Article Text

Statistics from Altmetric.com
Key messages
An increasing proportion of STI testing in the UK is occurring via online postal self-sampling (OPSS) services.
Service users tend to be asymptomatic, white, women, over 20s and from less deprived areas.
OPSS services are acceptable to users and can improve choice.
There is a need for a wide-ranging evaluation of OPSS services to determine their impact on sexual health inequalities, access, clinical outcomes and service delivery.
Introduction
‘Home testing’ whereby an individual tests for STIs and/or blood-borne viruses (BBVs) remote from traditional healthcare settings, encompasses user self-sampling (the laboratory processes and tests the samples) or self-testing (the user tests their own samples).1 The most widely used option in the UK is online postal self-sampling (OPSS) in which users order specimen collection kits via the internet. Kits are delivered by post or may be collected from a sexual health clinic. Users obtain their own samples (typically urine or vulvo-vaginal swab, blood, and anorectal and pharyngeal swabs where appropriate), and repackage before posting back to a laboratory for testing. Test results are made available by text message or online. OPSS is increasingly provided in high-income countries.2–4 England’s earliest online chlamydia testing services began in 2006,5 but the other devolved nations of the UK introduced OPSS rather later.6–8 The BASHH recommends online testing and care provision as an adjunct to in-person services to increase choice for service users.9
The UK had seen a sustained rise in diagnoses of several STIs, and increase in demand for sexual health service (SHS) consultations, until the start of the COVID-19 pandemic.10 Between 2015 and 2019 in England, there was a 23% increase in the number of SHS consultations (3 143 144–3 852 121). Total sexual health screens for chlamydia, gonorrhoea, syphilis and HIV increased by 31% (1 657 425 to 2 175 525) in this period. Internet-based services have assumed an increasing proportion of consultations and screening activity. In 2018–2019, while overall consultations and tests in England rose by 7% and 10%, respectively, consultations and STI screens provided by internet-based services surged by 94% and 69%.10 This trend of an increasing proportion of testing and consultations being accessed and provided online has accelerated as a result of the COVID-19 pandemic.11 Young people, people from ethnic minority groups, men who have sex with men (MSM), people who are gender diverse, and those living in more deprived areas have borne a disproportionate burden of STIs and poorer sexual health for many years.12–17 The reasons for this disparity are not sufficiently understood.18
Some evidence suggests that OPSS might improve access to STI services for those who feel uncomfortable or struggle to attend face-to-face services,19 and might cost less than in-person care.20 21 However, relatively little is known about the characteristics of people who use OPSS and the existing literature is heterogeneous and has not previously been comprehensively reviewed. With a drive towards further online sexual health provision in the UK,22 the pre-existing unequal burden of sexual ill health in the population and well-described inequalities in access to sexual healthcare, it is important to understand the impact of this shift in service delivery. We aimed to evaluate the current evidence on access to and usage of OPSS services. We have restricted our scope to the UK because online care has been relatively mainstreamed in at least one country (England) for many years and sexual healthcare is provided free at the point of access without the need for specialist referral. Our specific objectives were to: (1) describe characteristics of people accessing and using STI self-sampling services in the UK; (2) assess whether OPSS increases demand for testing; (3) assess the impact of OPSS on clinical outcomes; (4) assess levels of acceptability of OPSS services in the UK.
Methods
We conducted a systematic scoping review in order to map and synthesise the current research evidence, in an area where the existing literature is heterogeneous and has not previously been comprehensively reviewed.23 We followed the Joanna Briggs Institute Framework of Evidence Synthesis (https://jbi.global/scoping-review-network/resources) and Preferred Reporting Items for Systematic Review and Meta-Analyses extension for scoping reviews guidelines.24 A review protocol has not been registered. The Population/Intervention/Comparators/Outcome framework was used to identify the research question and objectives:
Population
People residing in the UK who are engaging in sexual activity and accessing online SHS.
Intervention
Self-sampling STI testing kits which are posted to individuals’ homes by online SHS.
Comparators
The alternatives to this intervention are for individuals to visit sexual health clinics, general practice, or community outreach services to be tested by healthcare professionals, self-sample in a clinical setting, or collect kits to bring home. This review will compare OPSS with these comparators where included studies have done so.
Outcome
Accessibility and usage of OPSS services, with a focus on inequalities in access and acceptability of services, and the impact of these on sexual health inequalities.
