Article Text

Statistics from Altmetric.com
Introduction
In the USA, approximately 19 million new cases of sexually transmitted infections (STIs) occur annually,1 primarily affecting adolescents and young adults.2 Direct and indirect costs to the USA for STIs are estimated to be $10–17 billion dollars per year (table 1).3 Issues of health inequity and health disparities make STIs a prime target for management and control. STIs present numerous barriers to routine clinical care and diagnosis because of the associated stigma, costs and confidentiality issues. Furthermore, even if tested, many infected patients (30%–74%) never return for routine test results or are lost to follow-up for treatment.4
Estimated annual burden and cost of STDs in the USA
In Canada, between 1997 and 2007, both the number and rate of reported cases increased for chlamydia, gonorrhoea and infectious syphilis.5 All three STIs increased more dramatically among middle-aged adults.
Age and health disparities
Age
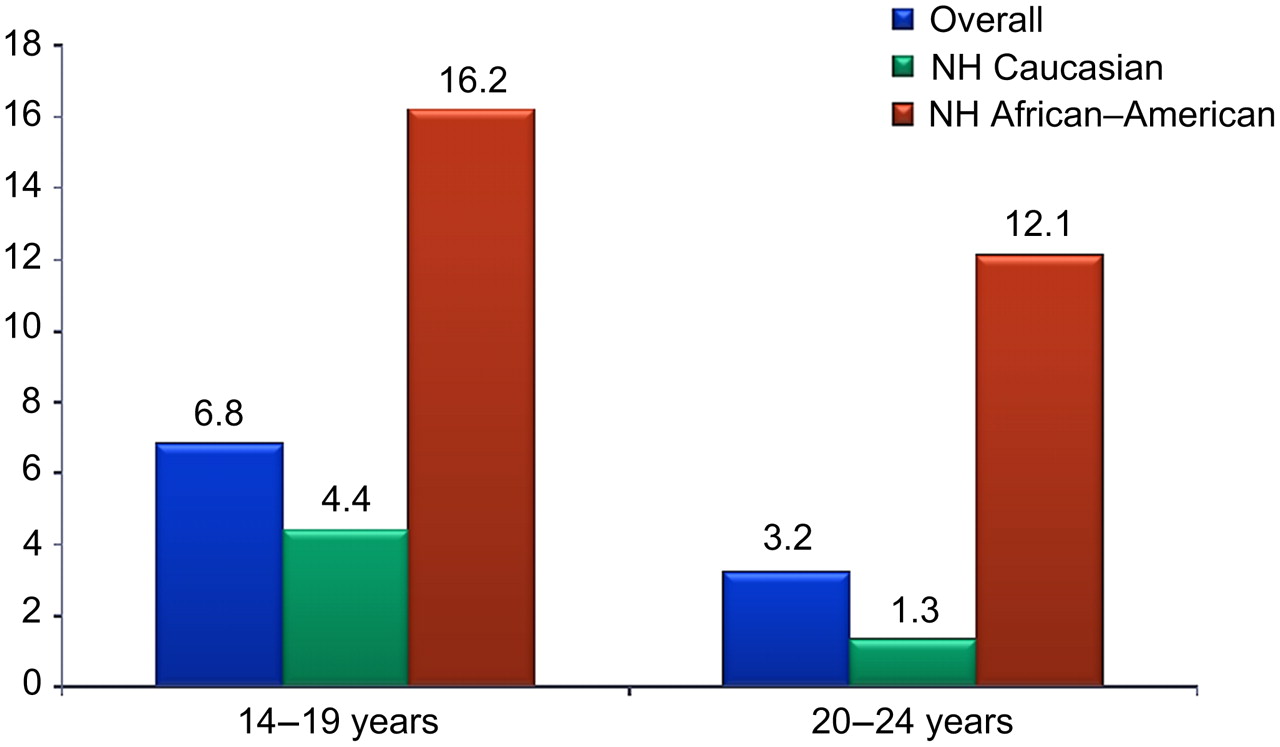
Youth of the USA represents the most vulnerable population and bears much of the burden of sexually transmitted disease (STDs). Studies indicate that one in four sexually active adolescents will acquire an STD (figure 1). The chlamydia rate in the young adolescents is astounding: 3329.3/100 000 and 3273.9/100 000 in 15–19 and 20–24 years women, respectively, versus 1234.0 and 511.7/100 000 for ages 25–29 and 30–34 years, respectively.2

{kind=link}
Chlamydia prevalence in sexually active women 14–24 years in the USA by age and race. NH, non-Hispanic.
