Article Text

Abstract
Objective We aimed to asses if there are differences in the clinical presentation and immune response of repeat as compared with initial syphilis.
Methods Prospective study: we prospectively recruited all patients with a new diagnosis of syphilis and tested their plasma for a range of cytochemokines and rapid plasma reagin (RPR) at baseline pretreatment and 6 months following therapy. Retrospective study: we compared RPR assay response kinetics between initial and repeat syphilis in persons attending our HIV/STI clinic from 1993 to 2016.
Results Prospective study: a total of 91 individuals, 36 with initial syphilis and 55 with repeat syphilis, were included in the study. At baseline visit, those with initial syphilis were more likely to be symptomatic and have higher levels of interleukin-10 than repeaters. At baseline, median RPR titres were higher in the repeat than the initial infection groups. Repeaters were less likely than those with initial infections to serorevert to a negative RPR and be serofast (<4-fold RPR titre decline) at 6 months.
Retrospective study: syphilis was diagnosed in 1027/43 870 individuals tested. At diagnosis, repeaters had higher RPR titres and a stepwise increase in RPR titre with number of syphilis episodes. They had a different RPR test response kinetic: they were less likely to be serofast and to serorevert than initial syphilis at 6 and 12 months. No individuals with four or more previous episodes of syphilis seroreverted.
Conclusion Repeat syphilis has a different clinical presentation and immunological response to initial infection.
- syphilis
- immunology
- epidemiology (clinical)
Statistics from Altmetric.com
Introduction
It seems important to emphasize that patients who have once had syphilis, even though cured in the primary stage, are immunologically never the same.
—Magnuson1
Magnuson came to this conclusion, 50 years ago, based on a study that involved the subcutaneous inoculation of prison volunteers with and without evidence of previous treated syphilis infection with Treponema pallidum subsp. pallidum (T. pallidum).1 The study provided evidence that previous infection attenuated the clinical response to reinfection. All eight of those with no previous syphilis developed dark-field microscopically positive, clinically evident lesions and a serological response. This response only occurred in 9/11 and 1/26 of those with a history of previously treated early and late syphilis, respectively. In those with untreated latent syphilis (LS) (n=8), none developed lesions or a serological response.
As Magnuson appreciated, if syphilis repeat infections present in a different way to initial infections, then this could have important clinical and epidemiological repercussions. If patients with multiple repeat infections are more likely to present with asymptomatic disease, then the diagnosis of syphilis will be wholly dependent on changes in their serological tests—mostly titres of their non-treponemal tests (NTTs).2–4 Because a wide range of factors can result in increases in NTT titres, there is a risk that syphilis will then be overdiagnosed and treated.5 Delayed diagnosis and underdiagnosis are, however, an arguably more important concern. If reinfection syphilis is more likely to be asymptomatic, then affected persons will be less likely to be tested and treated for syphilis than if they were symptomatic.
A number of studies have compared the clinical findings in initial and repeat syphilis and have reached different conclusions. Two studies found that persons with repeat syphilis were more likely than initial syphilis to present with asymptomatic or less symptomatic disease,6 7 and two studies found no difference.3 8 A further study found this difference only in the subgroup of HIV-infected men who have sex with men (MSM).2 The best quality evidence provided by these studies comes from a review of syphilis infections in an HIV-infected cohort in France over an 8-year period. Detailed clinical notes including photographs were kept from each syphilis diagnosis that enabled a more detailed and intraindividual comparison than the other studies could perform.7 In this study, a statistically significant 78% of repeat infections were scored as less symptomatic than initial infections.