Study selection criteria
Studies were included if they described the use of home self-sampling kits provided by online SHS in the UK, published between 1 January 2010 and 30 June 2021 in the English language. All non-theoretical study types with full-text online access were included. Studies were excluded if they described services outside of the UK, published prior to 2010 or not in English, and not focusing on home self-sampling kits provided by online SHS (for example, STI education, contraception or self-testing kits). We also excluded ‘siloed’ (HIV only) HIV self-sampling services because the national HIV self-sampling service targets specific key populations such as MSM and black African groups22 rather than the general population, and one of our key objectives was to evaluate access to, including potential inequalities with, the use of OPSS services. Protocols of studies and research displayed via conference or other forms of presentation were excluded if there was no full-text access.
Study selection
De-duplication and title screening was conducted by the first author; 20% of the abstract screening and 100% of the full-text screening were verified by a second reviewer (KCL and JG, respectively) independently to reduce selection bias.25 The inter-reliability rate of the two reviewers was over 90% at the abstract screening stage and was 100% for full-text screening.
Search method
A systematic search and data extraction was conducted on 22 June 2020 to fulfil requirements of KS’ Masters dissertation and was rerun on 7 July 2021 by JG in nine databases: Medline, EMBASE, PsycInfo, the Health Management Information Consortium, Web of Science, CINAHL Plus, Scopus, Open Grey and Ethos. The use of two grey literature databases (Open Grey and Ethos) aimed to reduce potential publication bias and provide a more comprehensive view of the evidence.26 The search consisted of a selection of medical subject headings terms, where appropriate, and free-text. Limits were used in applicable databases which limited by date and language. The search comprised of four concepts: types of STI, type of online or self-sampling service, accessibility or inequalities, and UK filters. For example, terms such as ‘STI’, ‘Chlamydia’, ‘Self-Sampl*’, ‘eHealth’, ‘Access*’, ‘Inequalit*’, ‘United Kingdom’ and ‘England’ were used. To ensure the search strategy was fully comprehensive, additional terms for ‘eHealth’ were included,27 and adapted and simplified versions of two verified filters for the UK were used in database searches, where appropriate.28 29
The search only included studies published between 2010 and 2021; this was due to the very low numbers of users of OPSS services prior to 20105 (see online supplemental file 1 for details of the full search strategy).
Supplemental material
Data extraction
