Article Text

Abstract
Objectives Annually, millions of people in sub-Saharan Africa (SSA) receive HIV counselling and testing (HCT), a service designed to inform persons of their HIV status and, if HIV uninfected, reduce HIV acquisition risk. However, the impact of HCT on HIV acquisition has not been systematically evaluated. We conducted a systematic review to assess this relationship in SSA.
Methods We searched for articles from SSA meeting the following criteria: an HIV-uninfected population, HCT as an exposure, longitudinal design and an HIV acquisition endpoint. Three sets of comparisons were assessed and divided into strata: sites receiving HCT versus sites not receiving HCT (Strata A), persons receiving HCT versus persons not receiving HCT (Strata B) and persons receiving couple HCT (cHCT) versus persons receiving individual HCT (Strata C).
Results We reviewed 1635 abstracts; eight met all inclusion criteria. Strata A consisted of one cluster randomised trial with a non-significant trend towards HCT being harmful: incidence rate ratio (IRR): 1.4. Strata B consisted of five observational studies with non-significant unadjusted IRRs from 0.6 to 1.3. Strata C consisted of two studies. Both displayed trends towards cHCT being more protective than individual HCT (IRRs: 0.3–0.5). All studies had at least one design limitation.
Conclusions In spite of intensive scale-up of HCT in SSA, few well-designed studies have assessed the prevention impacts of HCT. The limited body of evidence suggests that individual HCT does not have a consistent impact on HIV acquisition, and cHCT is more protective than individual HCT.
- AFRICA
- HIV
- HIV TESTING
- SYSTEMATIC REVIEWS
Statistics from Altmetric.com
Introduction
In sub-Saharan Africa (SSA), the HIV response has intensified dramatically since 2003, when the President's Emergency Plan for AIDS Relief (PEPFAR) was introduced. HIV counselling and testing (HCT), a gateway for HIV treatment, has been brought to scale with tens of millions of annual tests.1–4 Individual and couple HCT (cHCT) are essential for linking HIV-infected persons to HIV treatment, which reduces morbidity, mortality and horizontal and vertical transmissibility.5 ,6 Similarly, individual and cHCT can now serve as referral points for HIV-uninfected men to access medical male circumcision, and, in the near future, may serve as an entry point for antiretroviral pre-exposure prophylaxis.7–9 However, historically, individual and cHCT relied strictly on behavioural HIV prevention messages. The relationship between individual and cHCT and HIV acquisition is not well understood, in spite of three decades of implementation. Given the high volume of HCT, the high proportion of negative test results and the slow scale-up of biomedical prevention, understanding the impact of individual and cHCT on HIV acquisition is essential for guiding the magnitude and nature of future HCT rollout, as well as the relative emphasis of individual and cHCT.
Individual HCT typically consists of three components: pretest counselling, HIV testing and post-test counselling.10 Typically, in pretest counselling, HIV natural history and modes of transmission are explained, as well as behavioural HIV prevention measures. In pretest counselling, the counselling is tailored to the client's personal risk factors. Currently, HIV testing is conducted with rapid tests with real-time results, but historically HIV testing was laboratory based, with results becoming available days or weeks later. Post-test counselling typically involves return of results with differentiated messages for HIV-infected and HIV-uninfected clients. For HIV-infected clients, the discussion is focused on care and treatment, psychosocial support and methods for preventing onward HIV transmission. For HIV-uninfected clients, messages address HIV acquisition through partner reduction, condom use and faithfulness to one partner.
cHCT is an approach in which two members of a couple undergo HCT together, enabling both persons to learn their own status and their partner's HIV status simultaneously. cHCT allows for a couple diagnosis: both persons HIV uninfected (HIV concordant negative), both persons HIV infected (HIV concordant positive) or one HIV infected and the other HIV uninfected (HIV discordant). Counselling messages are tailored around the couples’ HIV status. In both individual and cHCT models, testing can be client or provider initiated, opt-in or opt-out and based in the clinic, home, workplace or community.
