Article Text

Abstract
Sexually transmitted co-infections increase HIV infectiousness through local inflammatory processes. The prevalence of STI among people living with HIV/AIDS has implications for containing the spread of HIV in general and the effectiveness of HIV treatments for prevention in particular. Here we report a systematic review of STI co-infections in people living with HIV/AIDS. We focus on STI contracted after becoming HIV infected. Electronic database and manual searches located 37 clinical and epidemiological studies of STI that increase HIV infectiousness. Studies of adults living with HIV/AIDS from developed and developing countries reported STI rates for 46 different samples (33 samples had clinical/laboratory confirmed STI). The overall mean point-prevalence for confirmed STI was16.3% (SD=16.4), and median 12.4% STI prevalence in people living with HIV/AIDS. The most common STI studied were Syphilis with median 9.5% prevalence, Gonorrhea 9.5%, Chlamydia 5%, and Trichamoniasis 18.8% prevalence. STI prevalence was greatest at the time of HIV diagnosis, reflecting the role of STI in HIV transmission. Prevalence of STI among individuals receiving HIV treatment was not appreciably different from untreated persons. The prevalence of STI in people infected with HIV suggests that STI co-infections could undermine efforts to use HIV treatments for prevention by increasing genital secretion infectiousness.
- HIV
- HIV/STI co-infection
- HIV treatment for prevention
- prevention
- sexual health
- STD
- test and treat
Statistics from Altmetric.com
Sexually transmitted infections (STI) are among the most well-established risk factors for HIV infection. STI facilitate HIV transmission by breaching protective mucosal barriers and recruiting susceptible immune cells (eg, CD4 T-helper cells, macrophages) to the site of infection.1 Ulcerative and non-ulcerative STI also create portals of entry for HIV to access susceptible cells. The association between ulcerative STI and HIV transmission is well established, with as many as half of newly HIV-infected people demonstrating herpes simplex virus type 2 (HSV-2) infection.2 STI can also cause genital bleeding, further increasing the risk of exposure to HIV during sexual activity.3 4 Trichomoniasis and bacterial vaginosis, for example, can increase the risks for vaginal bleeding more than 12-fold.5
Recent research has examined STI in people already infected with HIV. The effects of HIV infection on immunity can increase susceptibility to other STI as individuals who are immune compromised are less able to mount a protective response against sexually transmitted pathogens.6 7 For example, HIV and HSV-2 co-infections are prevalent and both infections can facilitate acquisition of the other. In a study that illustrates the reciprocal relationship between HIV and HSV-2, Tobian et al8 followed 6396 men in Uganda for 2 years and found a 1.09% HIV seroconversion rate in the cohort. However, HIV seroconversion was closely associated with HSV-2 seroconversion; more than half (56%) of HIV and HSV-2 infections occurred in the same time frame. In 25% of cases, HIV infection preceded HSV-2 infection, and in 19% of cases HSV-2 infection preceded HIV transmission.
Sexually transmitted co-infections pose considerable health threats to people living with HIV/AIDS. Syphilis, for example, is related to both increased concentrations of HIV RNA in blood plasma and decreased CD4 cells.9 Viral STI and genital ulcer diseases, particularly HSV-2, are also linked to increased concentrations of HIV in blood plasma and genital fluids.10 In addition, viral STI appear to have a bidirectional pathogenic relationship with HIV; HIV can accelerate disease progression of other viral infections and vice versa.11 When individuals are immune compromised, co-occurring STI are more difficult to treat and symptomatic periods may linger. Finally, local inflammation of the genital tract caused by viral and non-viral STI promotes HIV shedding, therefore increasing HIV infectiousness.12 Unfortunately, multiple sexually transmitted co-infections are common because the pathogens share transmission routes.13
There is growing evidence that antiretroviral therapies (ART) can reduce HIV infectiousness and prevent HIV transmission.14 Studies have reported that under optimal conditions HIV-infected men and women who initiate ART are significantly less likely to infect their HIV-negative sex partners. For example, Vernazza et al15 found that men treated with a suppressive ART regimen and cleared of other STI had a 98% concordance between HIV RNA in blood plasma and semen; men who had undetectable virus in their blood plasma almost always had undetectable virus in their semen. A study by Donnell et al16 reported only one HIV infection among 349 HIV-serodiscordant couples in which the infected partner had initiated treatment. In contrast, there were 102 HIV infections observed among the 3032 couples with untreated HIV-positive partners. These findings encourage the use of ART for HIV prevention. However, all participants in studies examining HIV treatment for prevention receive regular and routine STI screening and treatment services. Similarly, mathematical models that forecast the near elimination of HIV epidemics with universal coverage of HIV testing and treatment do not include population or individual-level STI prevalence in their models.17 Given the substantial role that STI co-infection plays in genital tract HIV viral shedding, projections reported by most models of ART for HIV prevention are probably unrealistically optimistic.18 The prevalence of sexually transmitted co-infections in HIV-infected populations thus has significant implications for expected outcomes of HIV test and treat programmes.19
