Article Text

Abstract
Objectives Trichomonas vaginalis (TV) is the most common curable STI worldwide and is associated with increased risk of HIV acquisition and serious reproductive morbidities. The prevalence of TV infection is very low in Australian cities, and this is thought to be at least partly due to incidental detection and treatment of TV in women participating in the cervical cytology screening programme. In 2017, the national cervical screening programme will transition to a new model based on testing for high-risk (HR) human papillomavirus (HPV), with a reduced frequency and commencement at an older age. We model the potential impact of this transition on TV prevalence in Australia.
Methods A mathematical model was developed to describe the transmission of TV in the general population and used to evaluate scenarios that capture the switch from cytology-based screening to HR HPV testing. Under these scenarios, individuals with asymptomatic TV who test negative for HR HPV will remain undiagnosed and untreated. We estimate the change in TV prevalence expected to occur due to the switch from cytology to HR HPV testing and changes to the frequency and age at commencement of screening.
Results Our results suggest that with the transition to HR HPV testing, TV prevalence may increase from the current ~0.4% to 2.8% within 20 years if TV testing coverage is not increased and HR HPV prevalence does not decline further. If HR HPV prevalence continues to decline at its current rate with ongoing vaccination, TV prevalence is predicted to increase to 3.0% within this time frame.
Conclusions Our modelling suggests that in a setting like Australia, where TV can be detected incidentally through cytology-based cervical screening, a transition to HPV testing is likely to result in increasing TV prevalence over time unless additional measures are implemented to increase TV testing and treatment.
- Trichomonas
- mathematical model
- screening
- HPV
Statistics from Altmetric.com
Introduction
Trichomonas vaginalis (TV) infection is the most common curable STI worldwide and is associated with increased risk of HIV acquisition,1–4 reproductive morbidity such as preterm labour5 and pelvic inflammatory disease.6 7 TV prevalence varies considerably within and between countries. In the USA, for example, prevalence is low among white women and is considerably higher among black women,8–10 while in the UK prevalence is generally very low.11 In Australia, TV prevalence is low in urban populations (<1%),9 12 but is very high among Aboriginal men and women living in remote areas (>10%).10 13 14 However, as most TV infections are asymptomatic they often remain undiagnosed and untreated for a long period of time.15 Because of the low prevalence of TV in Australia, current guidelines do not recommend routine testing for TV for asymptomatic individuals in the general population.16
While not included as part of routine STI screening in urban Australia, TV infection is currently reported in cervical Pap smears if there is cytological evidence of infection, and general practitioners will treat women for TV infection if it is reported and confirmed by an additional diagnostic test.17 Similarly, in the UK, TV has been reported when detected on Pap smears,18 but as described below for Australia, this is changing with the transition from cytology to human papillomavirus (HPV) testing for cervical screening. On the other hand, in the USA, TV has generally not been reported on Pap smears as the sensitivity and specificity of this method of detection are considered too low.19 While the sensitivity of cytology for detection of TV is only about 50%, it has been previously hypothesised that the low TV prevalence in urban Australian populations may be due, at least in part, to incidental detection through the cervical screening programme.20 21 Further support for this comes from a study in Sydney showing the risk of TV infection was independently associated with those who have never had a Pap smear.22
Virtually all invasive cervical cancers are caused by persistent infection with a subset of HPV types.23 These oncogenic types are denoted as high-risk (HR) HPV. In Australia, the National Cervical Screening Program has been in place since 1991 in order to detect cervical cancer and precancerous changes.24 The programme has achieved a 2-year participation rate of almost 60%.25 Prior to 2017, the recommended practice has been to screen all women aged 18–69 years who have ever been sexually active on a 2-year basis using cervical cytology as the primary screening test.26 However, from May 2017, the cervical screening programme will undergo a major revision with the following key changes27: HPV testing will replace the Pap test as the primary screening test and women testing positive to HPV 16/18 will be referred directly to colposcopy; women testing positive to other HR types will be triaged using liquid-based cytology, with high-grade cases referred directly to colposcopy, and the remainder recalled for 12-month follow-up; screening will commence later at age 25 years, up from 18; and the frequency of screening will be decreased from 2 to 5 years. The revised cervical screening programme is predicted to be substantially more effective in preventing cervical cancer and potentially cost-saving compared with the current cytology-based programme.28
We hypothesise that the changes to the cervical screening programme in Australia will result in increasing TV prevalence for two reasons. First, under the new programme, only those who are identified as HR HPV positive will be referred for cytology, therefore those who have asymptomatic TV infection but are HR HPV negative will not be tested or receive treatment. Second, the increase in the age at commencement of cervical screening and the decrease in the frequency of screening will also result in fewer TV infections being detected and treated. The extent to which these factors impact on TV prevalence is also likely to depend on the extent to which HR HPV prevalence continues to decline with ongoing HPV vaccination and the imminent introduction of a nine-valent HPV vaccine that provides protection against infection with an additional five HR HPV types.