Several reviews have explored the relationship between HCT and sexual behaviour in SSA.11–15 They find that there is a strong and consistent increase in condom uptake among persons learning they are HIV infected. This effect is even stronger in cHCT, especially for HIV-discordant couples. However, the effect of HCT on sexual behaviour among HIV-uninfected persons who test alone is inconsistent.
Assessment of the impact of HCT on HIV acquisition is needed, as behaviours are imperfect proxies for HIV acquisition. Sexual behaviour is based on self-report, which can be biased from inaccurate recall and social desirability. Even accurate self-report may not perfectly predict HIV acquisition. Consistent condom use is associated with substantial reductions, but not elimination, of acquisition risk.16–20 Similarly, questions about condom use or number of partners may mask certain behaviours, such as serosorting or selecting partners perceived to be less risky. Thus, direct estimates of the effect of HCT on HIV acquisition are necessary.
We conducted a systematic review to assess the impact of HCT on HIV acquisition among HIV-uninfected persons in SSA. Specifically, we reviewed articles comparing (A) sites that offered full HCT with sites that did not, (B) persons who received HCT with persons who did not and (C) persons who received HCT individually with those who received HCT as a couple. We also assessed the quality of each article, including research design and analysis.
Methods
In this review, we sought to systematically identify all published articles from SSA that assessed the impact of HCT on HIV acquisition. HCT was defined as a process that included pretest counselling, HIV testing and post-test counselling, including return of test results. Persons who tested, but did not receive their results were classified as not having received HCT. Articles were included if they met the following search criteria:
Conducted in SSA
Evaluated the impact of HCT among HIV-uninfected persons
Had a longitudinal study design
Had an HIV acquisition endpoint
Compared settings that provided HCT with settings that did not (Strata A), compared persons who were exposed to HCT with persons who were not (Strata B) or compared cHCT ewith individual HCT (Strata C).
Further restrictions were not made based on the nature of HCT or on methodological criteria, such as study design or analytic methods.
On 9 August 2013, PubMed and PsychINFO were searched using the following search terms: “HIV AND (acquisition OR incidence) AND testing AND counselling” to identify abstracts for review. Date of publication was not an inclusion criterion. A trained research assistant screened all abstracts and identified those that potentially met review criteria. Ambiguous abstracts, such as those that reported HIV acquisition in only one subgroup, were included at this stage. These abstracts were then screened by an epidemiologist, and when necessary the full manuscripts were reviewed. Reference lists of included manuscripts were reviewed for additional articles that potentially met inclusion criteria. These additional articles were screened using the same procedures. Duplicates were removed.
Information on the study settings, populations, study designs, intervention and comparison and HIV acquisition measures was abstracted. Setting attributes included country, year of data collection and whether HCT was workplace, community, home or clinic based. Population characteristics included age, gender and risk groups, such as general population or key populations (eg, sex workers, men who have sex with men or injection drug users).
Study designs were classified as randomised, pre/post or exposed/unexposed cohorts. Pre/post comparisons applied to persons who initially did not receive HCT and later did receive HCT. Exposed/unexposed comparisons compared persons who received HCT with those who did not receive HCT. Measures of HIV incidence were abstracted from articles as incidence rate ratios (IRRs) and/or hazard ratios (HRs) and 95% confidence intervals (CIs). Crude, adjusted and inverse probability weighted effect measures were reported separately. When multiple subpopulations or types of analyses were included, each was reported separately. When available, subpopulation effect measures were also reported. If the original authors had not calculated these measures, but sufficient information was available, we conducted these calculations using Open Epi (http://www.OpenEpi.com).
Information on study quality and bias was abstracted as well. To assess the possibility of exposure misclassification, we assessed whether HCT status was ascertained via self-report or from clinical or study records. The number of times HCT status was ascertained was also assessed. To explore the possibility of confounding, we abstracted adjustment variables, including whether sexual risk behaviours were included. To assess the possibility of selection bias, the proportion of eligible persons who participated and the proportion of participants who were retained were abstracted. To determine the amount of information each study was contributing, the number of seroconversion events was abstracted.
Study characteristics were entered into a Microsoft Access database. Two trained research assistants reviewed each article independently. The two databases were compared for consistency by the epidemiologist, who adjudicated discrepancies. She reread all articles to validate all information in the final database.
