Article Text

Abstract
Objectives In recent years, the internet has widely facilitated Chlamydia trachomatis home-sampling. In France (2012), the Chlamyweb Study evaluated an intervention (Chlamyweb) involving home-based self-sampling via the internet. One element of the study consisted of a randomised controlled trial (RCT), which is reported in detail elsewhere. The focus of this paper, however, is on describing the Chlamyweb Intervention and reporting on the non-RCT element of the evaluation of that intervention by the Chlamyweb Study. This involves (1) describing the design and roll-out of the Chlamyweb Intervention, (2) comparing the socio-behavioural profiles of the participants in the intervention with a nationally representative general population sample and (3) examining the factors that influence the acceptance and return of a self-sampling kit supplied to participants in the course of the intervention.
Methods Self-sampling kits were offered to sexually active people aged 18–24 years living on the mainland French. Participants' characteristics were compared with the general population to describe recruited and participant populations. Multivariate analyses by conditional logistic regression were performed to determine factors that were predictors of kit acceptation and use.
Results 7215 people aged 18–24 years were included. Compared with the general population, Chlamyweb reached larger proportions of women, younger people and people with several partners in the previous year. 3372 (46.7%) agreed to receive a self-sampling kit and 2084 (61.8%) returned it, with more women doing so than men. The participation rate was associated with age, place of birth, occupational status, number of partners and condom use, differently for men and women.
Conclusion The offer of easy-to-use, self-sampling kits free of charge appeared to be a logistically feasible strategy for testing in France and reached a large and diverse population including individuals who have limited access to the traditional healthcare system.
Trial registration number AFFSAPS n° IDRCB 0211-A01000-41; pre-results.
- CHLAMYDIA TRACHOMATIS
- SCREENING
- INTERVENTION STUDIES
Statistics from Altmetric.com
Introduction
In France, the only national survey studying the prevalence of Chlamydia trachomatis (CT) infection in the general population was conducted in 2006 and it estimated the prevalence to be 3.2% and 2.5% in women and men aged 18–29 years, respectively.1 Unlike other European countries,2 the French national CT control action does not include systematic screening in sexually active young men and women. In 2003, the French National Agency for Accreditation and Evaluation in Healthcare advised to offer systemic screening only to those women aged 15–25 years and those men aged 15–30 years who visit centres where testing is offered anonymously and free of charge such as STI clinics and family planning and education centres.3 It proposed to also develop operational research to study the benefit of self-sampling methods. In the mid-2000s, these were evaluated only in a medical setting and in an epidemiological study1 ,4 (see online supplementary file 1).
supplementary data
Many countries have developed new strategies to increase screening for CT infection,5 particularly outside a clinical setting. The availability of nucleic acid amplification tests, since the late 1990s, and the ability to test urine and self-collected swabs have made this more feasible. Home-based self-sampling via the internet is acceptable and cost-effective if the return rate is as high as the clinic-based screening rate with 6% positivity.6 It is also convenient and easily accessible. It has the potential to reach people who do not otherwise get tested and who were more likely to have several partners and who have not used condoms in the previous year.7 ,8
Based on foreign experiences,9 the French National Institute of Health Education and Prevention (INPES) decided, in 2012, to propose to young people aged 18–24 years home-based self-sampling via the internet through an intervention called Chlamyweb. The aims of this paper are to (1) describe the design and roll-out of the Chlamyweb Intervention, (2) compare the demographic and behaviour profiles of the intervention participants with a nationally representative general population sample and (3) examine the factors that influence the acceptance of a self-screening kit supplied to participants in the intervention.
