Article Text

Statistics from Altmetric.com
Introduction
This article provides a short summary of the current status of sexually transmitted infections (STIs)/HIV epidemiology in the Asia-Pacific region. Information was requested from WHO as well as from STI experts in a number of major nations in the region. Reliable national STI notification statistics were not available from several of these countries. Figures 1 and 2 plot notification rates for gonorrhoea and syphilis in countries where such figures were available. Varying rates of notification and completeness of data make direct comparison between countries difficult. However, within country trends do provide an idea of the epidemics in the respective countries.
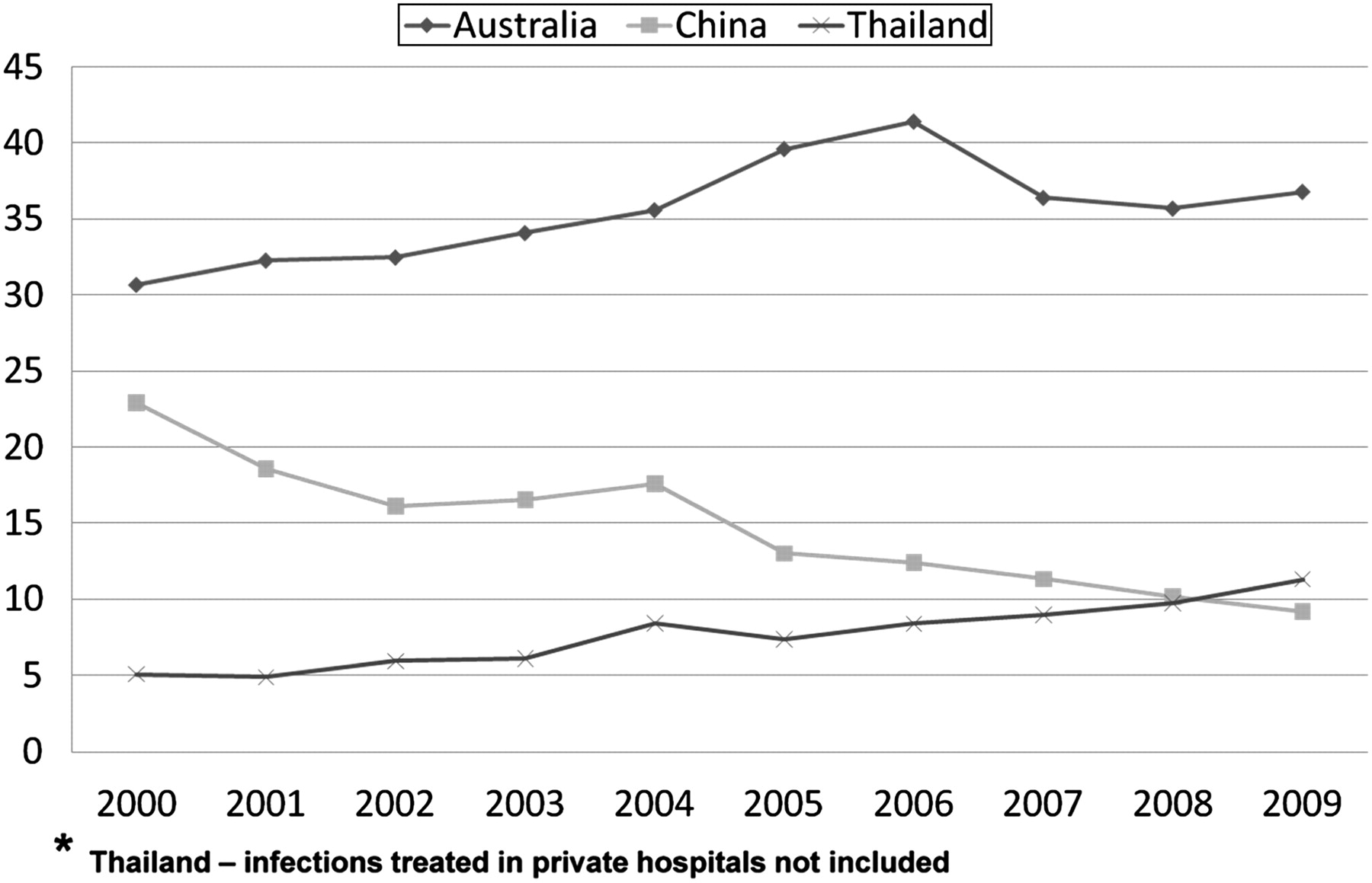
Gonorrhoea notification rates (per 100 000 population).

{kind=link}
{kind=link}
Syphilis notification rates (per 100 000 population).