Meta-analysis was not conducted because the studies were heterogeneous in terms of populations, study designs, effect measures and nature of HCT. Therefore, all assessments are descriptive. Our review procedures were not registered.
Results
The PubMed search yielded 1622 abstracts and the PsychINFO search yielded eight abstracts. Of these abstracts, 53 were identified as potentially eligible based on the abstracts and 12 were reviewed in their entirety. One was excluded as it reported on a duplicate cohort, four were excluded for lacking a comparison population, incidence information or both and seven met all inclusion criteria. Five additional articles were identified for review from the reference lists. Of these, two were reviewed in their entirety. One was excluded for lacking a longitudinal design and one met all inclusion criteria. In total, there were eight articles included in the review (figure 1). Of these eight articles, one was in Strata A, a comparison of sites with and without HCT,21 five were in Strata B, comparisons of individuals who received HCT with those who did not22–26 and two were in Strata C, comparisons of individuals who received individual HCT with those who received cHCT.27 ,28
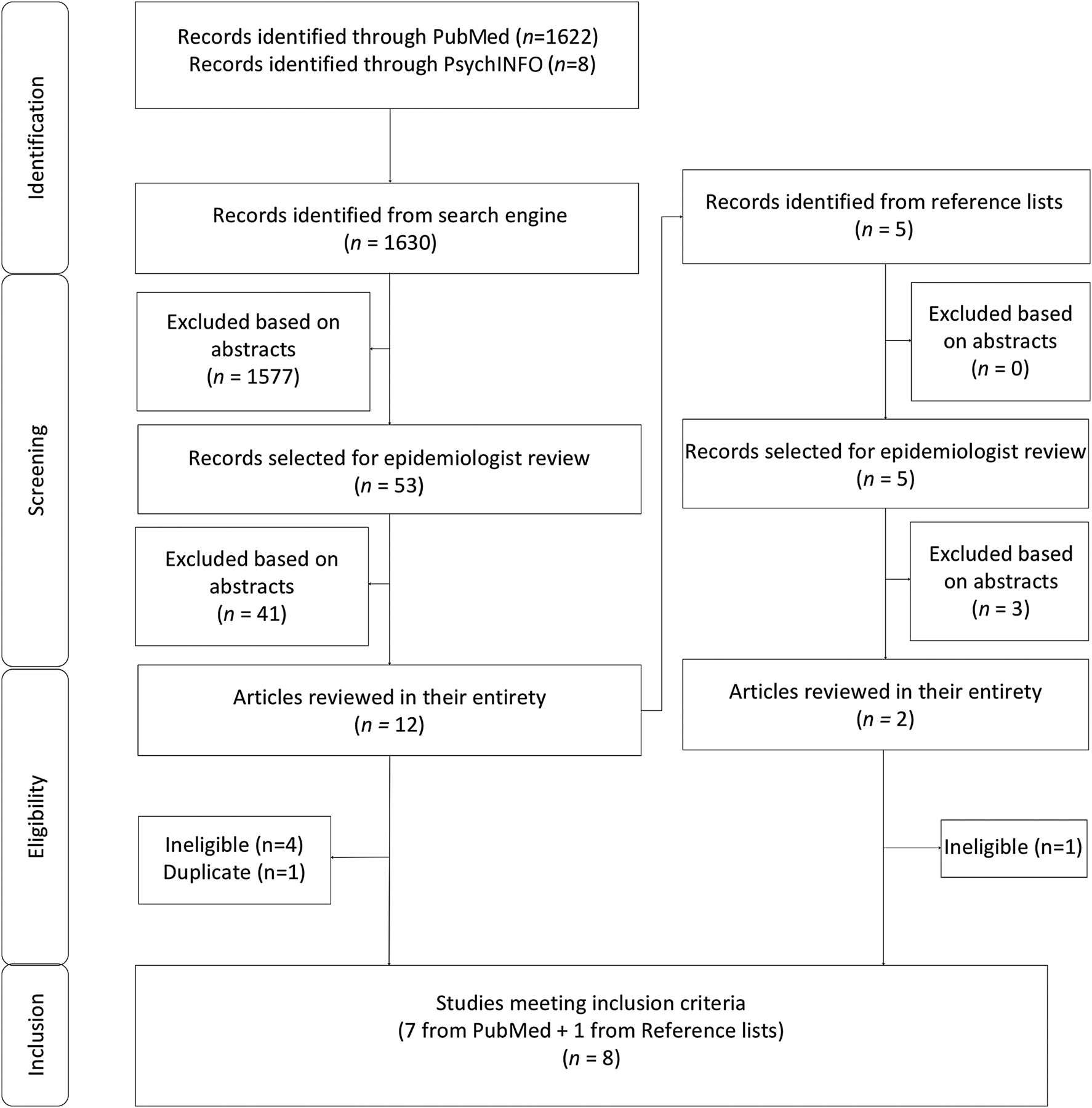
{kind=link}
This consort diagram depicts the steps in the search process, including article identification, screening, eligibility, and inclusion.