Methods
Intervention
Between 3 September and 14 October 2012, an online communication campaign was launched on sites via paid advertising, social networks and YouTube. The aim of this campaign was to raise awareness of and encourage young people to visit a website which provided information about CT, testing and treatment and information about other STIs (see online supplementary file 2). The website hosted a questionnaire to assess eligibility for the Chlamyweb Study (including the Chlamyweb Intervention and the linked randomised controlled trial (RCT)) and to gather the sociodemographic and behavioural characteristics of potential participants.
supplementary data
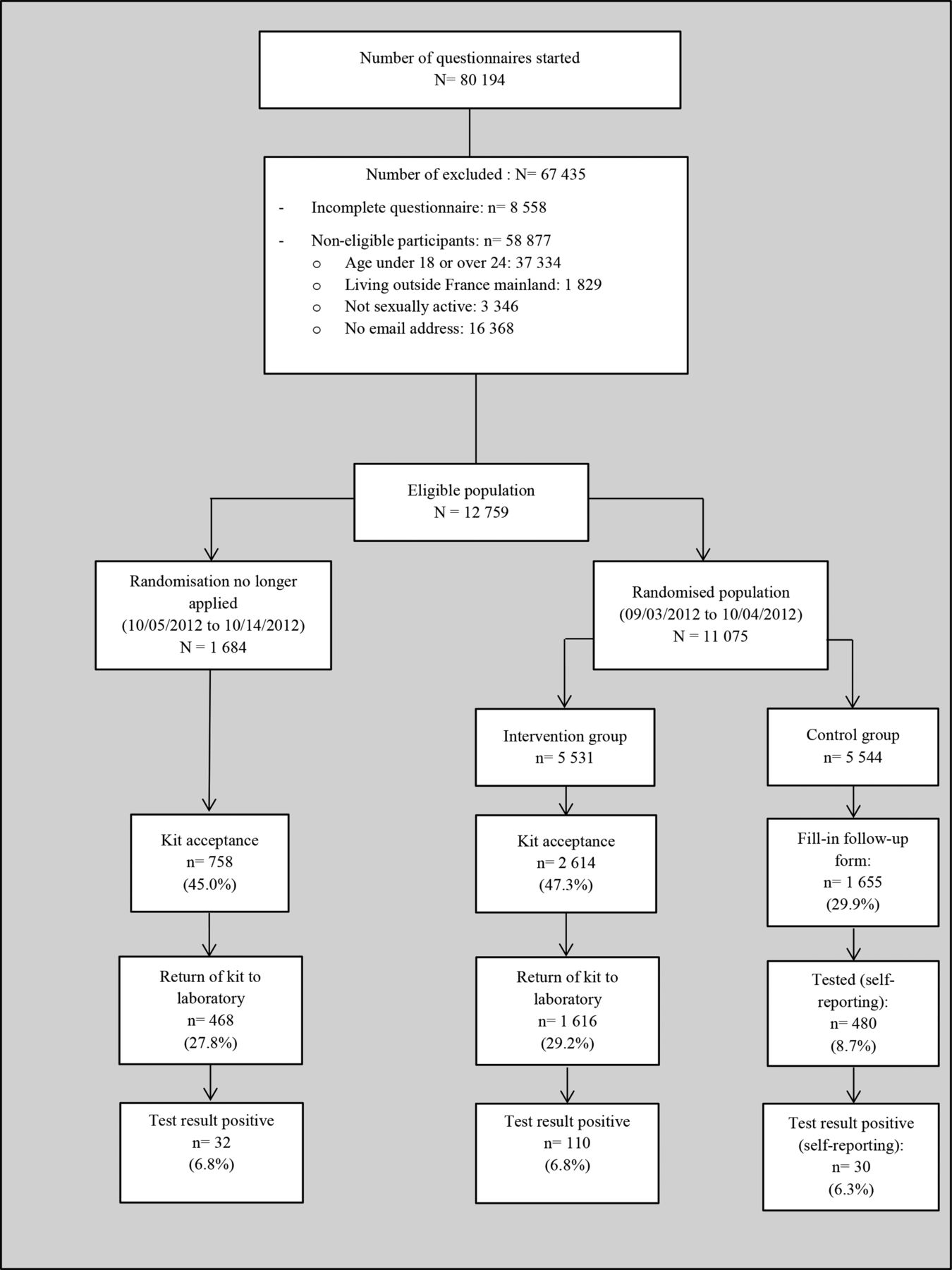
Eligibility criteria for the study include people aged 18–24 years and who are sexually active. Participation in the study involved either engagement in the Chlamyweb Intervention, which was formally marked by the offer of a self-sampling kit, or engagement in the control arm of the linked RCT (of which the results are described in detail elsewhere).10 During the first 4 weeks (from 3 September 2012 to 4 October 2012), participants in the study were randomised to either the intervention or the control arm of the RCT. In the 10 days that followed (from 05 October 2012 to 14 October 2012), randomisation was no longer applied and all study participants were assigned to the intervention. Participation in both the intervention and the RCT element of the study was dependent on the provision by potential participants of a valid email address (because the follow-up of participants was done via email). The relationship between the intervention and the linked RCT is shown in figure 1, along with the numbers of study participants assigned to the intervention, the RCT or both (in the case of the intervention arm of the RCT). The impact in reducing the prevalence of CT is higher when both men and women are screened, therefore, both men and women were included in the study.11
{kind=link}
Flow chart showing Chlamyweb Intervention and its nested randomised controlled trial (France, 2012).