To test this hypothesis, we developed a mathematical model of TV transmission to investigate the potential impact of the new cervical screening programme on TV prevalence in the urban population (over 85% of the total population29) in Australia.
Methods
We developed a compartmental, deterministic mathematical model to describe the TV transmission in the urban Australian population, assuming an underlying background prevalence of HR HPV. The model was developed using MATLAB software (MATLAB release 2016b, The MathWorks, Natick, Massachusetts, USA). The model accounts for changes in the diagnosis and treatment rate of TV that will occur due to changes to the cervical screening programme (outlined above) and predicted changes in HR HPV prevalence due to ongoing vaccination. The key features of the model are summarised below and a full technical description of model implementation is provided in the online supplementary technical appendix.
Supplementary file 1
The modelled population, representing the general urban population in Australia, is distributed between the following non-overlapping compartments (or states): susceptible to TV infection; exposed to TV but not yet infectious; infectious with TV infection; and treated. Individuals who are infected with TV can become susceptible again through natural recovery or through treatment. For women, the infectious compartment is further divided into five compartments based on the appearance of TV-related symptoms and HR HPV infection status (asymptomatic TV infection but HR HPV negative; asymptomatic TV infection and HR HPV positive; symptomatic TV infection but HR HPV negative; symptomatic TV infection and HR HPV positive; and symptomatic TV infection in those who seek treatment). For men, the infectious compartment is divided into those with asymptomatic TV infection and those with symptomatic TV infection. The model compartments and pathways are illustrated schematically in online supplementary technical appendix figure A-1.
It is important to note that HR HPV transmission is not explicitly modelled, rather we assume an underlying and age-specific background HR HPV prevalence for women based on published data (see below and online supplementary technical appendix).30 31 Each compartment is stratified into 1 year age groups ranging from 16 to 60 years. Each female compartment is further stratified according to HPV vaccination status (unvaccinated, vaccinated).
We define time point t=0 as the time when the new revised cervical screening programme commences. Prior to t=0, we assume all cervical cancer screening is cytology-based. With cytology-based screening, the detection of TV infection in women is not dependent on HR HPV infection status and is unaffected by HPV vaccination. This constitutes our baseline model, along with the assumption that 60% of women 18 years or older will be tested every 2 years, based on current participation rates.25 While robust estimates of TV prevalence in urban Australia are not available, limited published data suggest it is around 0.4% or lower.9 12 We therefore calibrated our baseline model to produce a stable endemic equilibrium TV prevalence of ~0.4% prior to implementation of the revised cervical screening programme. To achieve this, SaSAT software was used to generate 5000 parameter sets with Latin hypercube sampling,32 where model parameters were randomly sampled from prespecified ranges (see online supplementary technical appendix). The model was run to equilibrium for all 5000 parameter sets (assuming 60% of women aged 18 years or older undergo cytology screening every 2 years) and the 50 sets yielding equilibrium prevalence closest to 0.4% were selected for evaluating screening scenarios (see below) and sensitivity analysis (see online supplementary technical appendix). The median prevalence yielded by the 50 selected parameter sets was 0.40%, with an IQR of [0.10%, 0.78%].