The phases of data identification, de-duplication, screening and eligibility checks are shown in figure 1. For included studies, a data extraction form (online supplemental file 2) was used to extract the demographics of the study participants (online supplemental file 3), the study design and key findings from each study (online supplemental file 4).
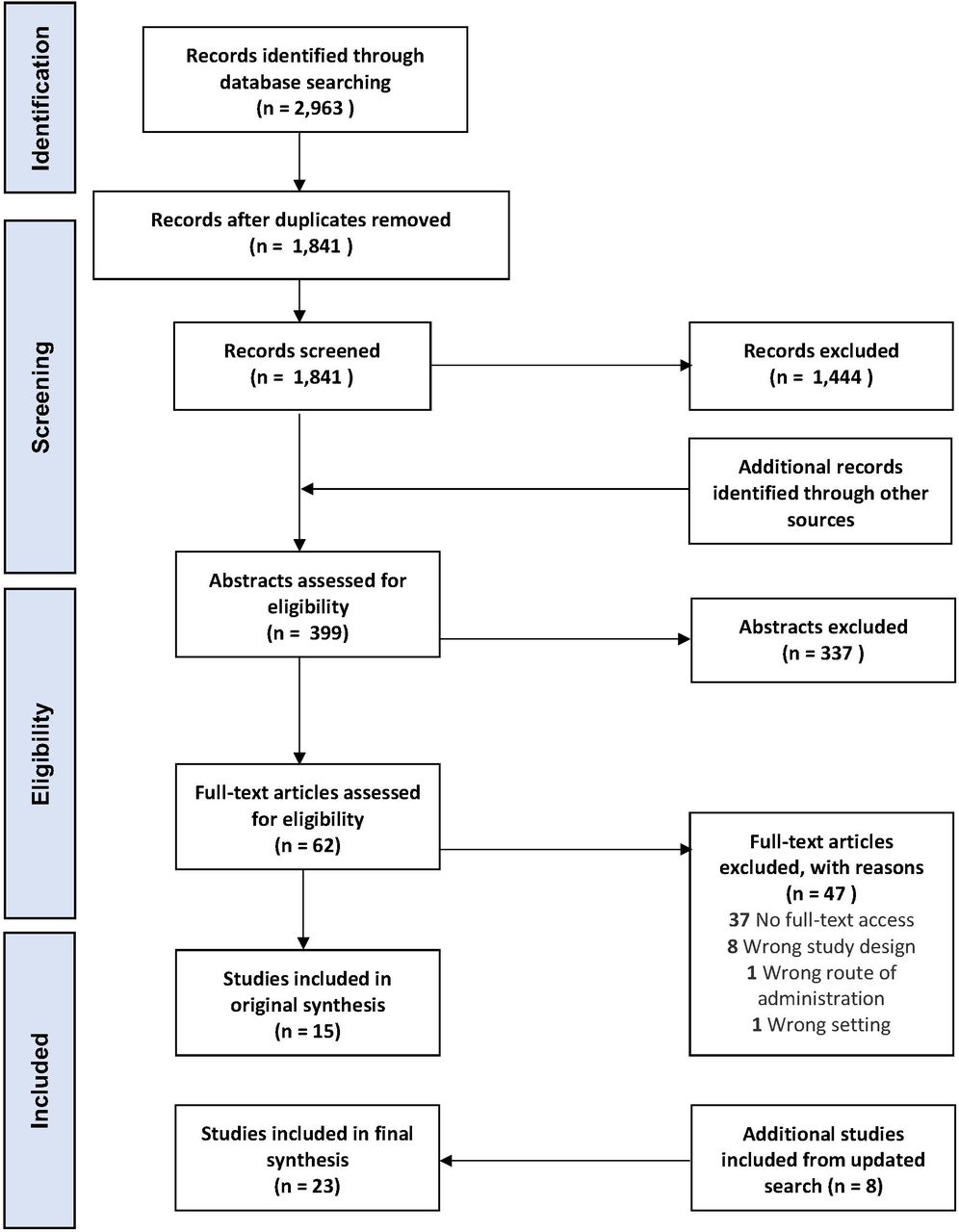
{kind=link}
Flow of Information, based on the Preferred Reporting Items for Systematic Review and Meta-Analyses flow diagram.32
Empirical appraisal and analysis of included articles
Study designs were heterogeneous, including quantitative, qualitative and mixed-methods analysis, and were therefore appraised using the Mixed Methods Appraisal Tool (MMAT).30 Quantitative data were analysed using descriptive statistics, and qualitative data were analysed using inductive thematic analysis.31
Results
Overview of included studies
This search strategy identified 23 relevant articles that described 10 different OPSS services, all located in England (see table 1 and online supplemental files 3 and 4). The overall quality was variable, with the majority either evaluating a single-site/testing provider, and exploratory or observational (see online supplemental file 5 for the full MMAT results; for a summary of each individual service or intervention, see online supplemental file 6). We found only one randomised controlled trial, which was single blind and where the intervention was a Short Message Service (SMS) containing a link to an OPSS website and the control was a link to a webpage that contained information for clinics where the recruits aged 16–30 years old could access testing . Six studies explored solely chlamydia testing, 1 assessed a chlamydia and gonorrhoea testing service and 17 assessed services which tested for chlamydia, gonorrhoea, HIV and syphilis. Five articles compared demographic characteristics and outcomes of users of OPSS with clinic-based services.20 32–36
Overview of included studies
As standardised definitions were not used across the included studies for terms such as ‘access’, ‘usage’ or ‘demand’, we have not attempted to define related terms in this scoping review.
Characteristics of those accessing OPSS services
Comprehensive demographic data were not consistently collected across studies, in terms of both type of data collected and what was collected (see table 1). Only two studies collected demographic data on all of gender, age, ethnicity, sexual orientation and the Index of Multiple Deprivation (IMD)32 37 ; two collected none of these items.20 38 In addition to age and gender, 6 studies collected IMD data, 17 collected sexual orientation and 21 collected ethnicity, the majority of which were described in different ways using a variety of groupings. Gender types captured also varied between studies, with 2 that did not collect these data, and 10 only reporting binary types.