Few studies have compared the immunological responses between initial and repeat syphilis. A retrospective cohort review from Baltimore found that persons with prior syphilis had higher geometric mean NTTs than initial infections.8 Two studies have established that initial infections were more likely to serorevert (NTTs return to negative) than repeat infections.9 10 Two previous studies have found that repeat infections had a slower NTT decay curve than initial infections.9 11 The studies were, however, retrospective, small (36 and 48 cases) and were subject to a number of potential confounders.9 Other studies have found no association between previous syphilis and NTT decay curve, but there were methodological shortcomings in these studies.12 13 In one study, for example, it was unknown in 77% of cases if they had had a previous episode of syphilis.12 No studies that we are aware of have assessed if there is a difference in the plasma immunological profile between initial and repeat syphilis episodes. We compared the clinical, chemocytokine and NTT profile of persons with a diagnosis of initial versus repeat syphilis in a prospective observational cohort study. We then validated the finding that repeaters had a different NTT response curve in a retrospective analysis of all syphilis tests performed at our HIV/STI clinic.
Methods
Prospective cohort study
The Institutional Review Board (IRB) of the Institute of Tropical Medicine (ITM), Antwerp, and the Ethics Committee of the University Hospital Antwerp approved this study (13/44/426).14 Between January 2014 and June 2015, all patients attending the HIV/STI clinic, ITM and over the age of 17 years in whom a new diagnosis of syphilis was made were prospectively recruited into the SeTPAT (Search for a Treponema Pallidum Antigen Test) study (ClinicalTrials.gov Registration Number: NCT02059525; see online supplementary file 1 for participant inclusion process). The staging of syphilis was according to the Centers for Disease Control and Prevention classification.14 Stage-appropriate syphilis treatment was administered on the day of diagnosis with either intramuscular benzathine penicillin G or oral dose doxycycline in the case of penicillin allergy or unavailability. Patients were followed up at 3, 6, 9 and 12 months after treatment. In addition, 30 HIV-positive controls attending the same HIV clinic and at the same time as the cases and in whom a diagnosis of syphilis was excluded were recruited.
Serofast syphilis
We defined a serofast response as the failure of the rapid plasma reagin (RPR) titre to decline by fourfold between the baseline and the 6-month visit (6-month serofast) and the 12-month visit (12-month serofast syphilis). Seroreversion at 6 and 12 months was defined as the RPR titre converting to negative at the 6-month or 12-month visit, respectively. Methods describing specimen processing and testing for chemocytokines, HIV viral load and T. pallidum PCR and serological tests are detailed in online supplementary box s1.
Retrospective study
The IRB of the ITM approved this study (IRB/AB/ac/127). We performed a review of all serological syphilis tests carried out for persons attending the HIV/STI clinic at the ITM from 1 October 1993 to 30 September 2016. Syphilis was tested for in persons at risk via a RPR card test (Becton, Dickinson and Company, Sparks, Maryland, USA) and a Treponema pallidum particle agglutination (TPPA) test (Fujirebio, Osaka, Japan). In mid-2013, the TPPA was replaced with the TPA test, a chemiluminescent immunoassay (Ortho-Clinical Diagnostics, Rochester, New York, USA) performed on the Vitros 5600 Integrated System (Ortho-Clinical Diagnostics).
An episode of syphilis was defined as an episode in which a person had an RPR titre of ≥1/4 and a positive TPPA or TPA test on serum. Previous RPR results were not always available and thus the definition also applied to persons who, on their first visit, had a positive TPPA and an RPR titre of ≥1/4. Repeat syphilis, which included syphilis repeat infections and reactivations, was defined as an episode in a person who had a ≥4-fold increase in RPR titre, after a previous diagnosis of syphilis who exhibited an appropriate response to therapy (≥4-fold decrease in RPR).
Statistical analyses
Values are summarised as medians and IQR. In keeping with previous studies, we found that the immunological profiles of syphilis differed between primary and secondary syphilis (PSS) and LS.15 16 Results are therefore presented stratified by clinical stage (PSS vs LS). There is also evidence that the immune profile differs by HIV status, presence of coinfections and HIV viral load.17 We therefore controlled for these in multivariable linear regression models with each of the chemocytokines as outcome variables. Non-normally distributed chemocytokine, HIV viral load, C reactive protein and RPR variables were log or square root transformed as appropriate to achieve normality. Comparison of the interindividual data between groups was performed using the Mann-Whitney U test. Wilcoxon’s signed rank test was used to evaluate intraindividual changes from baseline to repeat syphilis. Associations between categorical variables were assessed with the χ2 test and Fisher’s exact test. χ2 test for trend was used to test for changes over time and successive episodes of syphilis. The differences in the decay of RPR values over time between those with an initial infection and those with a repeat infection are presented graphically. We used Brown et al’s9 model to represent the exponential decay of RPR values over time following treatment. This was done in R V.3.3.2 with the package ‘drc’.18 19 The predicted RPR values were plotted over time stratified by initial RPR value, separately for those with initial and repeat syphilis infections. All other analyses were performed in Stata V.13 (StataCorp). A p value of less than 0.05 was considered statistically significant.