We then explored the potential impact on TV prevalence in the population due to the changes to the cervical screening programme. The following scenarios were investigated:
Switching the primary screening test for cervical screening from cytology to HR HPV testing with no change to screening coverage, age at commencement of screening, or screening frequency. Note that only women returning a positive HR HPV test will be referred for cytology, meaning that women with asymptomatic TV infection who are HR HPV negative will no longer be diagnosed with TV as a result of the screening process.
Retaining cytology as the primary cervical screening technology but increasing the age of commencement of cervical screening from 18 to 25 years; increasing screening coverage from 60%25 to the expected screening 5-year coverage of 80%; and reducing screening frequency from 2 to 5 years. The combined effects of increased coverage and reduced screening frequency under this scenario result in an overall decrease in the testing rate (approximately 30% decrease in the daily testing rate).
Combination of scenarios 1 and 2 as will be implemented in Australia from May 2017.
While scenario 3 comprises the full raft of changes to the cervical screening programme that will be implemented in Australia from May 2017, scenarios 1 and 2 are included to separately explore the respective impacts on TV prevalence of changing the primary screening test (scenario 1) and the changes to screening frequency, coverage and age of commencement (scenario 2).
For the scenarios that involve changes to the primary screening test (ie, scenarios 1 and 3 above), we subdivide the analyses further to reflect differing assumptions regarding the future trajectory of HR HPV prevalence. First, we estimated HR HPV prevalence in 2016 to be 37.7% among unvaccinated women and 22.8% among vaccinated women. This is obtained by assuming that between 2011 and 2016, HR HPV prevalence continued to decline