Those who accessed services tended to be majority women (56.7%–69.4% women, five studies reported statistical significance),5 20 32 34–36 39–41 were residents in less deprived areas compared with accessing testing in other settings (p<0.001),5 32 39 40 white or white British (53.3%–92% users, four studies reported statistical significance),5 32 34–36 39 41 and 20 years old or over (95.4% when compared with any age group,20 32 32.0%–42.9% when c.f. people aged 20–2540 42), with two studies reporting statistical significance.20 32
In those studies that collected more comprehensive gender data, people who identified as gender diverse made up a small proportion of the overall population accessing the service (0.0%–0.4%).35 36 41 43–46
There were limited and conflicting data on access according to sexual orientation; one study reported more MSM requesting access than heterosexual men,32 and one study found that a higher proportion of people identifying as non-heterosexual accessed online self-sampling compared with clinic-based testing (OR 0.44, 95% CI 0.27 to 0.72).34 This is in contrast to findings from the Umbrella service, Birmingham.36
Those accessing online services sometimes displayed higher risk behaviours,5 39 but often had a greater proportion of negative test results compared with clinic-based populations.32 33 35 36 Individuals were more likely to order OPSS kits if they had used STI testing services before.39 Of those who were never-testers, a significant proportion was recruited face-to-face in communities.45
Usage of OPSS services
The proportion of users returning self-sampling test kits varied by study (range 48.3%–78.4%).32 35 36 43 Women were more likely than men to access and return STI self-sampling kits in the majority of studies.20 32 35 36 39 40 46 One service evaluation found no difference between kit return rates between those identifying as gender diverse and those identifying as cisgender (OR 1.00, 95% CI 0.81 to 1.24), although successful return (OR 1.6, 95% CI 1.06 to 2.36) and successful testing (OR 1.2, 95% CI 0.87 to 1.66) of blood samples were higher in those identifying as trans or non-binary/gender fluid.43 Characteristics of those who returned test kits varied between studies for age32 36 39 and by level of deprivation.39 46 However, across several studies, people of white ethnicity were more likely to return the kit compared with other ethnicities.32 35 36
A study that evaluated those accessing an OPSS spontaneously, compared with those who attended clinic and were triaged to testing online, found that the return rate was slightly lower in the triage and signpost group compared with the spontaneous online group (67.0% vs 70.5% by 6 weeks, respectively).20
There are limited data on return rate of blood sampling kits, with one study finding only 54.4% (9033 of 16 611) of people returned a blood sample with a sufficient quantity of blood for testing.36 Studies that examined different types of blood sampling kits found no difference between return rates for dried blood samples (DBS) versus mini-tests (MTs) (66.5% vs 68.7%),47 but did find that the samples were significantly more likely to be successfully processed with DBS (94.6%–98.8%) compared with MT (55.7%–54.5%, p<0.001).41 47
Impact of OPSS services on demand
In many areas, the introduction of OPSS services was not associated with a change in numbers of people attending clinics, but increased the overall demand for STI testing services.20 33 44
Impact on clinical outcomes
Test positivity
Overall, test positivity for chlamydia and gonorrhoea was lower in OPSS services (4.4%–8.1%) than clinic-based services (10.3%–14.4%).32 35 Two studies found a low HIV prevalence in their OPSS testing population; 0.1% (144 of 148 257)48 and 0.8% (75 of 16 611)36 of users in the evaluation period had a reactive HIV result. Of these, 65.3%36 and 91.6%48 had confirmatory testing, and 1.3% (1 of 75)36 and 23.6% (34 of 144) had a new diagnosis of HIV confirmed. When comparing DBS and MT for HIV self-sampling, MT was found to have a higher proportion of reactive tests (6.2% vs 0.5%),41 lower proportion of confirmed reactive tests (n=1 of 30 (3.3%) vs 1 of 11 (9.1%))41 and higher false positive tests (5.2%–5.4% vs 0.0%–0.4%).41 47 However, these were service evaluations and the blood sampling kit options were offered sequentially rather than in parallel, so the populations being compared are not directly comparable. In addition, the tests were not compared with the results of a gold standard test (HIV Ab/Ag test), and the authors were unable to provide sensitivity and specificity data.47 These results should therefore be interpreted with caution.