Results
Prospective study population
A total of 91 individuals with a new diagnosis of syphilis and 30 HIV-infected non-syphilis-infected controls were included in the prospective study (see online supplementary figure S1). Only one participant was a woman. All the men with syphilis, excluding one, self-reported as MSM. Fourteen presented with primary, 40 with secondary and 37 with LS of which 25 were early latent and 12 late latent. Seventy-nine (86.8%) were HIV infected, 36 (39.6%) presented with initial infections and 55 with repeat infections (table 1). At baseline, the age, sex, median CD4+ T-cell count, other STIs diagnosed, treatment received and number of sex partners in the prior 12 months did not differ significantly between initial and reinfection groups (table 1). In the PSS but not the LS group, those with reinfection were more likely to be HIV positive (93.1% vs 68.0%, p=0.018). In the LS group, those with initial infections were less likely than repeaters to be on antiretroviral therapy (60% vs 100%, p=0.001) and to have a higher HIV viral load (34 (IQR 10–141 000) vs 10 (IQR 10–10, p=0.023, respectively). Likewise, except for a higher HIV viral load in the controls than the LS repeat infections, there were no significant differences in the age, CD4+ T-cell count or HIV viral load between the controls and the various subgroups.
Baseline characteristics of participants by syphilis stage and initial versus repeat syphilis presentation (prospective study)
Patients with multiple syphilis repeat infections are less likely to be symptomatic
Overall, 25/36 (69.4%) of those with initial infection were symptomatic (table 2). The proportion of those with one previous infection that was symptomatic was similar (22/30 (73.3%)). Fewer of those with two or more previous syphilis infections were symptomatic (8/25 (32.0%) p=0.047). There was a correlation between increasing numbers of previous infections and the probability of an asymptomatic presentation of syphilis (χ2 test for trend: p=0.005, online supplementary table S2).
Baseline plasma chemocytokine and cytokine concentrations in participants by syphilis stage and initial versus repeat syphilis presentation (prospective study)
Repeat infections have an altered immune profile compared with initial infections
Median RPR titres were higher in the repeat than the initial infection groups in those with PS (1/128 (IQR 1/64–1/128) vs 1/64 (IQR 1/16–1/128), p=0.016) and those with LS (1/64 (IQR 1/32–1/128) vs 1/32 (IQR 1/2–1/64), p=0.042). Controlling for a range of confounders, such as HIV status, syphilis stage and HIV viral load, RPR titres remained lower in initial than repeat infections (coefficient −0.44, 95% CI −0.67 to −0.22, p<0.001, table 3).
Multivariable linear regression predicting interleukin-10 (IL-10) and rapid plasma regain (RPR) at baseline visit* (prospective study)
After controlling for HIV status, syphilis stage, HIV viral load and coinfections, having an initial syphilis infection remained significantly positively associated with log interleukin (IL)-10 (coefficient 1.29, 95% CI 0.68 to 1.90, p<0.001); table 3/online supplementary table S3). At the 6-month visit. only log IL-10 remained positively associated with initial infections (coefficient 0.48 (95% CI 0.05 to 0.92), p=0.029, data not shown).
