify markers (the longest being part of the ompA gene), which are simple to manipulate and yield a high efficiency return of results as demonstrated in the quoted surveys. It also has an optimal ability to differentiate between genotypes,20 as measured by the Simpson's discriminatory index.13 ,18
The diversity of C. trachomatis in the heterosexual population has already been characterised, and thus the selection of genotypes that form this population are well established and set the baseline of known strains.13 ,21 ,22 Previous work has reported differences in the distribution of C. trachomatis genotypes between heterosexual and MSM populations6 and sexual behaviour factors, social and sexual network movement and tissue tropism may account for these differences.9 According to the current literature, the distribution of genotypes in rectal infections among MSM is dominated by D, G and J.6 W7–10 However, little is known with regards to the more detailed molecular analysis of the C. trachomatis genotypes that inhabit the rectum, although a study in Amsterdam attempted to compare anorectal samples from MSM and women,23 searching for evidence of rectal tropism.
The purpose of our work was to evaluate whether the MLVA-ompA genotyping scheme could be adapted and applied to rectal specimens in a MSM population looking for correlations with clinical variables, including HIV status. A unique and additional aspect of our project was to isolate rectal C. trachomatis in cell culture. This component was included to maximise the possibility of obtaining complete genotyping data and to provide a fully characterisable collection of live rectal C. trachomatis isolates for future studies into tropism in vitro.
The aims of this study were to determine the distribution of C. trachomatis genotypes found in rectal infection in MSM attending a GUM clinic in the UK city of Brighton, to compare this between HIV-positive and HIV-negative men and to examine any clinical correlations with certain genotypes.
Methods
Participants
Participants were men reporting sex with other men, undergoing rectal testing for C. trachomatis at the GUM clinic between October 2011 and January 2013. Males <16 years old were not eligible. Participants could be recruited more than once if the period between consecutive visits was greater than 3 months. If more than one sample was collected from the same patient in less than 3 months (eg, on the same day), one of these was excluded from the study.
Specimen collection and storage
Men were only eligible for our study if they underwent proctoscopy, having direct visualisation of the rectum and swabs taken directly from the rectal mucosa and not sweeping the perianal area on the way in so that the provenance of our specimens as rectal was assured. In addition to the routine nucleic acid amplification test (NAAT) with the BD Probetec assay (Becton-Dickinson, Sparks, Maryland, USA), clinicians took a separate rectal swab (Σ-VCM; Sigma, Poole, UK) for cell culture of C. trachomatis, which was stored at −80°C. If a participant was found to have rectal C. trachomatis on local testing, stored supplementary rectal samples were transported on dry ice to The University of Southampton Molecular Microbiology Group for tissue cell culture and genotyping. Stored specimens from patients subsequently found to be C. trachomatis negative were discarded. All patient identification information was removed, and samples anonymised prior to transport to Southampton.
Patient demographic and clinical data
Data regarding demographics, HIV status and clinical parameters: rectal signs and symptoms, history of unprotected sex in the previous 3 months and history of previous STIs were retrieved from patient case notes and recorded on a Microsoft Excel spreadsheet.
DNA sequence analysis of MLVA-ompA markers and tissue culture of C. trachomatis
Methodological details of DNA extractions from samples, PCR, sequence analysis and tissue culture isolation of C. trachomatis can be found in online supplementary appendix 1.
Statistical methods
Fisher's exact test (using the statistical software package SPSS V.X21) was used for statistical analysis of associations between C. trachomatis subclusters and clinical parameters.
Ethics
This study was approved by Brighton East Research Ethics Committee (REC reference 11/LO/0745).
Results
Participants
A total of 1809 men consented to participate in this study (the clinic tests approximately 3000 MSM for STIs per year), from which 112 C. trachomatis-positive rectal samples were obtained (6.2% positivity for rectal C. trachomatis). Seven of these men also had concurrent urethral C. trachomatis. Complete paired MLVA-ompA genotypes were only obtained for three of these seven participants. These three paired results were: for participant 6, rectal swab: 8.5.5-L2, urine: 8.5.1-E; for participant 50, rectal swab: 3.5.3-G, urine: 3.6a.3-G; for participant 79, rectal swab: 3.6.4-D, urine: 3.6a.4-G. Of the four incomplete paired MLVA-ompA genotypes (where one or more loci were not sequenced), two included individual paired loci, which differed between the rectal swab and urine and therefore these two samples could also represent different MLVA-ompA genotypes.