In Canada, between 1997 and 2007, chlamydia rates increased by 86.8% among adults aged 15–29 years (p<0.0001) and 165.9% among adults aged 40 to 59 years old (p<0.0001).5 Similarly, the increases for gonorrhoea were 133.3% (p<0.0001) and 210.2% (p<0.0001), respectively. Syphilis rates increased fivefold among younger adults compared with an increase of 11-fold among middle-aged adults (p<0.0001) since 1997.5 The reported rate ratios (younger:middle age) decreased over time for chlamydia (p<0.0001), gonorrhoea (p<0.0001) and syphilis (p=0.005). Men were disproportionately represented among reported chlamydia, gonorrhoea and infectious syphilis cases, constituting 59.8%, 87.6% and 93.0% of middle-aged adult cases, respectively, in 2007.5
Race
In the USA, STIs are a serious problem in African–Americans and ethnic minorities,6 resulting in major health disparities and inequities.2 For example, rates of infection in 2009 in black women for chlamydia are 7.8 times higher than in white women. Rates of infection in 2009 in black women for gonorrhoea are 17 times higher than in white women. Similar disproportionate burdens are noted for black men also. Primary and secondary syphilis rates show vast disparities in men (31.3 in black men vs. 3.9/100 000 in white men).2
HIV risk
Trichomonas, which is not reportable to Centers for Disease Control and Prevention (CDC), has recently been shown to be associated with HIV transmission7 and is also associated with poor reproductive outcomes.8 Understanding the pathophysiology and epidemiology of STIs is a critical step in developing rational diagnostic, treatment and control strategies. STIs have been conclusively linked to increased risk of HIV transmission and acquisition.9 Therefore, their control and management are intrinsically linked to prevention and control of HIV.
Traditional disease control programme approaches have included clinic-based screening and partner notification. These have been supplemented by newer approaches to community-based STI control, which include use of computerised disease surveillance systems, geographic mapping and use of non-invasive new diagnostic techniques and population-based screening in the non-clinical setting. This review will cover issues of the control of STIs and their management in North America, especially as they relate to successes and failures as well as innovative new ideas of control. Areas that are paramount to understand and acknowledge, as they relate to understanding STIs and their control, include: epidemiology, behaviour, diagnosis, treatment, vaccination, education of patients and education of providers.
Epidemiology and behaviour
Understanding the epidemiology of STIs as it relates to behaviour is critical to developing effective control and management strategies. STDs are unique in the infectious disease arena, in as they are completely dependent on behavioural factors for transmission. Critical to individual patient management involves taking a good sexual risk history, yet many primary care clinicians in the USA do not even ask their patients if they are sexually active.10 In a survey of 718 patients in a adult care clinic about their provider, 44% had never been asked about sexual health by their provider, 18% had never had a gender-specific genital exam, one third had never been tested for HIV, 33% stated they would not use a condom at next sexual act and 32% were uncomfortable discussing STIs with their provider.10 Education of primary care clinicians about STIs, their diagnosis, treatment and management is often needed.
Diagnosis and treatment issues
Rapid and accurate diagnosis and correct treatment are of critical importance in the control of STIs in the USA Diagnostic approaches have been revolutionised by such techniques as nucleic acid amplification tests. These assays have simplified diagnosis because they have facilitated the use of non-invasive specimens such as urine and self-obtained vaginal swabs, which have allowed population-based surveys outside the clinic and that provide a more accurate picture of the STIs in the general population than do clinic-based surveys.11 12 The National Health and Nutrition Examination Surveys1 have increased our knowledge of asymptomatic infections, as well as our understanding the true prevalence of STIs on a population basis. Both issues of diagnosis and treatment add knowledge as to how to design control and management strategies. Diagnostic issues that can augment control issues include the development and use of newer rapid point-of-care diagnostic tests (POCTs). These provide an immediate diagnostic result in a few minutes or within an hour. POCTs have advantages over lengthy standard diagnostic tests because they can provide an immediate diagnosis, interrupt transmission and facilitate delivery of timely prevention and counselling messages. Availability of POCTs can empower persons to ask to be tested for STIs or potentially even perform such a POCT themselves.13 14 Surveys have demonstrated that clinicians desire POCTs with specific qualities.15 16 Sadly, we have few good Federal Drug Administration-approved POC tests,17 other than for HIV and trichomonas in the USA,18 but several promising ones are in development.19 20
Treatment has become more complex because of the emergence of antimicrobial resistance, especially for gonorrhoea, which may soon become untreatable.21 Education of providers as to the proper use of the recommended treatment strategies is paramount in preventing transmission of STIs. Treatment guidelines are issued every 2 years by the CDC to facilitate proper treatment strategies.22
Education
Since STI rates are disparate and unequal among youth and in African–Americans in North America, special education tools are needed to address the ‘Hidden Epidemic’.23 Many persons, especially adolescents, and even clinicians are reluctant to discuss sexual health issues openly because of the social implications, issues of privacy and confidentiality.10 Barriers for clinicians and patients exist in getting persons tested for STIs. Focusing on sexual health rather than sexual disease is one solution to addressing these epidemics.24 However, there are barriers for both clinician sand patients to be overcome. For patients, barriers include lack of reimbursement for time required, lack of awareness that patients are sexually active and lack of knowledge that screening can be performed with non-invasive samples without a pelvic exam. For patients, barriers include inability to pay co-payments of the diagnostic test and lack of knowledge of the asymptomatic nature of STIs, high prevalence and possible adverse long-term reproductive effects of STIs.