Settings and populations
Six articles relied on data collected before the introduction of PEPFAR in 2003,21 ,22 ,24–26 ,28 and two relied on data collected after this period23 ,27 (table 1). Studies were conducted in Uganda,22 ,24 ,27 Rwanda,28 Zimbabwe21 ,25 ,26 and South Africa.23 Data were ascertained from five home-based settings,22–25 ,27 two workplace settings21 ,26 and one clinical setting.28 No studies were conducted exclusively among injecting drug users, sex workers or men who have sex with men. All were conducted among the general population with most HIV acquisition risk presumed to be through heterosexual contact. The workplace-based studies were conducted predominantly among men,21 ,26 the home-based studies were conducted among men and women22–25 ,27 and the clinical study was conducted among women attending antenatal or paediatric services.28 One study was restricted to youth 15–24 years old,23 and the rest were conducted in a broader range of adult ages with minimum ages of 13–18 years and maximum ages of 35 to >60 years. In all studies, HCT and cHTC were conducted by trained counsellors.
Study characteristics
Strata A
The assessment in Strata A was a two-arm cluster randomised controlled trial conducted in Zimbabwean workplaces from 2002 to 2004. In both intervention and control sites, participants received pretest counselling at their own workplaces. In the intervention sites, persons were also able to receive HIV test results and post-test counselling at their workplaces, whereas in the control sites, persons received a voucher to off-site nearby clinics, a less convenient approach. These different approaches led to different uptake of HIV test results and post-test counselling: 5% in the control sites and 71% in interventions sites, resulting in HCT-exposed and HCT-unexposed groups in the intention-to-treat analysis. There were modest differences in the mean HIV incidence in the intervention (1.37 per 100 person years) and control sites (0.95 per 100 person years) for an intention-to-treat IRR of 1.44 (95% CI 0.77 to 2.71) (table 2). In the per protocol analysis, the IRR was closer to the null: 1.34 (0.88 to 2.06). Sixty-one seroconversion events were observed (table 3). Approximately two-thirds of eligible persons participated and, of these, approximately two-thirds were retained.
Study results
Study quality
Strata B
Five studies were included from Strata B. Two of these studies were conducted in Zimbabwe (1993–1995 and 1998–2003), two in Uganda (1994–non-specified and 1999–2000) and one in South Africa (2006–2011) (table 1). All were observational. Four were conducted in homes in enumerated population-based household surveys and one was conducted in a workplace setting. One study had a pre/post design,26 three had exposed/unexposed designs22 ,24 ,25 and one had both.23
HIV incidence rates in the full populations ranged from 1.522 ,24 to 3.526 per 100 person years. In the full populations comparing those who received HCT with those who did not, unadjusted IRRs ranged from 0.63 to 1.28 with all CIs containing the null.22–26 In analyses disaggregated by gender, unadjusted IRRs among females ranged from 0.98 to 1.50 and unadjusted IRRs among males ranged from 0.63 to 1.40; none were statistically significant. Only one assessment adjusted for sexual behaviour, and in this analysis HCT was found to be protective with a HR of 0.65.23 This study also used inverse probability weights to account for confounding and in this analysis HCT was found to be protective with a HR of 0.59. In one study in which IRRs were disaggregated based on number of partners, there was a non-significant trend towards HCT being protective among those with more than one partner (IRR: 0.50) but not among those with only one partner (IRR: 1.16).22
All studies had methodological limitations. None of these studies were randomised. Three did not account for confounding,24–26 one accounted for confounding in subanalyses only22 and one accounted for confounding in the main analysis.23 Participation rates were between 75% and 80% in the two studies that reported this figure.24 ,25 Retention rates were 60–85% in the three studies that reported this figure.24–26 One retrospective study had sufficient information to include 54% of persons, with at least one baseline and follow-up endpoint.23 In three studies, HCT status was ascertained based on study or clinic records,22 ,24 ,26 and in two studies it was based on self-report.23 ,25 Studies had between 36 and 248 seroconversion events.