The purpose of this paper is systematically to review the research on the prevalence of HIV/STI co-infection. We examined the point and time interval prevalence estimates of HIV/STI co-infection in people living with HIV/AIDS to provide a more realistic context for interpreting studies of the test and treat strategy and mathematical models that forecast the effects of ART on HIV transmission. Our review is based on the premise that increased genital infectiousness resulting from co-occurring STI will diminish the positive effects of reducing community-level blood plasma viral load. Our aim is therefore to examine the prevalence of HIV/STI co-infections better to inform efforts to scale up HIV treatment for prevention programmes.
Co-occurring STI and HIV infectiousness
On a population level, concentrations of HIV RNA tend to be lower in genital secretions than blood plasma. However, the relative concentrations of HIV RNA in peripheral blood and genital compartments are reversed when there are co-occurring STI. A review of studies reporting the association between semen and blood plasma concentrations of HIV RNA found an average correlation of 0.44, with associations ranging between no relationship (r=0.07) and nearly perfect (98%) concordance. Studies with the highest correspondence between blood plasma viral load and seminal plasma viral load were those that screened and treated men for co-occurring STI.15 The prevalence of STI and HIV co-infection is therefore probably a significant factor in accounting for the overall low correspondence between HIV in the genital tract and blood plasma.20
HIV concentrations in semen and vaginal fluids are directly associated with the number of leucocytes migrating to the genital tract. A dose relationship exists between leucocyte concentrations, a marker for inflammatory processes, and HIV viral shedding.21 Various STI differ in their impact on HIV shedding, and the same STI can have different effects on HIV concentrations in men and women. Overall, the greater the inflammatory response the greater the impact on HIV infectiousness.21 Gonorrhoea and chlamydia, for example, are associated with high concentrations of leucocytes in the genital tract and therefore greater HIV shedding.21 In addition, bacterial vaginosis increases HIV viral shedding by as much as sixfold.22 Syphilis is associated with HIV shedding in blood plasma as well as the genital tract; blood plasma concentrations of HIV can increase as much as 0.22 log values before syphilis treatment.23 Syphilis is also related to decrements in CD4 cell counts. In addition, treating syphilis improves both blood plasma viral loads and CD4 cells.24 In contrast, human papillomavirus (HPV) does not significantly impact inflammatory responses in the genital compartment and is not associated with HIV shedding.25 26 Similarly, candida infections are not associated with increased HIV shedding.22 Therefore, the STI with the greatest impact on HIV shedding are those that produce genital ulcers and urethral/vaginal discharge, specifically syphilis, chancroid, gonorrhoea, chlamydia, HSV-2, trichomoniasis, bacterial vaginosis, urethritis, cervicitis and cervical mucopus. Our review of studies reporting sexually transmitted co-infections therefore focuses on these STI.
Literature review
We conducted electronic and manual searches for studies that reported STI co-infections among people diagnosed with HIV. Details on review search strategies are available from the authors. We did not include HPV, candida and other infections that have not demonstrated increased HIV infectiousness. Studies of antibodies to STI, particularly HSV-2 and syphilis, do not necessarily reflect recent infection but are included because chronic infections will have a longer lasting effect on community viral load. Our search was restricted to studies reported since 2000 to produce STI prevalence rates relevant to contemporary models that forecast the use of HIV treatments for prevention. The literature search was completed in August 2010 and identified 1652 studies of HIV co-infections, with most concerning AIDS-related opportunistic co-infections unassociated with HIV infectiousness (eg, tuberculosis, HPV, hepatitis, etc). The initial search for HIV co-infection studies was followed by searches within results for key terms, specifically STI diagnoses. We also conducted manual searches of leading relevant journals (eg, AIDS, Journal of Acquired Immune Deficiency Syndromes, Sexually Transmitted Infections, Sexually Transmitted Diseases, AIDS and Behaviour and AIDS Patient Care and STDs). Figure 1 shows the derivation of the 37 studies included in the review.