No difference in immune profile between asymptomatic repeat infections and controls
Thirty-seven participants presented with asymptomatic (latent) syphilis at the baseline visit. For 25 of these individuals, this was at least their second episode of syphilis and thus the diagnosis of syphilis was based purely on an increase in NTT titre. In these individuals, there was no significant difference between their immune profile and that of the HIV-infected controls (table 3). In 12/37 individuals, this was their first episode of syphilis and the diagnosis of syphilis was based on a positive treponemal test and a positive NTT. In these 12 individuals, IL-10 was significantly higher than the controls (7.2 (IQR 1.5–17.7) vs 1.5 (IQR 1.5–1.5), p=0.001).
Some asymptomatic repeat infections are PCR positive for syphilis
In a total of 27 patients, T. pallidum DNA was detected using PCR either in the plasma/serum (n=13) or on a skin/mucosal lesion (n=14) at baseline. These cases of confirmed syphilis infection included several cases with pauci-immune responses and three cases of asymptomatic syphilis where the PCR was positive in the serum. Two of these three cases were initial infections, and these had only very mild elevations of IL-10 and macrophage inflammatory protein-1β (online supplementary table S4). The third case was a reinfection who had a marked elevation in a range of cytokines.
A number of cases of PCR positive syphilis had a bland immune profile (participant 1, online supplementary table S2).
Initial infections are more likely than repeat infections to serorevert but remain serofast
Prospective cohort study
At 6 months, 0/50 of those with repeat infections seroreverted versus 9/34 (26.5%) initial infections (p<0.001). By 12 months, this gap had widened to 3/47 (6.4%) and 13/24 (54.2%, p<0.001). The proportion seroreverting was significantly higher in initial than repeat infections in all the subgroup comparisons (table 2). We had RPR results available for 85/72 individuals at 6-month and 12-month time points. At 6 months (but not 12 months), those with repeat infections were less likely to be classified as serofast than those with initial infections (PSS: 0/29 (0%) vs 5/25 (20.0%) p=0.017, LS: 2/26 (7.7%) vs 5/11 (45.5%); p=0.016, respectively).