Strata C: cHCT versus individual HCT
Two studies were identified within Strata C. The first was conducted in Rwanda from 1988 to 1990 among women presenting for antenatal and paediatric care at an urban hospital.28 The second was conducted in Uganda from 2006 to 2008 as part of a home-based HCT programme.27 From these two studies, four IRRs were abstracted. In Rwanda, one assessment compared HIV-uninfected women before cHCT and after cHCT (pre/post). A second compared HIV-uninfected women who received HCT alone with HIV-uninfected women who received HCT with a partner (unexposed/exposed). In both comparisons, there was a trend towards cHCT being protective: pre–post IRR: 0.44 (95% CI 0.14 to 1.22); unexposed–exposed IRR: 0.53 (95% CI 0.18 to 1.32). In Uganda, HIV acquisition was compared between HIV-uninfected persons who tested individually with those who tested with a partner. Overall, testing with a partner was significantly protective: 0.31 (95% CI 0.19 to 0.48), with a stronger trend among females than males.
Combined these two studies had 135 seroconversion events. Incidence was 2.7 per 100 person years among HIV-discordant couples in Rwanda. Incidence was 0.5 per 100 person years among HIV-negative persons in unknown-status couples in Uganda. Neither study was randomised and neither adjusted for sexual behaviour. In both studies, the participation rates were not stated.
Discussion
In spite of the rapid and substantial expansion of HCT in the SSA, there are few assessments of the impact of HCT on HIV acquisition, and, to our knowledge, these few assessments have not been synthesised previously. Based on this small body of evidence, two key trends emerge. First, individual HCT does not consistently increase or decrease HIV acquisition risk. Second, cHCT reduces HIV acquisition risk by approximately half compared with individual HCT. These findings must be interpreted cautiously and within a broader context, as this body of evidence is modest with imprecise estimates and possibilities of bias.
In all unadjusted analyses, when comparing those receiving HCT with those not receiving HCT, all results were close to the null and imprecise. These observations are consistent with comparable assessments in SSA and other parts of the world. Project Accept, a large cluster randomised controlled trial in SSA and Asia, comparing areas of widespread community-based HCT with more limited clinic-based HCT, found no difference in HIV incidence at a community level.29 In Western settings, among men who have sex with men, HCT has not been associated with decreased risk, especially among those who test repeatedly.30
HIV-uninfected persons testing as a couple were less likely to acquire HIV than persons testing alone, a finding consistent with other evidence and models in the region. In an assessment in Uganda and Kenya, couples receiving cHCT had substantially lower HIV incidence than historical controls.31 Similarly, HIV-uninfected women in HIV-discordant couples who tested with their partners had lower HIV acquisition than HIV-uninfected women who tested alone, when assumptions were introduced about the proportion of HIV-uninfected women who were in HIV-discordant relationships.32 These findings are consistent with a mathematical model suggesting that the scale-up of cHCT could reduce HIV incidence in Zambia and Rwanda by 35–60%.33
Our findings are also consistent with assessments of the behavioural impacts of HCT in SSA. Individual HCT is associated with modest behaviour change in some HIV-uninfected populations, but not others.11 However, cHCT is consistently and strongly associated with uptake of consistent condom use, especially in HIV-discordant couples, with meta-analysed ORs in excess of 60.12–14 ,34 ,35 The greater effectiveness of cHCT is likely due to the importance of dyadic interventions for sexual activities which are dyadic behaviours.36–38 Regardless of why, promoting cHCT over individual HCT is a key policy implication. Although the WHO has endorsed cHCT for the region, it remains the exception, not the norm. Several strategies, such as partner notification and community invitations have been effective for increasing cHCT and could have important implications if brought to scale.39–41 Such efforts would have benefits on reduced HIV incidence and on reaching global HIV targets, including the 90–90–90 goals and elimination of mother-to-child transmission42–44