Results of automated literature search using key terms ‘HIV’ and ‘co-infection’ followed by manual searches within findings in key journals. STI, sexually transmitted infection.
Prevalence of co-occurring STI and HIV
Table 1 shows the summary of 37 studies that report the prevalence of STI in people living with HIV/AIDS. Studies that reported separate prevalence rates by gender were examined separately when possible; 21 samples of men, 12 samples of women and 11 mixed genders. Studies were conducted in Africa (N=3), Asia (N=4), Australia (N=1), Europe (N=7), North America (N=19), South America (N=2) and the Caribbean (N=1). A total of 708 296 people living with HIV/AIDS was included in the studies, with one study, Manning et al,49 accounting for 90% of cases (N=632 264) as it reported time interval prevalence data from STI records of all cases in New York City.
Summary of findings from studies of sexually transmitted co-infections in people living with HIV/AIDS
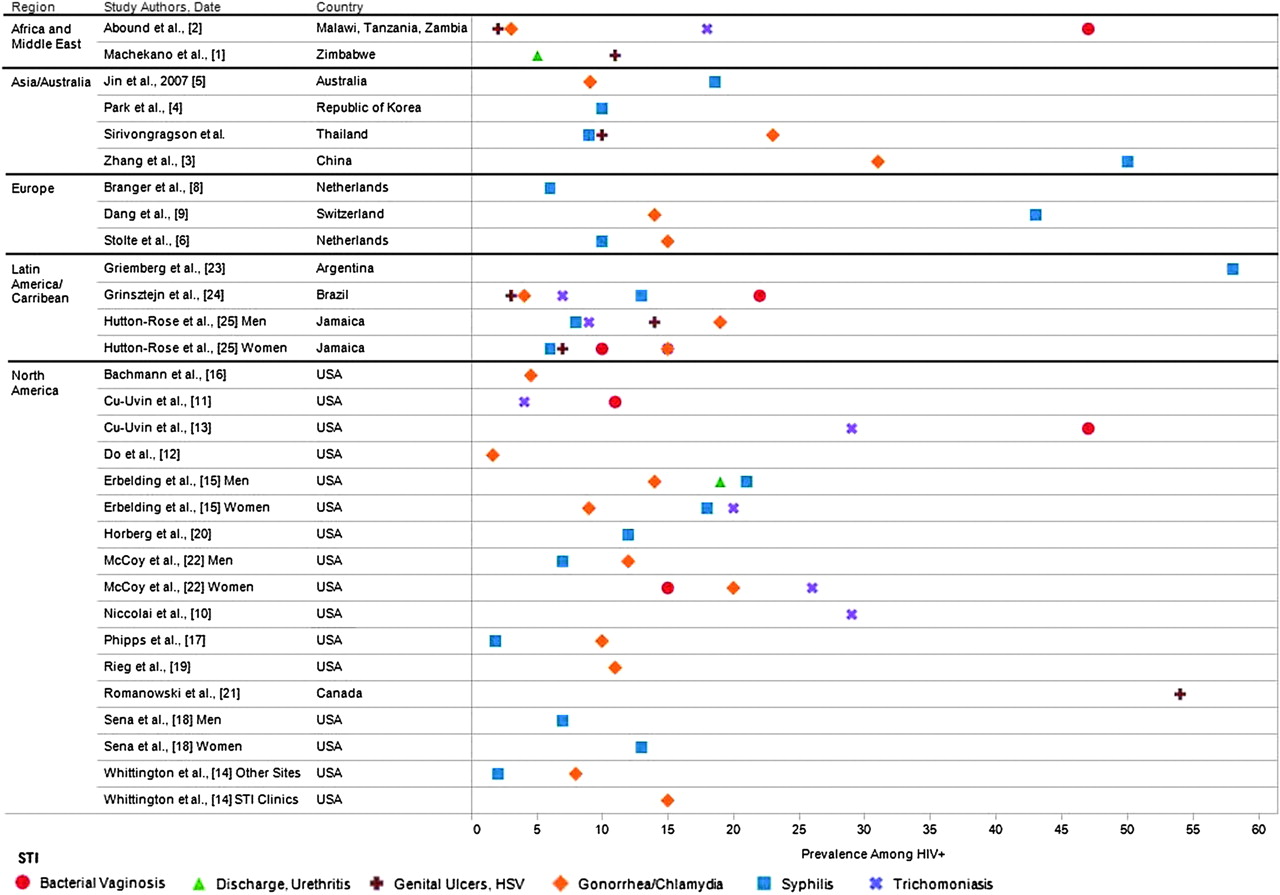
Overall, the studies demonstrated a mean point prevalence STI co-infection of 16.3% (SD 16.4, median 12.4%). Figure 2 shows the point prevalence of individually diagnosed STI segmented by geographical region. The most common STI studied were syphilis with median 9.5% prevalence, gonorrhoea 9.5%, chlamydia 5% and trichamoniasis 18.8%. The figure shows that the highest point prevalence rates were for syphilis, genital ulcers, which included herpes simplex virus and bacterial vaginosis. For studies reporting point prevalence, the mean STI in Africa was 11.3 (SD 4.6), Asia 17.4 (SD 15.3), Europe 14.7 (SD 10.6) and North America 16.1 (SD 18.4). STI prevalence was similar for men (13.6%, SD 10.3), women (15.8%, SD 9.9), t=0.5,23 ns, and was somewhat higher in mixed gender samples (24.0%, SD 30.6). Reports of time interval STI had a mean prevalence of 16.9 (SD 13.88, median 14.0).

{kind=link}
{kind=link}
Prevalence of specific sexually transmitted infections (STI) that have significant effects on HIV genital shedding reported in studies of people living with HIV/AIDS.
Sexually transmitted co-infections over the course of HIV disease