Mean age of men with rectal C. trachomatis was 39 years (median 40, IQR, 31–46), 104 (93%) were Caucasian and 47 (42%) were HIV positive.
A total of 85/112 (76%) C. trachomatis-positive rectal samples were assigned full MLVA-ompA profiles. All of the other samples had types assigned to at least two markers based on direct patient samples.
Genotypes identified among MSM in Brighton
Among the 85 fully genotyped samples, there were 66 different MLVA-ompA sequence types (table 1).
MLVA-ompA genotypes according to HIV status
The most prevalent ompA genotypes were G, E and D comprising 19.6%, 17.9% and 15.2% of the 112 positive samples, respectively (table 2). There were two D subgroups: D/UW-3Cx and D/IC-CAL8, which comprised of 4.5% and 10.7%, respectively (see online supplementary table S2). The distribution of ompA genotypes from most to least numerous was G, E, D, L2, F/J (both same number of samples) and I (table 2). Column two of table 2 shows the total number of rectal specimens per ompA genotype, and column three shows the number of rectal specimens that were culturable.
Distribution of MLVA-ompA genotypes among Chlamydia trachomatis-positive MSM in Brighton
Six new VNTR repeats were identified in this study (table 3), in addition to those described in Pedersen et al13 and Wang et al.18
New types and variants of the variable number tandem repeats (VNTRs) identified in this study
In most cases, the MLVA types were unique to the ompA genotypes. However, 11 MLVA genotypes were associated with more than one ompA genotype. These MLVA types were 3.2.4, 3.5.2, 3.5.3, 3.6.4, 8.2.4, 8.5.1, 8.5.4, 8.5.5, 8.6.1, 8.6.3 and 8.7.2 (see online supplementary table S2). The MLVA-ompA profile most commonly detected was 8.5.1-E, which was identified in five patients. MLVA type 8.5.1 was also the MLVA type most associated with different ompA genotypes: it was identified in four ompA genotypes. Genotypes H and K were not detected from any of the samples.
Cluster analysis of genotype distribution among MSM in Brighton
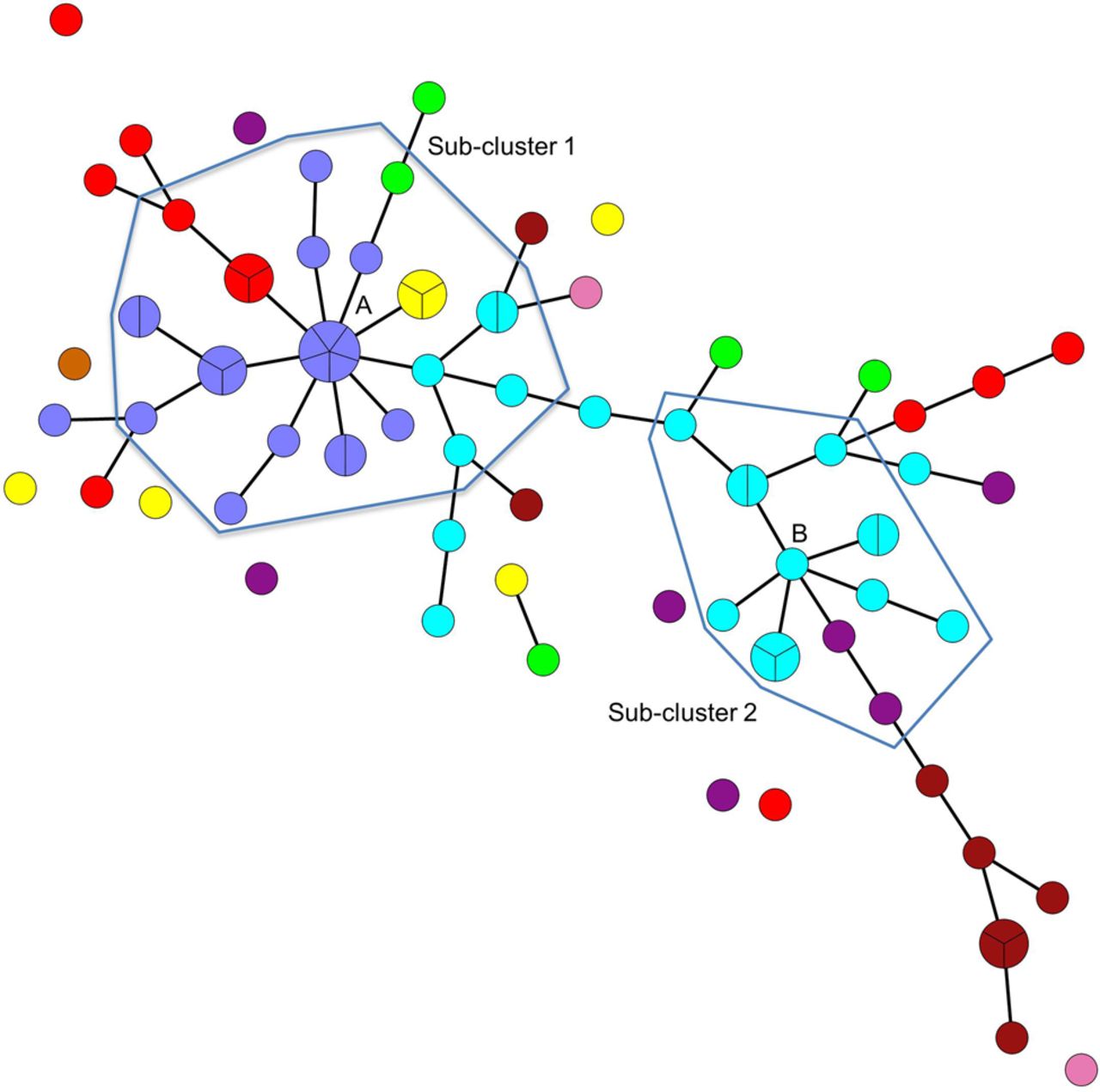
Owing to the variation of genotypes within the highly diverse number of fully genotyped samples in this study (85), it proved necessary to identify possible founder groups within the minimum spanning tree, so as to enable statistical analysis of subclusters. Two possible subclusters were identified (subcluster 1 and subcluster 2, figure 1) on the basis that the putative subcluster founders (A and B, figure 1) had five or more single-locus variants (SLVs) associated with them. Only SLVs and double-locus variants (DLVs) of the subcluster founders A and B were included in further analysis. Statistical analysis using the Fisher's exact test showed a significant difference between the subclusters with respect to HIV status (p=0.025). Most genotypes were from either HIV-positive or HIV-negative MSM (27 genotypes were from HIV-positive MSM only; 32 from HIV-negative MSM only). There were seven genotypes that were found in both HIV-positive and HIV-negative MSM, which were ompA type E (4 genotypes); F (1 genotype); G (1 genotype) and L2b (1 genotype) (table 1). Subcluster 1 consisted predominantly of HIV-negative men and subcluster 2 of HIV-positive men (see also online supplementary figure S2). The distribution of ompA genotypes in subcluster 1 was mainly ompA D, E and F (p<0.001), whereas that in subcluster 2 consisted mostly of ompA G and J (p<0.001), and there were ompA D and L2b genotypes closely associated with this cluster (figure 1). There were seven different MLVA-ompA genotypes among the nine L2bs in this study, five of which were from HIV-positive MSM and four were from HIV-negative MSM. Of the 85 fully genotyped samples, 66 had unique MLVA-ompA genotypes (tables 2 and 3).
{kind=link}
Minimum-spanning tree of 85 men who have sex with men samples from Brighton. Each coloured circle represents a multilocus variable number tandem repeat analysis (MLVA)-ompA genotype. Segmentation within the circles shows the number of samples per genotype, branches show single-locus variants (SLV). Unlinked circles show genotypes, which differ from nearest linked genotype by more than a SLV. Hand-drawn blue lines delineate user-defined subclusters based on founder groups A (subcluster 1) and B (subcluster 2). The circle colour coding shows ompA genotypes as follows: green=D (subtype D/UW-3CX); red=D (subtype D/IC-Cal8); lavender=E; yellow=F; blue=G; light brown=I; purple=J; pink=L2 and dark brown=L2b.
Cultured isolates
Thirty three per cent (37/112) of the samples were successfully isolated in cell culture. The distribution of ompA genotypes among these isolates was as follows: G (n=10), E (n=6), D (n=8) and L2B (n=6) (table 2). MLVA-ompA genotypes 3.4.3-G, 8.5.1-F, 8.7.1-E and 1.9.2-L2b were found in multiple culture-positive samples. In some of these cases (8.5.1-F; 8.7.1-E), genotypes were detected in direct patient samples and post culture (but not from the same patient). Two of the samples with MLVA-ompA genotype 1.9.2-L2b were collected on the same day.