at the same rate as observed between the prevaccination period of 2005–2007 and the postvaccination period of 2010–2011.30 We then investigate the changes in TV prevalence under two different assumptions: (1) HR HPV prevalence does not decline further from the estimated 2016 level; and (2) HR HPV prevalence continues to decline at the same rate as estimated for the period prior to 2016.
We performed a sensitivity analysis to assess the possible effects of parameter uncertainty on the results. For this analysis, we focused on the absolute changes to modelled TV prevalence 20 years after introduction of the fully implemented, revised cervical screening programme (ie, scenario 3 above). The relative importance of each parameter is estimated through calculation of a partial rank correlation coefficient (PRCC) using SaSAT software.33
Results
The changes in TV prevalence that are predicted by the model to occur as a result of changes to the cervical screening programme are illustrated graphically in figures 1–3 for scenarios 1–3, respectively. These results are also summarised numerically in table 1 as absolute and relative changes in TV prevalence. Results are given below as medians and IQRs in square brackets.
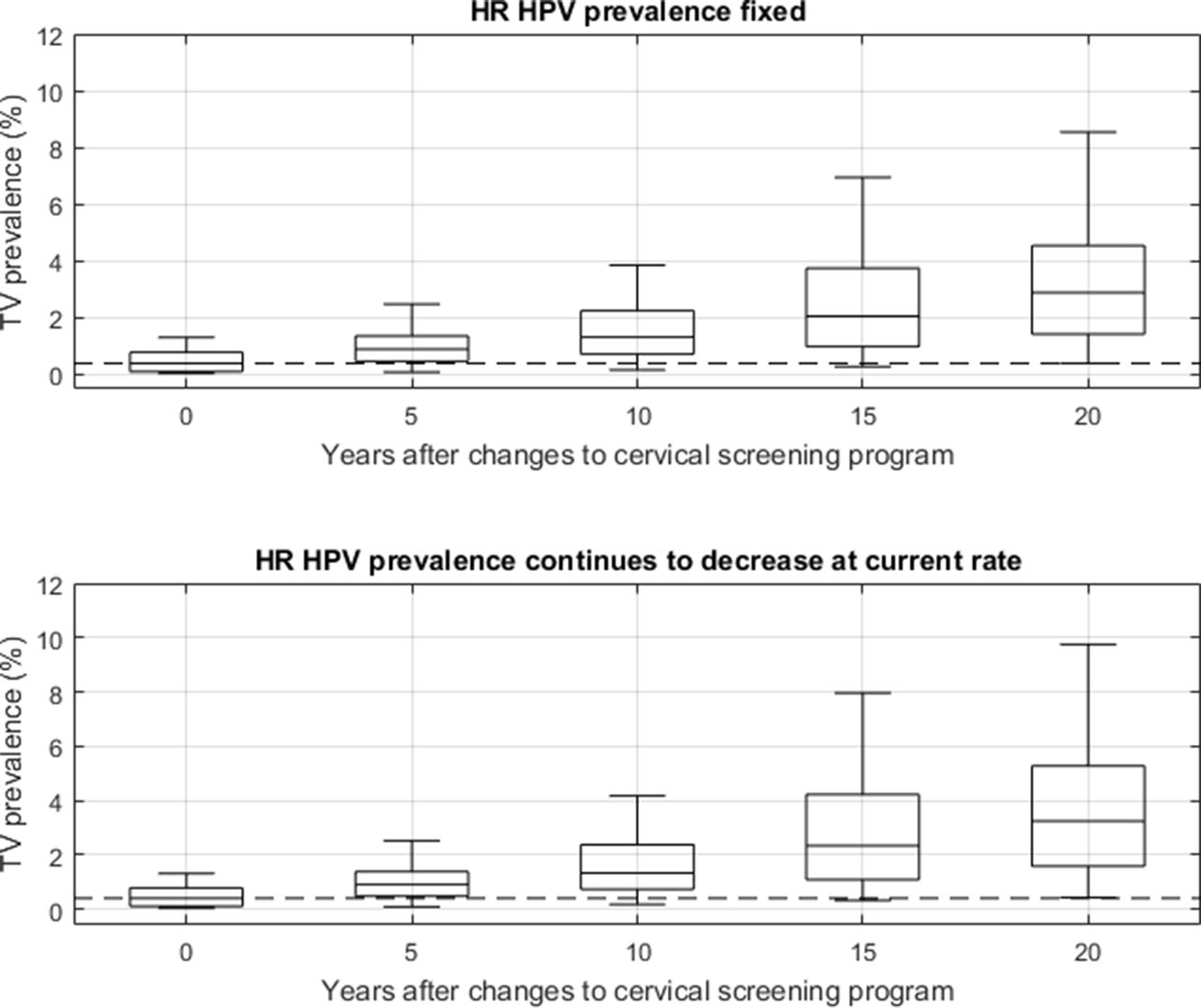
TV prevalence at t=0, 5, 10, 15 and 20 years for scenario 1 (where HPV testing replaces cytology, but cervical screening coverage, age at commencement and screening interval remain unchanged). The centreline in each box indicates the median prevalence and the box represents the 25th–75th percentiles for 50 simulations. The whisker length is 1.5 times the width of the IQR (corresponding to 99.3%, or approximately ±2.7 SDs, coverage of the data if prevalence at steady state is normally distributed), and outliers are not plotted. The dotted line indicates the median prevalence of 0.43% at baseline (t=0) for the 50 simulations. HPV, human papillomavirus; HR, high risk; TV, Trichomonas vaginalis.