Assessing the impact of HCT on HIV acquisition is methodologically challenging. First, all assessments of HIV acquisition require large cohorts followed for long periods with low, non-differential loss to follow-up. These longitudinal studies are time consuming and expensive. Second, the impact of HCT on HIV acquisition cannot be assessed in randomised settings; deliberate withholding of HCT is unethical due to the incontrovertible benefits for HIV-infected persons. As a result, observational designs are typically employed, but these are less rigorous, especially without controlling for confounders. A third challenge is that both the primary exposure (HCT) and the primary outcome (HIV acquisition) require an HIV test. Thus, it is necessary to have independent ascertainment methods for establishing HCT (the exposure) and acquisition (the outcome). In some studies, the exposure is based on self-report, making it subject to information bias. In some assessments, persons refuse to provide blood for outcome ascertainment, introducing potential bias.
In light of these methodological challenges, this body of literature is small and methodologically weak. Only eight articles are included with fewer than 1000 seroconversion events, providing a limited foundation for drawing conclusions. Furthermore, all studies have important limitations. The study in Strata A was randomised at the cluster level. However, participation and retention were moderate, with possibilities for selection bias. All assessments in Strata B and Strata C were non-randomised, and most did not control for key confounders: sexual behaviour and pregnancy. In the study that did control for these factors, HCT had no effect on HIV acquisition in unadjusted analysis but was protective in adjusted analysis.23 This difference suggests that those who received HCT were at higher risk for HIV than those who did not; HCT helped lower the risk of testers (a higher risk population) to a level similar to that of non-testers (a lower risk population). It is not clear whether similar effects would have been observed, had other strata B studies controlled for these variables.
Integrating new biomedical advances into HCT is an important direction for future HCT programming. Most of these studies were conducted in the 1990s and early 2000s, prior to the findings that medical male circumcision and pre-exposure prophylaxis can be effective at reducing HIV acquisition rates among HIV-uninfected persons.7–9 ,45–48 As such, HCT in these studies was focused on behavioural prevention messages. To enhance its effectiveness, HCT can be used as a platform for providing referrals for biomedical prevention.
HCT with simple behavioural messages, when offered to HIV-uninfected persons without their sexual partners, is insufficient to consistently and substantially prevent HIV acquisition. However, HCT, when offered to HIV-infected persons, is critical for treatment initiation and subsequent reductions in transmissibility. Considering the effects of HCT on both HIV-uninfected and HIV-infected persons, HCT scale-up must continue. However, to maximise the prevention impacts, a paradigm shift towards cHCT is needed, along with improved linkages to biomedical prevention for those who are HIV uninfected and at high risk of HIV acquisition.
Key messages
In spite of intensive scale-up of HIV counselling and testing (HCT) in sub-Saharan Africa, a few well-designed studies have assessed the prevention impacts of HCT.
Individual HCT is neither consistently protective nor harmful.
Couple HCT (cHCT) is more protective than individual HCT.
Interventions beyond HCT are needed for substantial declines in HIV acquisition, including cHCT.
References
Footnotes
Contributors NER conceptualised the study in collaboration with WCM. BH conducted the search and reviewed all abstracts. BH and JR reviewed and coded all full articles; NER adjudicated discrepancies. NER and BH wrote the first draft. All authors provided substantive edits to the manuscript and approved the final draft.
Funding National Institute of Mental Health (K99MH104154-01A1), National Institute of Allergy and Infectious Diseases (P30 AI50410), Fogarty International Center (R25 TW009340).
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.