Article Text

Abstract
Background The UNAIDS Modes of Transmission (UNAIDSMoT) model is increasingly being used to inform national-level HIV priority setting. Although the model is simple to use, important factors may be omitted. Using the UNAIDSMoT model, with Uganda and Cambodia as case studies, we explored the influence of the incorporation of additional factors.
Methods A detailed review of the UNAIDSMoT model was conducted, including reviewing the model structure, data requirements, parameters and assumptions. Country-specific literature reviews were undertaken, along with field visits involving key-informant interviews, to identify the main features of the HIV epidemic in each setting. Adaptations were made to the UNAIDSMoT model to explore the sensitivity of the model projections to these revisions.
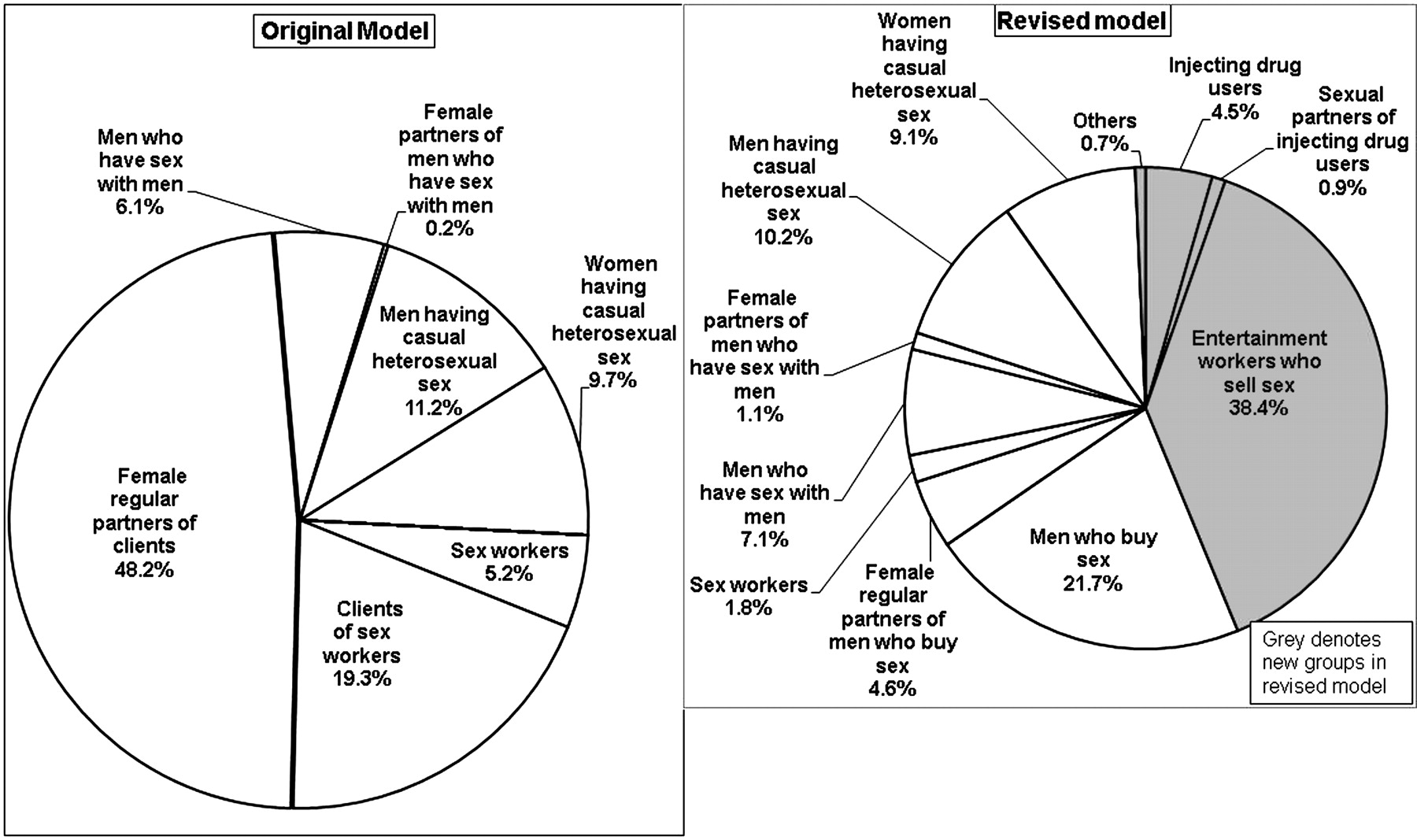
Results A key limitation of the original UNAIDSMoT model is that it does not allow an individual's multiple sources of risk to be considered. The model was adapted to incorporate important multiple risk sources (including injecting drug use), and the effects of the 2008 change in Cambodian law on human trafficking which led to brothel closures, the migration of many sex workers into entertainment venues, and the discontinuation of numerous outreach and condom distribution programmes. As illustrated in Abstract P1-S4.16 figure 1, the revised model projects lower percentages of new HIV infections occurring among sex workers (2% vs 5%) and the regular female partners of men who buy sex (5% vs 48%) than the original model, primarily replaced with new infections occurring in the new groups: entertainment workers who sell sex (38%), and injecting drug users and their sexual partners (5%). In Uganda, the high prevalence of HIV infection among women means that the static model predicts men are more at risk of infection from their female partners than women are from their male partners. This fails to reflect the dynamic chain of HIV transmission.
{kind=link}
Distribution of HIV incidence in original and revised UNAIDSMoT models.
Conclusions Our analysis highlights the limitations of the UNAIDSMoT model, and the potential dangers of over-interpretation of a relatively simplistic and static reflection of a dynamic HIV epidemic (and prevention priorities) at a particular time-point. It is important to regularly re-structure and re-parameterise models according to new data and changes in patterns of risk behaviours. Further research to test the validity, sensitivity and robustness of the UNAIDSMoT model projections in different epidemic settings is needed.