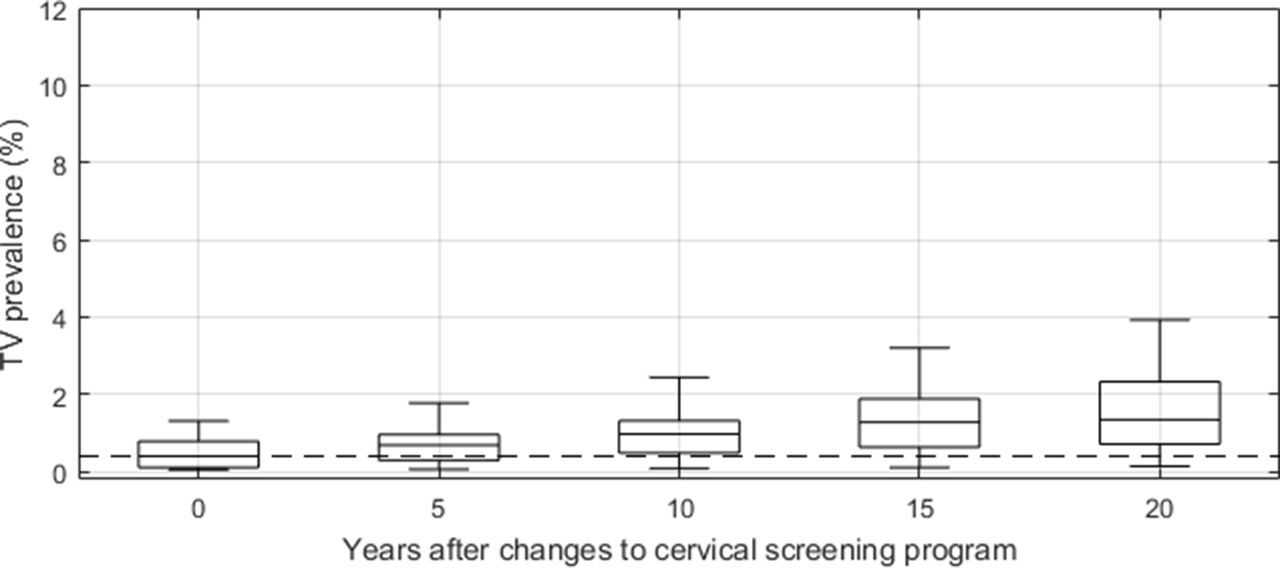
TV prevalence at t=0, 5, 10, 15 and 20 for scenario 2 (where cytology remains the primary cervical screening technology but screening coverage is increased from 60% to 80%, screening commences at age 25 rather than 18 and the screening frequency is reduced from 2 to 5 years). Other features of this figure are as described for figure 1. TV, Trichomonas vaginalis.

{kind=link}
{kind=link}
{kind=link}
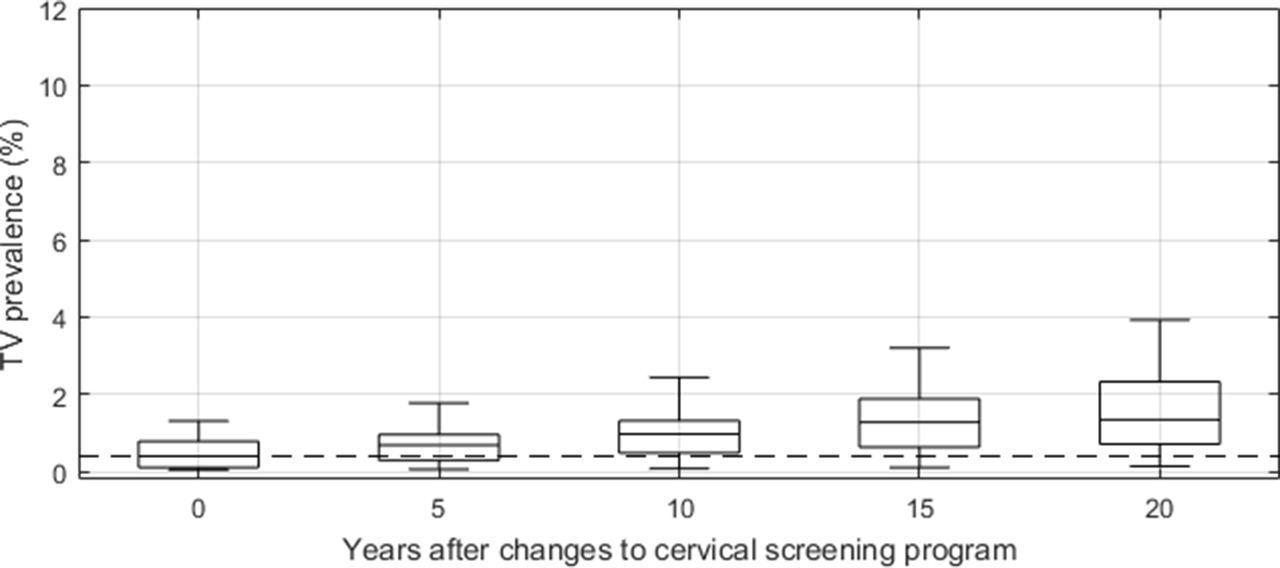
TV prevalence at t=0, 5, 10, 15 and 20 for scenario 3 (where HPV testing replaces cytology for cervical screening, screening commences at age 25 rather than 18 and the screening frequency is reduced from 2 to 5 years). Other features of this figure are as described for figure 1. HPV, human papillomavirus; HR, high risk; TV, Trichomonas vaginalis.