Clinical correlations
There were no significant clinical differences between HIV-positive and HIV-negative men. Overall, 75% of individuals were asymptomatic with regards to rectal symptoms (including pain, bleeding, tenesmus, constipation, diarrhoea, discharge and perianal itch). Individuals with ompA genotype L2/L2b were more likely to be symptomatic (64% of individuals with this genotype were symptomatic) than any of the other ompA genotypes. Further analysis using Fisher's exact test showed that there was no statistical significant differences with respect to rectal symptoms (p=0.725) or signs (p=1.000) and MLVA-ompA genotypes between subclusters 1 and 2.
Discussion
This is the first MLVA-ompA study of C. trachomatis in MSM with HIV. Using this method, we have seen much greater diversity in C. trachomatis genotypes than was expected in comparison with other studies using other genotyping schemes;6 W10 however, there are some trends and significant findings.
Our principle finding in this prospective study is that there are distinct subclusters of chlamydial genotypes for HIV-positive and HIV-negative MSM. We have also observed that the distribution of ompA genotypes among MSM overall differed somewhat from that previously described.6 W10–11 We found that the three predominant ompA genotypes were in descending order: G, E and D, whereas elsewhere studies have shown predominant MSM genotypes to be G, D and J.6 ,24 W10 The Brighton ompA distribution bears a close resemblance to that of MSM in Northern Spain.25
The second most prevalent ompA genotype among our samples was E, which is the predominant ompA genotype among heterosexual individuals. This overlap is further represented by MLVA-ompA genotype 8.5.1-E, the predominant genotype in both this study and a study of Southampton women.18 A unique finding is that this genotype could represent a bridging population between heterosexual females and MSM that could be responsible for the transmission of C. trachomatis between risk groups. Alternatively, this particular genotype may have been introduced to the MSM network some time ago and has since been circulating among predominantly HIV men.
Specifically, while there was no significant symptomatic correlation between HIV-positive and HIV-negative men, there was a trend for individuals with ompA genotypes L2/L2b to be symptomatic compared with those with any other genotype, in keeping with what is already known of the current LGV epidemic in MSM.26 While the initial LGV outbreak was characterised by a painful proctitis and, on fewer occasions, an inguinal syndrome, the number of asymptomatic individuals at that time was low. However, the most recent national LGV case-finding exercise found that 22% of LGV cases were asymptomatic, a quarter of those being presymptomatic, that is, men were asymptomatic at first visit but symptomatic by the time they attended for treatment of rectal chlamydia.27 Despite smaller numbers, our data showed an asymptomatic LGV rate of 36%, slightly higher than the national rate but also consistent with the changing epidemiology of LGV.
In terms of strengths and weaknesses, the sample size was small giving insufficient power to make symptomatic associations with the large diversity of genotypes. Inherent to many epidemiological studies in MSM, the challenges of contact tracing in MSM, who often have multiple and anonymous partners, make obtaining information for complete clusters and sexual networks difficult.
There is some debate over what influences the site of C. trachomatis replication, whether it is tissue tropism or sexual behaviour or both. However, a recent study comparing MLST types of C. trachomatis from women (anorectal, cervical, vaginal and pharyngeal) did not correlate genotypes with these sites.23 Geisler et al28 examined ompA genotypes in women showing that rectal C. trachomatis genotype distribution was similar to that of genital C. trachomatis, notably genotype E. By contrast, genotype G, which was found commonly in the rectums of MSM, was seldom seen at either cervix or rectum in women. From this, it would appear that sexual behaviour factors and epidemiology play a significant role. Another study used whole genome sequencing (WGS) to identify correlations between polymorphisms in specific loci and tissue tropism. Strong associations with rectal tropism were found for polymorphisms in serovar G.29
Of the seven participants from whom we obtained paired samples, five appeared to have different MLVA-ompA genotypes in the rectal compared with urine samples. This suggests that these participants may have been in sexual contact with a wider network.