Many clinicians are not aware that the CDC, the US Preventive Services Task Force and other professional organisations recommend screening for chlamydia in all sexually active women <25 years and in those ≥25 years with STI risk factors.25 26 In the USA, we estimate that <50% of all women who should be screened are being screened for chlamydia (online supplementary figure 3).
Behaviour and control interventions
Assessing sexual behaviour is critical to the development of behaviour and disease control interventions. Major challenges in designing and implementing intervention strategies include using appropriate assessment tools, defining an individual's or population baseline status and implementing the intervention. In the USA, a number of large cross-sectional national surveys have been very useful in assessing behaviour and trends. These have included the National Health and Nutritional Examination Surveys, the Sexual Behaviour, Sexual Attraction and Sexual Identity in the USA: data from the 2006 to 2008 National Survey of Family Growth and the Youth Risk Behavioural Surveillance.1 27 28 Trends in these data strongly suggest that the overall median age of sexual debut has stabilised at 15.5–16 years. Nationwide, 46.0% of high school students had ever had sexual intercourse, and prevalence of sexual intercourse was higher in African–Americans (65.2% vs 42.0% in Caucasians).28 By grade, ranges were 31.6% of 9th graders to 62.3% of 12th graders. Among 34.2% currently sexually active youth, 61.1% reported that they or their partner used a condom at the last intercourse.28 Data from the National Survey of Family Growth demonstrated that among adults aged 25–44 years, about 98% of women and 97% of men ever had vaginal intercourse, 89% of women and 90% of men ever had oral sex with an opposite-sex partner, while 36% of women and 44% of men ever had anal sex with an opposite-sex partner. More women (13%) than men (5.2%) reported same-sex contact in their lifetime.27 Knowledge of these behaviours is important to designing control methods.
In Canada, data from the 2005 Canadian Community Health Survey were used to examine sexual behaviour risks by geography and age in British Columbia.29 Outcomes investigated were ever diagnosed with an STI and did not use a condom during the last sexual intercourse. Region was categorised as metropolitan (northern, remote) and non-metropolitan (southern). In adjusted multivariate analysis, older age (25–49 years) and being female were significantly associated with previously having an STI and not using a condom during the last sexual intercourse.29 When stratified by region, the relationship between older age and not using a condom was particularly strong in northern non-metropolitan regions. The results indicate the importance of considering older age individuals in the design of STI preventive interventions, particularly in non-metropolitan and rural and remote regions, where access to testing and treatment may be limited.29 Socioeconomic status has been linked to increased incidence of STIs in a number of different settings, including rural and urban areas in the US areas.
Interventions to reduce the STI exposure
Promoting condom use has been one of the central tenets of the HIV and STD risk-reduction strategy in the USA. Many programmes have developed to ensure marketing and wide distribution of large numbers of condoms, and instructions for condom use have been part of the national STD guidelines since 1989. Condoms are effective when used correctly and consistently in reducing the risk of STIs,30 including HIV.
Behavioural models
When developing STD/HIV interventions specific to the North American population, behavioural models are necessary for their design and evaluation. Behavioural models are deterministic constructs of sexual behaviour.31 These constructs are usually delineated in sequential steps, with each step being (1) an environmental factor, (2) a behavioural attitude (eg, positive or negative attitude for condom use), (3) individual's area knowledge or (4) a previous behaviour. Risk behaviour is a necessary precursor step to acquisition of an STI. These contextual behavioural elements affect the outcome or the end result being a risky behaviour or a prevention behaviour.