Absolute and relative increases in TV prevalence from baseline at t=5, 10, 15 and 20 years, for scenarios 1, 2 and 3*
Scenario 1: screening is switched from cytology to HR HPV testing with no other changes to the programme
Figure 1 shows the modelled TV prevalence at 5, 10, 15 and 20 years after HR HPV testing replaces cytology as the primary cervical cancer screening test. TV prevalence is predicted to double within 5 years to 0.89% [0.47%, 1.36%], and to increase ~7-fold to 2.89% [1.43%, 4.54%] within 20 years if HR HPV prevalence remains at the current (2016) level. If HR HPV prevalence continues to decline at the current rate, TV prevalence is predicted to increase ~8-fold to 3.24% [1.58%, 5.27%] within 20 years.
Scenario 2: screening remains cytology based but screening coverage, age at first screen and screening interval are increased
Figure 2 shows the modelled TV prevalence at 5, 10, 15 and 20 years if cervical screening changes from 60% coverage of 2-year screening of women starting at age 18 years or older to 80% coverage of 5-year screening of women starting at age 25 years or older, while cytology remains the primary cervical cancer screening test. TV prevalence is predicted to increase by ~70% to 0.68% [0.29%, 0.96%] within 5 years and to increase more than threefold to 1.34% [0.71%, 2.33%] within 20 years. Note that under this scenario, changes to HR HPV prevalence have no effect on TV prevalence as cytology remains the primary screening test and TV detection is thus independent of HR HPV status.
Scenario 3: combination of scenarios 1 and 2
Figure 3 shows the modelled TV prevalence at 5, 10, 15 and 20 years if changes to cervical screening (HR HPV testing replaces cytology, screening commences at age 25 years and screening interval is 5 years) are fully implemented in accordance with the changes to be introduced in Australia from May 2017. TV prevalence is predicted to more than double within 5 years to 0.92% [0.50%, 1.40%] and to increase more than eightfold to 3.25% [1.55%, 5.07%] within 20 years if HR HPV prevalence remains at its current (2016) level. As with scenario 1, the predicted increases in TV prevalence are greater (to 0.93% [0.51%, 1.41%] and 3.44% [1.63%, 5.52%] after 5 and 20 years, respectively) if HR prevalence continues to decline at the current rate.
Sensitivity analysis
The PRCCs for all model parameters are illustrated in online supplementary technical appendix figure A-6, as a tornado plot, and listed in online supplementary technical appendix table A-3. The sensitivity of cytology for TV detection contributes most substantially to variability in the absolute increase in TV prevalence when HPV testing is introduced, with a PRCC of 0.65 if HR HPV prevalence remains unchanged, and a PRCC of 0.67 if HR HRV continues to decline.
For parameters related to the natural history of TV, the results of the sensitivity analysis show that parameters pertaining to men contribute more substantially to variability in the outcome measure (increase in TV prevalence) than the corresponding parameters for women. If HR HPV prevalence remains unchanged, then the duration of infection for men (PRCC of −0.31) and the proportion of infections that are asymptomatic in men (PRCC of −0.13) contribute more to outcome variability than their female counterparts (PRCCs of −0.05 and −0.07, respectively), although the latter makes a relatively minor contribution for both men and women. The male-to-female transmission probability (PRCC of −0.25) also contributes more to the variability than the female-to-male transmission probability (PRCC of −0.08), but again the latter makes a relatively minor contribution. This overall pattern is replicated if HR HPV continues to decline, with slight variations to the PRCC values.