The greatest prevalence of HIV/STI co-infections occur among individuals newly diagnosed with HIV.27 Studies of people who tested HIV positive at the time of STI testing found an average STI prevalence of 19.6%. These studies reflect the importance of STI as reliable risk factors for HIV transmission.42 59 New STI are also often contracted relatively soon after HIV transmission. Erbelding et al45 reported that men contracted a new STI within 415 days and women within 176 days of their HIV diagnosis. However, studies show that STI co-infections occur throughout the years of HIV infection, not just at the time of, or soon after, HIV seroconversion. The average STI prevalence among HIV clinic patients, most of which have been living with HIV for some time, was 14%.
People receiving HIV treatment also demonstrated a significant prevalence of STI co-infections. A total of 14 samples reported ART exposure, with a mean proportion of samples taking ART 67.4% (SD 19.9, median 71%). The overall STI point prevalence in the studies that reported participants receiving ART was 16.2% (SD 23.7) compared with 16.5% (SD 13.3) among the studies that did not report ART use, a non-significant difference, t=0.9,45 ns. Among the samples that reported ART use, there was no association between the percentage of the sample using ART and the prevalence of STI co-infections, r=0.013, ns. Studies also showed relatively stable rates of gonorrhoea infections among people infected with HIV in the USA during the late 1990s when ART was being prescribed early in the course of HIV infection, with diagnoses ranging from 7.6 cases per 1000 person-years to 14.3 per 1000 person-years.42
Methodological limitations of studies of STI among people living with HIV/AIDS
The literature on STI and HIV co-infection over-represents countries in North America and Europe, regions with a relatively low HIV prevalence. The few studies conducted in Africa and Asia therefore limit the usefulness of the literature in informing models that estimate the impact of test and treat programmes in developing countries. Several studies reported aggregate STI that were not the focus of the current review. Rather, we focused our review on studies of STI that are known to increase HIV infectiousness. The literature is also limited by mixed gender samples that do not report gender separate estimates. In addition, STI rates that rely on self-reported symptoms over time intervals are non-specific and were not included. Also of concern are asymptomatic STI that can lead to underestimates of HIV/STI co-infections; one third of syphilis infections in people living with HIV/AIDS are asymptomatic.37 Asymptomatic STI are especially concerning because these infections worsen and increase HIV infectiousness when untreated, and do not alert the person to reduce risk practices.