This paper will, from here on, focus on the intervention rather than the study as a whole. It will be concerned exclusively with participants in the intervention (both the larger numbers who were randomised to the intervention in the course of the RCT and the smaller number of non-randomised study participants who were added to the intervention in the final 10 days). It will not, therefore, be concerned with the study participants who were assigned to the control arm of the RCT.
Study participants who were also assigned to the intervention had the choice of agreeing, or not agreeing, to receive the kit. If they agreed to receive the kit, this opened up a form to enter the address of their choice. In cases of refusal, they were sent to a page that provided information on CT. The same procedure was followed for non-eligible people. At any time, the STI helpline ‘Sida Info Service’ could be called free of charge by the participants.
Twice per week, a list of those who had agreed to receive a kit was sent to the logistics coordination team in charge of sending the readymade kits for male and female. An agreement was made with the national postal service to ensure widespread distribution across the country. The package was designed to fit into all postal drop-off points.
The free home self-collection kit included contact, consent form, instructions and materials (see online supplementary file 3). The sampling device included a urine collection device with three sponges for men and dry self-taken vulvovaginal swab for woman (Copan diagnostics). The participant was asked to sign the consent and to choose the terms of the return result (mail or email). After sampling, the kit was returned to the National Reference Centre (NRC) for Chlamydia infection (CNR), Bordeaux, France, in a self-addressed prepaid envelope.
supplementary data
All samples returned to the NRC for Chlamydia were analysed using the fully automated Cobas 4800 CT/Neisseria gonorrhoeae (NG) system (Roche diagnostics) either after suspension of the dry swab in the Cobas transport medium or direct urine. The fully automated Cobas 4800 system incorporates nucleic acid extraction and real-time PCR. An internal control is added to each sample as the first step of automated sample preparation. All samples that could not be tested with the Cobas 4800 system were retested using the Xpert CT/NG assay from CEPHEID.
The NRC for Chlamydia directly informed the participant of the results. If the test for CT was positive, the result was posted, including a letter informing the participant's doctor of the intervention with recommendations for treatment and information for their partner. Negative results were sent to the participant via their chosen delivery method (post or email).
To encourage the return of the kit, two reminders using a simple personal style were scheduled 15 and 25 days after the order date. No incentive was offered. Duplicate email reminders were not sent because studies have shown that after three or four messages, there is no improvement in retention rate12 because participants classify the messages as spam or unwanted mail.13 ,14
Measure
Socio-behavioural data were collected via a self-administered questionnaire at the time of inclusion. Acceptance of the kit was defined by fulfilment of the following two conditions: providing a postal address and ticking the ‘I accept a kit being sent’ box on the online form. The kit was recorded from the moment it was returned to the analytical laboratory.
Seven weeks after registration, each participant received a follow-up questionnaire by email. This questionnaire allowed additional information to be collected: effective outcome of screening, type of organisation consulted and reason for consulting primary care rather than using the kit.