This is a meaningful study since we have shown that the MLVA-ompA high-resolution genotyping system can be successfully applied to rectal samples in MSM and that the recovery rate of C. trachomatis in cell culture from rectal swabs (33%) was greater than has previously been reported. The implications for clinicians are that different behaviours among HIV-positive and HIV-negative MSM affect coinfections with chlamydial genotypes and are encouraging evidence for serosorting behaviour (a known HIV transmission reduction strategy). Policy-makers should note that paying attention to identification of ‘HIV-positive MSM C. trachomatis genotypes’ can lead to trapping high-risk networks in terms of reducing onward transmission of avoidable deaths from HIV. Implications from our study also indicate that future vaccines for C. trachomatis must encompass all genotypes and cannot be targeted to single groups, such as HIV-positive MSM.
Our second main finding is based on minimum spanning tree analysis and the derivation of two distinct subclusters, suggestive of two separate sexual networks. Subcluster 1 consisted of more ‘heterosexual’ C. trachomatis genotypes, reinforcing the suggestion that linkages between risk groups exist, whereas subcluster 2 displayed a genotype distribution more typical of that previously seen in MSM. However, these two subclusters are closely related genetically, differing by no more than DLVs, which indicate that there is a circulating pool of closely related strains in a single sexual network, which can only be subdivided into ‘more MSM-like’ and ‘more MSW-like’ subgroups.
Furthermore, subcluster 2 consisted of significantly more HIV-positive men, suggesting that these men choose sexual partners from within risk groups, known as, serosorting. The LGV epidemic over the last 10 years has largely affected HIV-positive men and, within this, a distinct group of men with specific behaviour patterns has been implicated. It follows that other genotypes may also be found in higher rates among HIV-positive individuals, but the fact that they are clinically indistinct from other non-LGV genotypes, being mainly asymptomatic, means that we are less likely to be aware of them. Indeed an alternative explanation would be that HIV-positive individuals, who are immune suppressed, are less able to clear certain types of C. trachomatis.
Further larger studies examining rectal genotypes are needed to enable sexual network mapping. Moreover, similar studies in women will provide useful insight into whether certain C. trachomatis genotypes have a predilection for the rectum because of sexual behaviour factors and tissue tropism.
One unanswered question is whether the 8.5.1-E found in the rectums of MSM is similar or quite different to the 8.5.1-E found in the cervices of women. Further work includes WGS, which will facilitate comparison between 8.5.1-E isolate(s) observed in the current MSM study and the women's study.18 Comparison of total single nucleotide polymorphism differences (SNPs) within the women's 8.5.1-E isolates to those of MSM will reveal if there is a significant difference or not, and therefore support a conclusion as to whether or not the ‘MSM 8.5.1-E’ is the same as the women's ‘heterosexual 8.5.1-E’. While not part of the present study, further work will involve detailed in vitro analysis of the tropism of the cultured rectal isolates.
In conclusion, we have been able to identify an association of MLVA-ompA genotypes with HIV status, and our results indicate a possible network within Brighton defined by HIV status.
Key messages
There is a wide diversity of Chlamydia trachomatis genotypes as defined by multilocus variable number tandem repeat (VNTR) analysis (MLVA)-ompA typing circulating in the men who have sex with men (MSM) population of Brighton.
High-resolution multilocus VNTR analysis—ompA genotyping points to discrimination of subclusters of MSM who are distinguishable by their HIV-status.
Heterosexual genotypes circulate within the MSM community in Brighton, but appear to be more associated with HIV negative MSM.
Acknowledgments
We wish to gratefully acknowledge the help we received from Dr Steve Green (PHE Southampton) in use of the Bionumerics software for construction of figure 1.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
- Data supplement 3 - Online figures
- Data supplement 4 - Online tables
Footnotes
Handling editor Jackie A Cassell
Contributors CL conducted the tissue culture and genotyping, as well as data analysis with PM and SG. SS was involved in the concept of the study and study design with INC and PM, led on running the clinical side of the study, and was involved in writing of all drafts of manuscript and the final version. PM and INC drafted the manuscript with SS. JZ was involved in the running of the study and contributed to the first drafts of the manuscript. AB was involved in running the study from a clinical perspective. INC provided expertise in chlamydial biology, genetics and tissue culture, PM provided public health, Chlamydia trachomatis epidemiology and molecular diagnostics expertise, SG provided statistical analysis.
Funding We acknowledge the financial support from the HPA PhD Fund (reference number 2010/001) for CL.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by Brighton East Research Ethics Committee (11/LO/0745).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We are happy to share data from this study, please contact the corresponding author.