Retrospective cohort analysis revealed similar findings
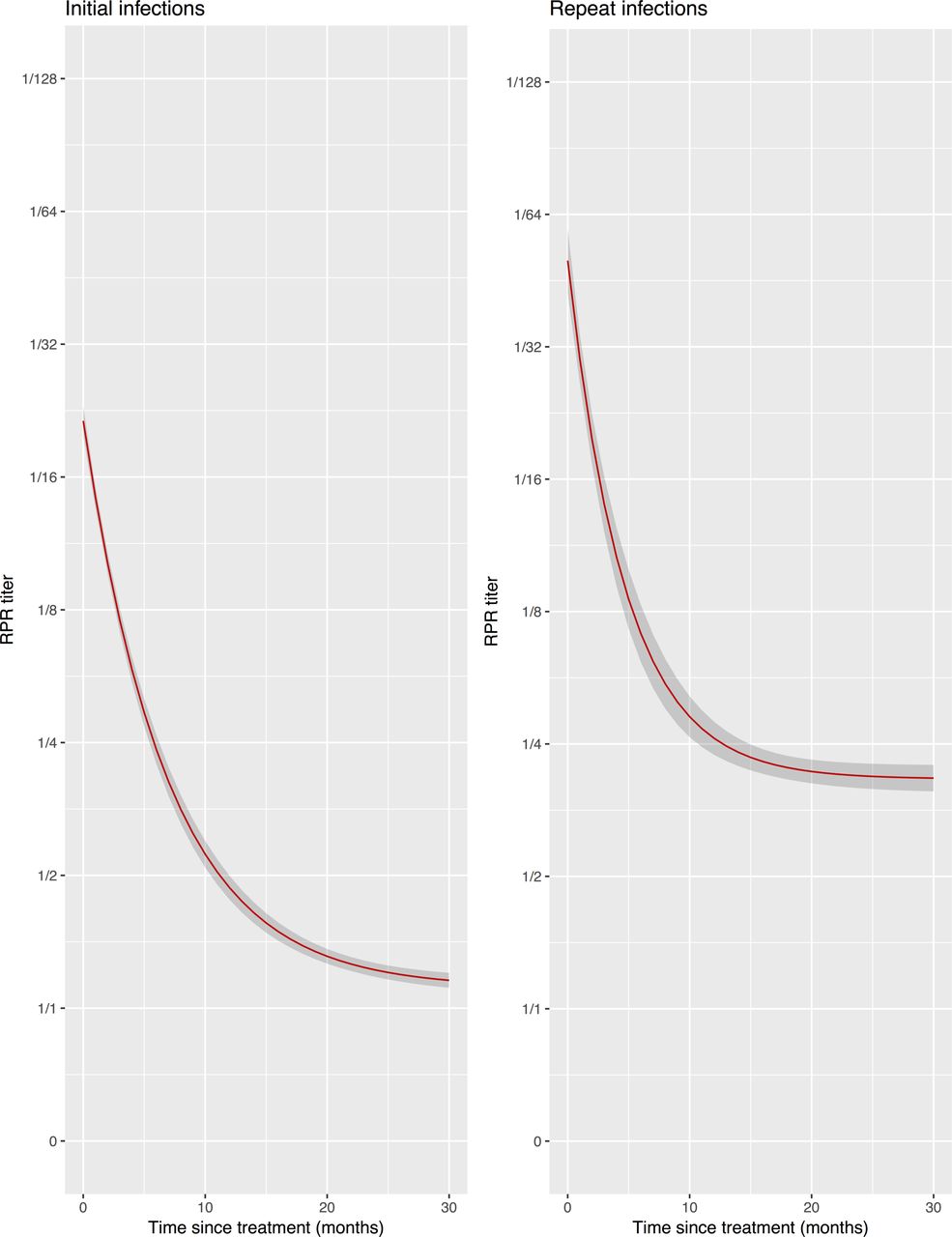
The baseline characteristics of the retrospective cohort are detailed in table 4. Overall, 97 921 serological tests for syphilis were performed on 43 870 individuals over the 23-year period. A total of 1027 initial and 530 reinfection syphilis episodes were diagnosed in this period. In 485/1027 (47.2%) cases of initial syphilis, a preceding RPR result was not available. RPR titres were higher in repeat infections than initial syphilis infections (median 1/64 (IQR 1/16-1/128) vs 1/16 (IQR 1/8–1/64), respectively, p<0.001, figure 1). RPR titres increased linearly with increasing number of syphilis infections (coefficient 0.58 (95% CI 0.53 to 0.63), p<0.0001, online supplementary figure S2). Initial infections were more likely than repeat infections to serorevert at 6 and 12 months post-treatment (6 months: 75/648 (11.6%) vs 19/407 (4.7%), p<0.001; 12 months: 183/790 (23.2%) vs 48/476 (10.1%), p<0.001, online supplementary figure S4). Each episode of syphilis had RPR follow-up results for a median 602 days (IQR 171–1527).

{kind=link}
Curves of mean rapid plasma reagin (RPR) titre decline in initial versus repeat syphilis in individuals attending HIV/STI clinic 1993–2016—retrospective series. (Grey zone represents 95% CIs. The curves stratified by initial RPR titre value are shown in online supplementary figure S4.)
Baseline characteristics of participants by initial versus repeat syphilis presentation (retrospective study)
Initial infections had a higher probability than repeat infections of remaining serofast at the 12-month (but not the 6-month) visit (12 month: 335/873 (38.4%) vs 154/627 (24.6%), respectively, p<0.001). A dose effect was present: increasing numbers of previous syphilis decreased the probability of seroreversion and serofastness (online supplementary table S5). The RPR did not serorevert in any of the participants with four or more syphilis infections (online supplementary figure S3).