Analyses
Analyses were based on participants in the Chlamyweb Intervention and defined as all those who had a kit offered to them between 3 September and 14 October (n=7215). The characteristics of Chlamyweb participants could be compared with the general population based on information from the 2010 Health Barometer survey15 and knowledge, attitudes, beliefs and practices (KABP) survey 201016 using Pearson's χ2 test. Both of these surveys were conducted by telephone on a representative sample of the population living in metropolitan France. The 2010 Health Barometer interviewed 1210 men and 1264 women aged between 18 and 24 years. The KABP survey interviewed 530 men and 570 women from the same age bracket. An effect size for each test was performed using Cramer's phi (ϕc).17 Significant variables in the univariate analysis were entered into a logistic regression model to determine predictive factors for kit use. Analyses were performed using STATA (V.13; StataCorp Stata Statistical Software: Release 13, College Station, Texas, USA: StataCorp LT, 2013). City size and age were forced in the model as confounding variables. p Values ≤0.05 were considered significant.
Ethical considerations
The Chlamyweb Intervention was approved by the French National Commission for Information Technology and Liberties (CNIL) and a Regional Ethics Committee (CPP). It is registered with a French medical authority (no.°2011-A01000-41).
Available epidemiological data for the general population1 and from specific groups4 ,18 warranted opening the intervention to minors (aged 15–17 years). However, CNIL refused to allow this because in France parents have to provide consent for children <18 years in any scientific research. In our case, it was not possible to verify parental consent online.
Participants were informed of the aim of the intervention and the nature of their participation and were asked to give consent for their participation directly online before starting the questionnaire. They also had to fill a paper consent form within the testing kit and send it back to the laboratory with their sample. Personal information was managed by a third party (BVA) with a secure data network. Data collected by the laboratory on the paper form (name, address and biological results) were managed only by the laboratory. At the end of the study, BVA sent the investigator (INPES) an anonymous database including the kit numbers as well as the sociodemographic and behavioural data. The NRC for Chlamydia had a file with the kit numbers and the biological results. Merging was done using the kit number.
Results
Characteristics of participants
During the 6-week intervention, 7215 participants aged 18–24 years were included, of which 3930 (54.5%) were women. Compared with the general population (table 1), the Chlamyweb Intervention reached a larger proportion of women. Men and women participating in the intervention were more likely to be younger (18–19 years). They were also more likely to be students and live in a town of more than 100 000 inhabitants or in the Paris region. Those born abroad (particularly women from sub-Saharan Africa) were slightly under-represented among the intervention participants. Women and men participating in the intervention were much more likely to report same sex partners during their life and multiple partners in the previous year. For about 30% (vs 12% in the general population), the most recent partner was a casual partner and about two-third (67.5%) reported not having used condoms during their last sexual encounter (vs 81.3% in the general population). Intervention participants have been already tested for CT infection in the same proportion as their counterparts in the general population (around 11% for men and 5% for women).
Comparison of the demographic and behavioural characteristics of the intervention participants relative to the general population aged 18–24 years, by sex
Involvement in the home-based self-sampling process
Of the 7215 participants, 3372 (46.7%) agreed to receive a self-sampling kit, with more women agreeing than men (52.0% vs 40.4%; p<0.001). Of these, 2084 (61.8%) returned the kit with more women doing so than men (63.5% vs 59.2%; p<0.01). Totally, 2084 of the 7215 participants were tested representing an overall rate of 28.9%, which was higher in women (33.1%) than in men (23.9%).
Kits were complete in 99.2% of cases with just four signatures and 11 consent forms missing. Eight consent forms were recovered after a reminder was sent. All samples were consistent apart from two urine samples. An inhibited single sample was observed giving an inhibition rate of <1 out of 2000. Interestingly we observed peak positivity at the first 4 days with 11 positive cases of 52 samples received (21%) (see online supplementary file 5). Out of the 1539 responders to the follow-up questionnaire who used the kit, 87.5% found it very easy to use and 12.4% found it fairly easy without a difference between men and women.