Estimates of time interval STI were difficult to interpret because studies used a range of periods. It is also unknown if point prevalence estimates stemming from different data sources, such as chart abstraction, clinical diagnosis and laboratory confirmation yield varying prevalence estimates. The literature is also limited by incomplete reporting of HIV disease stage and exposure to ART. The literature is therefore hampered by non-standardised procedures and allows only for a partial picture of the prevalence of STI and HIV co-infection.
Implications of STI co-infections for using treatment for HIV prevention
While HIV treatments reduce blood plasma viral load and may reduce infectiousness, ART does not eliminate the risks of HIV transmission. HIV shedding in the genital tract is well documented in men and women who have undetectable blood plasma viral loads.60 STI among people receiving ART further increase viral shedding and infectiousness. Studies show that the number of people living with HIV who are STI co-infected has increased over the years since access to ART has improved.61 In addition, evidence that ART reduces infectiousness in persons who are HIV/STI co-infected is mixed. Some studies show that ART does not attenuate the association between STI and HIV shedding.22 In contrast, Sadiq et al62 found that men with urethritis who were not treated with ART had a fivefold increase in semen concentrations of HIV RNA relative to men receiving ART.
Ensuring that ART reduces HIV infectiousness will require aggressive behavioural interventions that include STI screening and treatment for all sexually active HIV-infected persons. Treating STI has repeatedly demonstrated reductions in genital tract HIV RNA. Wang et al,63 for example, reported a 3.2-fold reduction in HIV concentrations following the treatment of vaginal infections. However, infrequent screening for STI in sexually active people living with HIV will probably prove insufficient because of the amount of time that people with undetected STI remain infectious. It is also insufficient to rely on sexually active persons to self-detect STI symptoms because as many as one in four STI in people with HIV/AIDS are asymptomatic.51 64 65
Sporadic patterns of sexual behaviour demand a broader definition of patients for STI screening. Clinical visits for monitoring blood plasma viral load in response to HIV treatment offer an opportunity for frequent routine STI screening. Although treatment guidelines are regularly revised, the standard of care is to monitor viral load routinely for people on ART every 3 or 4 months in order to detect viral rebound before the onset of drug resistance.66 All patients who receive ART for HIV prevention should therefore receive routine STI screening in the same monitoring time frame, every 3 to 4 months. In addition, patients receiving HIV treatment for prevention should receive repeated counselling to address erroneous beliefs regarding infectiousness. Risk compensation beliefs are common in response to viral suppression and must be addressed to avoid increases in risk behaviours.67 Patients should also routinely be offered condoms when receiving HIV treatment for prevention. Clinical guidelines should therefore be enhanced to recommend frequent and routine STI screening in the context of using HIV treatment for prevention.
The findings from this review also have implications for mathematical models that forecast the effects of universal HIV testing and treatment for HIV prevention. Models that demonstrate the potential for ART to change the trajectory of HIV epidemics have not included the impact of STI co-infections on infectiousness,68 and are therefore overly optimistic in their projections.69–71 Overall, the potential for ART to reduce genital tract infectiousness will be impeded for at least 15% of persons receiving treatment who contract a new STI. In addition, estimates of treatment effects on HIV transmission vary for vaginal and anal intercourse suggesting that the differential impact of STI will also affect estimates of infectiousness by the route of HIV transmission.72 In addition, economic analyses of the cost-effectiveness of HIV treatment for prevention have not considered the costs for STI screening and treatment. Failure to address ongoing STI/HIV co-epidemics will therefore undermine the potential benefits of using HIV treatment for prevention.
Key messages
Sexually transmitted co-infections are prevalent among people living with HIV/AIDS.
High-rates of co-occurring STI in people living with HIV/AIDS will impede efforts to prevent HIV transmission by using HIV treatments to reduce infectiousness.
Sexual risk reduction interventions are needed for people living with HIV/AIDS to control sexually transmitted co-infections and reduce infectiousness.
References
Footnotes
Funding This project was supported by grants from the National Institute of Mental Health (NIMH) grants R01-MH71164 and R01-MH82633 and National Institute of Alcohol Abuse and Alcoholism RC1AA018983.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.