Time to treatment
There were varied results regarding time to treatment; one paper reported that online patients took longer to receive treatment than clinic users,35 and one study found that there was no statistically significant difference.44 When an entire care pathway was trialled online and asymptomatic chlamydia-positive individuals could access an automated online clinical consultation which allowed people to collect their treatment at a community pharmacy, median time to treatment was 1 day (IQR 0–1).49 A study comparing outcomes of asymptomatic service users testing positive for chlamydia via clinic-based services and online found that those diagnosed online were less likely to wait more than a week for treatment compared with those diagnosed in clinic (OR 9.94, 95% CI 2.87 to 34.42).34
Reporting sexual assault and safeguarding outcomes
When evaluating outcomes of those people who reported online a recent sexual assault over a 6-month period in 2020, one service found that 0.5% (n=242 of 45 841) of users indicated they had been a victim of a recent sexual assault, which led to telephone intervention by a clinical healthcare professional. Of these, nearly 80% of people were contacted. However, 41.7% (n=101 of 242) of users stated that they had not intended to report recent sexual assault. Fifteen people had already reported the sexual assault and had been seen by the police or by a Sexual Assault Referral Centre (SARC). One person required a SARC referral, and eight people were referred to a clinic-based service.50 The same service also evaluated their safeguarding outcomes in those aged 16–17 years old, finding that a high proportion of this population (42.5%) met the service criteria for a follow-up telephone call from a health advisor. The most frequent reason that a call was triggered was related to drug and alcohol use (27%). The outcome of 8.5% of calls was a discussion with the child protection team, with 7.0% requiring a referral or discussion with social services.48 There was no evidence as to whether safeguarding opportunities were missed, or an in-depth understanding of the acceptability of providing this information in an online setting.
Acceptability of OPSS services
Qualitative research showed the importance of trust, confidentiality, discretion, reliability, convenience and improved patient choice in ensuring the successful use of OPSS,51 52 and between 71.1% and 98.0% of individuals surveyed expressed that they were pleased with and found these services acceptable.38 44 45
Economics
Although this review did not specifically set out to evaluate the economic outcomes of OPSS services, only one study included any costing data.33 This study, evaluating the impact of online testing across specialist SHS in two London boroughs found that, although there was an increase in the total annual cost of STI testing following the introduction of online testing, the average cost per test and diagnosis decreased.33
Discussion
Although evaluations of OPSS of variable quality were found, we did not identify any large-scale, multicentre robust studies. Available evidence suggests that OPSS services appear to be more likely to be used by, and acceptable to, asymptomatic individuals who are predominately women, over 20 years of age, residents in less deprived areas and of white ethnicities, when compared with clinic-based populations. There is preliminary evidence that people from groups experiencing a disproportionate burden of STIs use OPSS less than other groups. The heterogeneity of the included studies prevented full evaluation of clinical outcomes.
Online services tend to be targeted at asymptomatic individuals who do not have other sexual health needs. The ability for asymptomatic people to manage their care needs remotely is an important and useful contribution to detect symptomless STIs, in order to enable treatment of the index patient and partner notification, and reduce morbidity and onward transmission. However, asymptomatic users reported higher risk behaviours in some studies,5 39 and there were no data on the impact of using OPSS on future sexual behaviour. In addition, there was insufficient evidence to be able to establish the impact of OPSS on treatment and partner notification outcomes.
Women were more likely than men to access and return STI self-sampling kits in the majority of studies.20 32 35 39 40 46 For services that provided accessibility information by sexual orientation, MSM seemed to be successfully using OPSS services.32 46 This finding is consistent with those from an OPSS in Canada.53 Certain minority ethnic groups such as black Caribbean, black African and mixed ethnicities, who are also key populations who are at higher risk of poor sexual health, were under-represented in OPSS users,11 perhaps due to a preference for face-to-face care.52
Some services appear to appropriately reach younger people, but other services were more popular with those aged over 20 years.35 This could be because younger people are more likely to live at home and have concerns about parents finding a test kit delivered through the post.54 Using chlamydia as an exemplar, chlamydia has formed 49% of new STI diagnoses in 2019, yet there has been a 13% reduction in tests completed by young people since 2015.11 Chlamydia is the most commonly reported STI in the UK, and disproportionately affects young people from deprived areas,42 so it is crucial to ensure services are targeting these groups within their region. Despite this, recent research shows that both men (adjusted OR (aOR): 1.36 (95% CI: 1.35 to 1.39), p<0.001) and women (aOR: 1.32 (95% CI: 1.31 to 1.33), p<0.001) living in the least deprived quintile were more likely to use OPSS services for chlamydia screening than those from the most deprived quintile.55
Understanding inequalities in access and usage of OPSS services requires services to collect comprehensive sociodemographic data. Of the 15 included studies, only 2 collected gender, age, ethnicity, sexual orientation and IMD data.32 37 Most studies included categories such as ‘other’ ethnicity or sexual orientation and though a few included trans participants, only one described people of non-binary, gender fluid or other genders.43 This data gap results in not only a skewed understanding of the impact of STIs on minorities, but also ‘facilitates the erasure of communities’.18 Further, the inter-relations between demographic groups have not been sufficiently examined in these studies despite reference in the literature20 42 56 (eg, 4, 11, 65).