Discussion
The risk of developing cervical cancer in Australia has been decreasing over recent decades, largely due to an effective cervical screening programme and, more recently, HPV vaccination. The forthcoming changes to the cervical screening programme are expected to provide a substantial additional reduction in the number of cervical cancers over time.26 However, the transition to HPV testing will also result in a reduction in the number of cytology tests performed, which will in turn lead to a decrease in the detection of asymptomatic TV infections. Our model predicts that these changes to the cervical screening programme will result in a greater then sevenfold increase in TV prevalence within 20 years if additional measures are not implemented to increase testing and treatment of asymptomatic TV. Furthermore, although not investigated in this study, the imminent introduction of the nine-valent HPV vaccine is expected to lead to an even greater reduction in the prevalence of HR HPV and therefore even fewer reflex cytology tests for TV diagnosis. This suggests that the increase in TV prevalence predicted by our model is likely to be a conservative estimation of the real increase.
The prospect of increasing TV prevalence does not provide justification for altering or delaying the planned changes to the cervical screening programme. These changes have been rigorously evaluated and are expected to yield substantial reductions in the incidence of cervical cancer and associated costs. However, consideration could be given to integrating a molecular test for TV into the HR HPV testing process and to expanding routine STI screening to include TV for young people not eligible for HR HPV testing. At the very least, surveillance systems should be put in place to monitor changes in TV prevalence following the transition to HR HPV testing.
It has been hypothesised that the low level of TV prevalence in urban Australia is due, at least in part, to the incidental diagnosis of TV diagnoses on Pap smears performed for cervical cancer screening. While there are Australian studies to support this hypothesis,20 22 we were unable to identify published data from other countries to further substantiate it. TV infection is not notifiable in Australia, meaning the total annual number of diagnoses in the general population and the proportion of diagnoses detected through cervical screening is unknown. However, the aim of this study was not to assess whether cervical screening is an effective means of reducing the prevalence of TV infection, but rather to estimate the potential impact on TV prevalence if fewer TV infections are diagnosed with the shift from cytology-based cervical screening to HPV testing. Current guidelines recommended in Australia include the reporting of TV on Pap smears and we thus calibrated our model to the estimated TV prevalence in the general urban population, assuming a sensitivity of 57% for TV detection on the Pap smear. We consider our result to be applicable for similar settings, where TV prevalence is low, cytology-based cervical screening coverage is high and TV is currently reported on Pap smears. The results are not applicable for other dissimilar settings such as populations where TV prevalence is high and/or cervical screening coverage is low.
It is thought that a combination of low TV treatment rate (due to the high proportion of infections that are asymptomatic) and long duration of infection, rather than frequent transmission, is the main contributor to TV persisting in older age groups compared with other STIs such as chlamydia and gonorrhoea, which tend to be more concentrated in younger age groups. Because TV continues to be prevalent in older age groups, despite lower levels of sexual activity,14 we suggest that screening and treatment of older age groups will have some impact in reducing TV prevalence and this is borne out by the findings from our model.