supplementary data
supplementary data
Factors associated with acceptance of the kit
For women, the rate of acceptance of the kit increased with age—rising from 42.5% among women aged 18–19 years to 60.3% for those aged 22–24 years (table 2). The rate was lower for women born in Maghreb or in a sub-Saharan country compared with those born in metropolitan France. It did not vary according to the size of the place of residence. Having had first intercourse before 17 years and not having used a condom during most recent intercourse increased the probability of acceptance of the kit. The number of partners during the past 12 months and having a recent partner (within the past 3 months) were not associated with acceptance of the kit. Finally having consulted a healthcare professional for gynaecological reasons over a year ago increased the probability of acceptance of the kit.
Proportions and factors associated with kit acceptance and with return of kit to laboratory in women
For men, the kit acceptance rate increased with age rising from 33.6% among men aged 18–19 years to 44.8% for those aged 22–24 years (table 3). This rate did not vary according to the country of birth or the size of the place of residence. The rate was lower among men who were seeking employment compared with those who were students. Having had sexual intercourse with a same sex partner and not having used a condom during most recent intercourse increased the probability of acceptance of the kit. The rate was also higher among men who have had two partners or more during the past 12 months (43.6% vs 36.9% for those with a single partner). For both men and women having already been screened for CT infection was not associated with acceptance of the kit.
Proportions and factors associated with kit acceptance and with return of kit to laboratory in men
Factors associated with returning the kit
Women from the Maghreb accepted the kit less frequently and were also less likely to return them. The return rate was also lower among those who had had their first sexual relationship before the age of 17 years even though there were more of them who agreed to receive a kit. Finally, the return rate was more among women who had had only one partner in the year versus those who had had several partners. For men, the only variable associated with the return of the kit was occupational status—those who were on an educational course were more likely to return the kit compared with those who had left the educational system.
Refusal and non-use of the kits
Among the participants, 5131 did not make use of the kit—it was either refused (74.9%; 3843/5131) or accepted but not sent back (25.1%; 1288/5131). Among participants who refused the kit, 17.2% completed the follow-up questionnaire. More than a quarter of them (27.7%) reported having been tested in primary care. Among people who did not return the kit, 24.0% answered the follow-up questionnaire and 17.4% reported having a screening test. A preference for going to a doctor to be screened (44.2%) and a lack of time (11.1%) were the two main reasons for not using the kit.
Use of the support helplines
During the 6 weeks of the intervention, the STI helpline received only nine calls. However, 172 requests were recorded in the dedicated inbox. These mainly concerned answers to reminder emails for returning kits (55%) delays in the delivery of kits (13%) and delays in obtaining results (10%).
Discussion
Statement of principal findings
The offer of easy-to-use, self-sampling kits free of charge appeared to be a logistically feasible strategy and reached a large and diverse population. It was well accepted. Of the eligible participants, 46.7% agreed to receive a home-testing kit and 61.8% returned it, thus representing an overall success rate of 28.9%.