Return rates of blood samples that were sufficient for testing were relatively low, and in keeping with findings from the national HIV self-sampling service.57 Overall test positivity was lower in OPSS services compared with clinic-based services.32 36 This is in keeping with, but more marked than, findings from both selective and unselective national datasets.10 57 As highlighted within one study, the low positive predictive value (PPV) for home-based BBV testing is concerning36 and requires further evaluation from both a cost-effectiveness and well-being perspective.
To our knowledge, this is the first review to explore the accessibility of OPSS services in the UK. The inclusion of qualitative as well as quantitative studies ensured that both acceptability and core themes regarding people’s access to and use of services could be explored. The included studies were heterogeneous in design using a variety of methodologies which added value to the review. By excluding hypothetical studies, acceptability and barriers to service use are indicative of the real-life experience of online service users.
Fourteen of 23 studies took place in London and no studies were conducted in Wales, Scotland or Northern Ireland, so findings may not be generalisable to all of the UK. This review did not set out to evaluate partner notification or economic outcomes of OPSS services, but the authors observed that there was a dearth of information on these within the studies that were included in this review. This study only focused on the UK setting as it was focusing on access, and the infrastructure of SHS provision in the UK is different to other settings. However, the findings relating to acceptability and convenience are similar to those reported in systematic review and synthesis of qualitative research on OPSS services.54
OPSS services appear acceptable to current users and improve choice, but evaluation is limited. The existing evidence suggests that successful services achieve reliability, privacy, convenience, trust and are integrated with clinic-based services to provide ease of transition between modalities of care. Online services are successful in relieving pressure from clinics,58 but clinic-based services remain essential for symptomatic individuals, people who have digital constraints and those who prefer face-to-face care and or require additional safeguarding, among others.18 Further research is required to understand impact on clinical outcomes, including safeguarding opportunities.
With the extensive expansion in provision of OPSS services in recent years, a large-scale, multicentre evaluation is needed to determine their cost-effectiveness and impact on access, clinical outcomes and service delivery. In addition to more targeted evaluations, it would be beneficial to conduct a holistic evaluation across all service modalities (including face-to-face services). Clinical outcomes are key to understanding the cost-effectiveness of these services and there is limited research into this important factor. Further research is required to understand why people aged under 20 years have lower uptake, and whether this is related to, for example, an individual’s experience of autonomy, competence and relatedness59 and how awareness and access can be improved for these individuals.60
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Alec Miners
Twitter @KarenCLloyd, @jogibbs76
Correction notice This article has been corrected since it was first published online. 'Clinic' was changed to 'clinical' in the title.
Contributors KS conducted the original scoping review to fulfil requirements of KS’ Masters dissertation, supervised by JG and KCL. JG, KCL, KS, CSE and FB conceived of the original idea. KS, JG and KCL contributed to the design of the study. KS led, and KCL and JG contributed to the establishment of the search strategy and method of analysis. The original article reviewing and data analysis were led by KS, with contribution from KCL and JG. The updated article review and data analysis were led by JG, with contribution from KCL and KS. All authors (KS, KCL, CSE, FB and JG) have made contributions to the drafting and revising of the article, and have approved the final version.
Funding Not applicable.
Competing interests FB, CSE and JG report receiving NIHR funding to research digital sexual health (NIHR129157 (FB, JG) and NIHR200856 (CSE, JG)). CSE and JG are associate editors for STI journal, and have coauthored three papers included within this review.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.