WHO estimates that in 2005 there were 7.39 and 32.69 million cases of Chlamydia trachomatis in South-East Asia (SEA) and Western Pacific (WP) regions, respectively.1 Estimates for gonorrhoea were 8.37 and 9.43 million cases, for syphilis were 11.77 and 2.54 million cases, and for trichomoniasis were 26.91 and 25.76 million cases for these SEA and WP regions, respectively. The corresponding 2005 incidence rates for chlamydial infections were 6.6 and 41.6 million, for gonorrhoea were 22.7 and 26.9 million, for syphilis were 2.9 and 1.1 million, and for trichomoniasis were 38.6 and 39.1 million, respectively. The total for these four infections was 70.8 million for the SEA region and 108.7 million for the WP region giving an overall total of 179.5 million. The Asia and Pacific region had by far the greatest number of curable bacterial STIs of all the global regions.1
UNAIDS estimates that in 2007 there were 700 000 people living with HIV in China, which was up from 470 000 in 2001.2 National notification rates for gonorrhoea have fallen but syphilis has increased over the 10 years from 2000–2009 (Chen XS, personal communication, 2010). Syphilis infection in sex workers ranges from 8.8–9.5% in the Yunnan province to 8% in Guangdong to 3.5% in Beijing (Chen XS, personal communication, 2010). Condom use rates are still generally unsatisfactory—for example, only 53.9% and 50.3% used condoms consistently in the Yunnan province and Beijing, respectively (Chen XS, personal communication, 2010). Men who have sex with men (MSM) have been identified to be at particularly high risk—a meta-analysis of infections among MSM estimated national prevalence of HIV infection to be 2.5% (95% CI 0.9 to 3.3) and syphilis prevalence of 9.1% (95% CI 7.6 to 10.8).3 A study on MSM in Beijing in 2006 yielded incidence rates of 2.6 per 100 person-years for HIV, 16.9 per 100 person-years for syphilis and 3.3 per 100 person-years for hepatitis B virus. In a 2006 study on MSM in the Jiangsu province, the prevalence of gonorrhoea was 2.7%, chlamydial infection 8.0%, non-gonococcal urethritis 27.7%, active syphilis 6.9%, hepatitis B virus infection 9.1%, herpes simplex virus 2 infection 7.8%, and genital warts 13.2%.4
The HIV epidemic in India has stabilised in recent years. According to the Indian National AIDS Control Organisation (NACO) the number of people living with HIV has declined from 2.73 million in 2002 to 2.27 million in 2008; estimated adult prevalence fell from 0.45% and 0.29% over the same period. HIV prevalence among pregnant women in the age group of 15–24 years also showed a declining trend. However, there is high prevalence among high risk groups: injection drug users (IDU; 9.2%), MSM (7.4%), female sex workers (4.9%) and sexually transmitted disease (STD) clinic attendees (2.5%).5 There is no fully functional STI surveillance system in India—estimates depend on ad hoc surveys often among facility based or convenience samples. The general consensus is that syphilis and gonorrhoea are declining, and chlamydial infections, human papillomavirus and herpes genitalis are increasing. However, the decline in the prevalence of bacterial STIs should be interpreted with caution as this may reflect the improved facilities of syndromic treatment in the peripheral centres that reduces the need of many patients to attend STD clinics in tertiary centres. According to national Behavioural Surveillance Survey (BSS) results, condom use among MSM has increased from 2001 to 2006 in most major cities for female as well as male partners. Similarly more heterosexual respondents reported consistent condom use with non-regular sex partners (42% vs 27%) and with sex workers (74% vs 57%) over the same period.6
Disease notification over the last 10 years in Australia indicates stable figures for HIV infection (4.1 per 100 000 in 2008), gonorrhoea (36.8 per 100 000 in 2009) and non-infectious syphilis (6.4 per 100 000 in 2009), but increasing notifications of chlamydia (286.4 per 100 000 in 2009) and infectious syphilis (6 per 100 000 in 2009).7 8 As is the case in other industrialised countries, most HIV and infectious syphilis infections occur in MSM. Behavioural data for MSM have shown relatively stable rates of unprotected anal intercourse with casual partners in Melbourne between 2004 and 2008, whereas Sydney showed a decreasing trend and Queensland showed an increasing trend.9
In Thailand, the prevalence of HIV infection has been decreasing in the last 10 years: pregnant women from 1.46–0.65%, among direct sex workers from 18.46–2.76% and among indirect sex workers from 6.56–1.71% in 2000 and 2009, respectively. The prevalence of HIV in MSM has decreased from previous surveys to 24.7% in Bangkok, 8.3% in Chiangmai and 6% in Phuket in 2009. A national STI reporting system has been in place in Thailand since 1967. The notification rate of five reportable STIs in public STI clinics increased from 25.2 per 100 000 population in 2002 to 37.22 per 100 000 population in 2009, the highest in 10 years. The rise has been attributed to an increase in unprotected sex among young persons, an improved surveillance system and revitalisation of STI clinics. It should be noted that these figures do not include STI cases treated in private clinics and hospitals or self-treated with antibiotics from drug stores.
Indonesia has reported a significant increase in HIV infections over the last 10 years from 607 in 2000 to 19 973 infections in 2009. Most infections are among heterosexuals (50.3%) and IDU (40.2%); the provinces with the highest number of infections are in Java, Papua and Bali. However, infections among MSM are increasing rapidly—34% of transgenders and 8.1% of MSM tested in Jakarta in 2007 were HIV positive. Surveys among direct sex workers in nine cities in 2009 showed chlamydia infection in 41.8%, gonorrhoea in 34.5%, syphilis in 7.2% and HIV infection in 8.1%.
Acknowledgments
I would like to acknowledge the contributions of Francis Ndowa from WHO, Chen Xiangsheng from the National Centre for STD and Leprosy Control in China, Sunil Sethi from the PGIMER in Chandigarh, India, Christopher Fairley from the University of Melbourne in Australia, Angkana Charoenwatanachokchai from the Ministry of Public Health, Thailand, and Sjaiful Daili from the University of Indonesia.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.