There are limitations in this study that should be noted. We did not stratify our modelled population by levels of sexual activity, on the basis that, as noted above, it has been observed in subpopulations where TV infection is common, that prevalence tends to be similar across all age groups in the sexually active population despite higher partner acquisition rates in younger age groups.13 However, due to a lack of data, it is difficult to ascertain if this observation holds for populations where TV infection is rare. There is also considerable uncertainty regarding TV natural history parameters, in particular the duration of untreated TV infection in women. This uncertainty, and that for all model parameters, is accounted for in the prespecified ranges from which parameter values are selected for our simulations. However, our sensitivity analysis suggests that uncertainties in TV natural history parameters for women are of relatively low importance in contributing to variability in the increase in TV prevalence. This is not surprising given the natural history of TV will not be affected by changes to cervical screening practices. This is likely to be different if the sensitivity analysis was performed for TV prevalence rather than the increase in TV prevalence, as uncertainties in women’s TV natural history parameters would be expected to contribute more substantially to variability in modelled prevalence. We found that the absolute increase in TV prevalence is most strongly influenced by the uncertainty in the sensitivity of Pap smears. If the sensitivity of the Pap smear is assumed to be higher than 57% (base case assumption), then a higher proportion of TV infections will go undetected when cervical screening transitions to HPV testing and thus the absolute increase in TV prevalence following the transition will be higher than predicted in our base case. Conversely, if the sensitivity of the Pap smear is assumed to be lower than 57%, switching to HPV testing will have a lesser impact on TV prevalence as cytology-based screening will account for a smaller proportion of TV diagnoses. The impact of changing Pap smear sensitivity on our findings is illustrated in the results presented in online supplementary technical appendix table A-6. Here, the absolute and relative increases in TV prevalence, under scenario 3, have been obtained for recalibrated baseline models where the sensitivity of the Pap smear is set to 30% and 70%. This analysis shows that if the sensitivity of the Pap smear for TV detection is reduced to 30%, then the increase in TV prevalence due to the transition to HPV testing will also be lower, with a relative increase at 20 years of around 3.6% (compared with 8.1%) when HR HPV prevalence remains constant, and 3.7% (compared with 8.8%) if HR HPV prevalence continues to increase. From a transmission point of view, the model only considers TV and assumes that TV infection and HPV infection are entirely independent. In reality, having one infection may alter the probability of having the other. We also assume that changes to the cervical screening programme and HPV vaccination can be represented in the model as a simple function of HR HPV prevalence. A more complex model that also accounts for HPV transmission is required to assess the full impact of changes to both HR HPV and TV prevalence, but the added complexity would also add to the uncertainty in the outcomes. Finally, the revised screening programme includes additional features such as repeated HPV testing and different follow-up procedures for those who test HR HPV positive. Assessment of these changes is not possible using the current compartmental model as it does not keep track of an individual’s infection status and treatment history through time.
Conclusions
Our model predicts that the prevalence of TV infection in urban Australia will rise substantially once changes to the cervical screening programme are fully implemented. If this is the case, the morbidities associated with TV infection as well as HIV incidence can also be expected to increase accordingly. In light of these findings, we suggest that additional measures should be considered to increase TV testing in order to mitigate a substantial increase in the prevalence of asymptomatic TV infection. Our findings are also of relevance to settings such as the UK where TV prevalence is low, TV is currently reported on Pap smears and a transition to HPV testing for cervical screening is under way or being considered.
Key messages
Modelling suggests that changes to Australia’s cervical screening programme will lead to a decrease in the detection of asymptomatic Trichomonas vaginalis (TV) infections and thus an increase in the prevalence of TV.
Measures to increase TV testing and treatment should be considered in order to prevent increases in TV prevalence when transitioning from cervical cytology screening to human papillomavirus (HPV) testing.
Our findings have relevance for other settings such as the UK where TV has been routinely reported on cervical cytology and that are now implementing a transition to HPV testing.
References
Footnotes
Handling editor Katy M E Turner
Contributors BBH and DGR developed and collaborated in the writing of the manuscript. BBH and CPR were involved in the design and implementation of the model. RJG, BD, JSH and MGL were involved in providing expert opinions on cervical screening and HPV. RB and JSH were involved in providing expert opinions on transmission of Trichomonasvaginalis and laboratory practice. All coauthors revised the manuscript before submission.
Funding DGR and BBH are supported by a National Health and Medical Research Council Program Grant (568971). The Kirby Institute is funded by the Australian government Department of Health and Ageing, and is affiliated with the Faculty of Medicine, University of New South Wales.
Disclaimer The views expressed in this publication do not necessarily represent the position of the Australian government.
Competing interests BBH reports grants from the National Health and Medical Research Council during the conduct of the study; CPR reports personal fees from The Kirby Institute during the conduct of the study; MGL reports grants from Boehringer Ingelhiem, Gilead Sciences, Merck Sharp & Dohme, Bristol-Myers Squibb, Janssen-Cilag, ViiV HealthCare, and personal fees from Gilead Sciences, Sirtex, outside the submitted work; DGR reports grants from the National Health and Medical Research Council during the conduct of the study; RJG, BD and JSH have nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.