Strengths and weaknesses of the Chlamyweb Study
The high specimen return rates in the Chlamyweb Intervention indicate that the majority of people agreed to provide specimens when approached in their homes. The phase of acceptance is more challenging. Sending out the kit on the prior acceptance of the participant allows for greater efficiency in returning samples. However, in accepting the participant had to understand what they were committing to and be capable of identifying the sender of the message. A more advanced use of the technique such as ‘foot in the door’ increases compliance to a request and ‘priming’ could have increased the acceptance rate and therefore overall participation.19
Chlamyweb attracted a population that was different from the general population in several respects. It was more often younger women and more commonly living in large towns. It contained many students. Conversely, populations originating from abroad were under-represented. This result may be somewhat explained by the different use of the internet in these populations and by their use of the internet to research information about health. In France, in 2010, 70% of people aged 15–85 years reported using internet at least once during the course of the year. This was 96% among the population aged 15–19 years and decreased with age (92% among those aged 20–25 years and 90% among those aged 26–30 years).15 Internet use is also very high among students, with 99% having used it within the past 3 months.20 Several studies have shown that there are fewer women than men who use the internet; however, when they use it, more of them will do so to find health information.21 ,22 When considering those born abroad their use of the internet is less common—both in general and for health-related questions.21
Participants in the Chlamyweb Intervention also had different sexual behaviour indicators from those of the general population. A larger proportion of people with multiple partners and with casual partner for their last intercourse relationship indicate that the population reached by the intervention was more at risk of STIs than the general population. Men reporting same sex partners accepted the kit more commonly than heterosexuals. This could be explained by their greater difficulty in broaching sexual health subjects with their doctors.23
Strengths and weaknesses of the Chlamyweb Study in relation to comparable studies, particularly regarding any differences in results
The return rate is about the same as that reported in a review of the literature including four studies in which the home-sampling kits were requested via the internet or by telephone without prompting.11 Compared with NatChla, a previous French study in 2006 in which the subjects were recruited by telephone, the return rate was the same (28.9%) before telephone or postal reminders.1 Return was lower in men than in women as already described in other previous screening programmes.24 We found that the most at-risk participants accepted the kit most frequently. This is consistent with previous studies in Sweden and in Great Britain.25 ,26
Lessons to be learnt: possible mechanisms and implications for clinicians and policymakers
The results show that the kit acceptance phase is a significant issue and needs specific attention. Working with young people to improve the arguments and the attractiveness of the system could help in the acceptance phase. Enquiries via email highlighted an awareness of the process among the participants. Implementation of a system that allows people to monitor the steps for the kit being sent, the specimens being received by the laboratory and the results being returned would undoubtedly alleviate these concerns. A more personal reminder12 or broadening the channels used to send reminders27 might also improve the specimen return rate. However, our results show that refusing or not returning the kit is not necessarily synonymous with a rejection of the screening process. An important number of these individuals reported having been tested in primary care.
The Chlamyweb Intervention proved particularly well adapted for some subgroups of population: older people; those born in France and those at recent risk of STIs. It also reached individuals who have more difficulties with the traditional healthcare system such as men who have sex with men. For women who had already consulted for gynaecological reasons, the intervention did not act as a replacement for the traditional system but as an additional opportunity to be tested. The intervention was less effective for other groups of interest, such as younger people (aged 18–19 years), those born abroad and young women who had never consulted for gynaecological reasons. Other strategies need to be used here, including for minors who are currently excluded from online systems. General practitioners who are not actively involved in CT screening should take a greater role. The Chlamydia Testing Training in Europe (CATTE) project showed that it was possible to lift barriers to providing CT testing and other appropriate sexual health services by developing training packages for general practice staff.28
All these results have to be considered to define the best system for France. Our analysis should also examine all the components of an effective CT control strategy (treatment partner notification and retesting).
Keys messages
The offer of easy-to-use, self-sampling kits free-of-charge and is a logistically feasible strategy and reached a large and diverse population.
Behavioural factors indicate that population reached by the programme was more at risk of STIs than the general population.
Conducting studies in cyberspace presents challenges to the conventional frameworks in terms of involvement and follow-up.
Acknowledgments
The authors would like to acknowledge the McCann France agency who managed the information website and advertisement and Bérengère Gall and Jean Baptiste Gautherin who assisted in the data collection and data management. They also thank members of the scientific committee who are not authors of this paper for their advice: Josiane Warszawski, Véronique Goulet, Nathalie Spenatto, Carine Favier and all the young people who participated in the study.
References
Supplementary materials
Abstract in French
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Abstract in French - Online abstract
Footnotes
Handling editor Jackie A Cassell
Contributors NL and DK-R designed the study analysed and interpreted data and wrote the article. BdB and CLR collected biological data and performed biological test. LB was responsible for the media campaign. All authors commented on draft version and all approved the final version.
Funding The trial was funded by the French National Institute of Health Education and Prevention (INPES). INPES is funded by the French Ministry of Health and National Health Insurance.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the French National Commission for Information Technology and Liberties and a Regional Ethics Committee (no.2011-12- 04).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data created during this research are available on demand at the Santé publique France. Please contact the corresponding author.