Discussion
Our results are concordant with previous studies such as that of Magnuson et al, which found an altered immune response in repeat compared with initial syphilis. Repeat syphilis was less likely to present with symptomatic disease and had lower levels of plasma IL-10 compared with those without a previous history of syphilis. This is compatible with the finding in other infections that the strength of the IL-10 response reflects the strength of the preceding inflammatory response.20 RPR response rates also vary between initial and repeat syphilis. In keeping with the findings of Hutchinson et al, we found that RPR levels at diagnosis were higher in repeat than initial syphilis.8 A novel finding of our study was that RPR titres at diagnosis increase linearly with increasing number of episodes of repeat syphilis and that RPR titres decline more rapidly following repeat than initial syphilis. RPR titres were also less likely to serorevert after repeat episodes. These findings are compatible with the RPR and other NTTs representing an immunological reaction to antigens such as cardiolipin whereby repeat infections provide an immunological boost to this anamnestic response.1 21
These results have several clinical and epidemiological implications. In numerous settings, repeat syphilis constitutes an increasing proportion of syphilis cases.2 7 22–25 It is important for clinicians and epidemiologists to have accurate data of how repeat syphilis presents and its expected NTT response trajectory. The most widely used reference NTT decay curves are those produced by Brown et al. 9 These have several limitations in the contemporary era: they are based on old data (1965–1967) when older generation NTTs where used, small sample size and individuals with reinfections were excluded. Our study found a difference in the RPR decay curves between initial and repeat syphilis. Repeat syphilis had higher RPR peaks, then declined more rapidly but settled at a higher RPR than initial syphilis. Thus, the probability of seroreversion at 12 months dropped stepwise with increasing numbers of infections, and in our population it was zero at four or more infections. These reference curves provide a useful update to those produced by Brown et al.
This and other studies have found that persons with multiple episodes of syphilis are more likely to present with asymptomatic syphilis.1 2 6 7 22 Clinicians and patients could use this information to motivate for more frequent testing in such individuals as this may be the only way reinfections will be diagnosed in a timely manner.
Limitations in our study include the fact that for several of the chemocytokines, only a small proportion of samples had levels above the level of detection (online supplementary table S1). A number of these low abundance chemocytokines and cytokines had low correlations between technical duplicates (online supplementary table S1). As a result, the findings pertaining to these chemocytokines need to be interpreted with considerable caution. Furthermore, we did not correct for multiple comparisons that may have led to type I errors.26 Our sample size was small, and the fact that almost the entire cohort were MSM from one clinic reduces the generalisability of the results. The immune profile of syphilis varies in those with and without HIV infection.17 We dealt with this by controlling for HIV infection and HIV viral load in multivariate analyses. It is possible that a proportion of the cases of syphilis we classified as latent syphilis may have been diagnosed early by enhanced screening/follow-up before they presented with primary or secondary syphilis. However, this should not have influenced our comparison of initial versus repeat syphilis in the prospective cohort since we stratified the analysis by primary/secondary versus latent syphilis. The strengths of the study include its setting within a prospective observational cohort study wherein the patients had their behavioural, clinical and laboratory characteristics collected in a detailed and standardised fashion. Our RPR decay curves derived from our retrospective study did not control for syphilis stage, HIV serostatus, timing and type of therapy and changes in screening and treatment practices over 23 years, which is suboptimal. We did, however, control for these in our prospective study and found that after controlling for these, RPR titres remained higher in repeat than initial syphilis.
In conclusion, we demonstrate that the immune profile of repeat syphilis differs from initial syphilis. Further work is required to ascertain the optimal screening strategy in those with multiple previous episodes of syphilis.
Key messages
We found differences in the presentation and response to therapy between initial and repeat syphilis.
Initial syphilis is more likely to be symptomatic than repeat syphilis.
Initial syphilis has a higher interleukin-10 level than repeat syphilis.
Repeat syphilis is more likely to remain serofast than initial syphilis.
Acknowledgments
We would like to thank Said Abdellati and Vicky Cuylaerts for performing the cytokine assays.
References
Footnotes
CK and AT contributed equally.
Contributors CK conceptualised the study. CK and AT were responsible for the acquisition, analysis and interpretation of data. AT, CK, KO, TC, LK and MVE played a role in writing, editing and approving the final version.
Funding This work was part of Project ID: 757003 funded by the Flemish Government -Department of Economy, Science & Innovation.
Competing interests None declared.
Ethics approval Ethics Committee of the University Hospital Antwerp.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. The last author’s surname (Kesten) should be spelt Kestens. This has now been corrected.