Temporal sequence is also important to model development and interventions. The stages-of-change theory is a construct that has been used in a number of interventions, including the widely reported project RESPECT (risk-reduction counselling to prevent HIV and STDs) in the USA.31 32
Implementation guides for healthcare providers
Guides for clinicians can provide practical information and tools for encouraging providers to screen and manage patients with STIs and to assist with practical tools to enhance screening for STIs. One popular guide in the USA is ‘Why screen for Chlamydia? An implementation Guide for Healthcare Providers’.33
The guide offers practical management techniques including sexual history taking, testing and counselling, treatment, patient management, and partner notification. Other resources for STI healthcare providers are available at http://www.prevent.org/ncc and include learning materials and guides such as healthcare for adolescents; materials for professionals and tribal healers; Safe in the City, a video, intended to promote condom use; and tips for youth confidentiality.
Partner notification
Sexual partners with sexual contact with patients within 60 days should be notified to seek healthcare about exposure to an STI. Traditional partner notification methods have been used successfully previously, especially for syphilis. This has been particularly challenging in North America, especially in environments where partners are inaccessible, such as where commercial sex workers or gay men with anonymous partners are operative.
Most health departments in the USA no longer have resources for partner notification except for gonorrhoea, syphilis and HIV. Using a disease intervention, specialist is labour intensive and costly in today's shrinking budgets. Several internet accessible methods of notifying partners about exposed to an STI have become popular in the USA; most widely in use is InSPOT.34 35 Also available are CDC's e-cards (http://www2a.cdc.gov/ecards/message/message.asp?cardid=292).
Expedited partner therapy (EPT) may be an alternative in some locations in the USA.36 In some states, it is legal for a diagnosed patient to deliver medications or a prescription directly to sexual partners without the partner being clinically assessed. EPT may be especially beneficial in situations in which the patient is doubtful a partner will seek medical care.36 The practice is growing in the USA, and it is now legal or permissible in many states. Legal status of EPT can be found at http://www.cdc.gov for each state.
Innovative STI control methods
Treatment to control transmission
Another modality for controlling transmission of STIs has been the use of treatment regimes. Once-daily valacyclovir to reduce the risk of transmission of genital herpes has been shown to reduce transmission to partners.37 For HIV, a recent report demonstrated prevention of HIV transmission in 1763 serodiscordant couples with early antiretroviral therapy.38 Future studies will add much information for using treatment to control STIs/HIV.
Vaccination to prevent human papillomavirus transmission and prevent cervical cancer
One of our most recent and potentially most successful control programmes for STIs is the vaccine initiative to vaccinate young women against acquisition of human papillomavirus infections, thereby preventing cervical cancer.39 40 Challenges require endorsement by governments and policy makers, affordable prices and education at all levels, to overcome barriers to vaccination.41
Home collection of urogenital specimens
There has been recent interest in using samples collected at home for direct mailing to a laboratory for testing, thereby by-passing the clinic for routine screening, when an individual does not have symptoms. Although home collection is not yet Federal Drug Administration cleared, the focus of current research has shown that vaginal swabs can be collected at home and sent through the US mail to a laboratory for testing.42 43 Two on-going studies—I Want the Kit (IWTK) http://www.iwantthekit.org/female/default.html and I Know https://www.dontthinkknow.org/—have recruited women through specially designed websites that offer education and a home collection kit.44–47
Future considerations
According to the new Affordable Care Act in the USA, primary care clinicians and health directors in Federally Qualified Health Centers will be essential in the provision of routine STD and HIV testing and care. Diagnosis and treatment of STIs will shift from specialty STI clinics to primary care clinicians who will require training from STI clinic personnel. Since preventive services keep people healthy and reduce future healthcare costs, especially with regard to STIs and HIV, education will need to be centred on the US Federal Health Reform. The new Affordable Care Act requires Private Health Plan Coverage for Sexual Health Preventive Services. These include chlamydia tests for all sexually active women ≤24 years, all pregnant women and all women at high risk who are ≥25 years, as well as gonorrhoea and syphilis testing for women at risk; syphilis and HBV tests for pregnant women; and HIV tests for all high-risk adults and adolescents. Primary care clinicians in such Federally Qualified Health Centers will need training to raise awareness and acquire necessary skills to institute screening for sensitive issues such as STIs/HIV. We have much work ahead in trying to achieve better sexual health in North America.24
Key messages
Approximately 19 million new cases of sexually transmitted infections occur annually in the USA, costing $10–17 billion dollars a year and primarily affecting adolescents and young adults; the prevalence continues to increase.
Sexually transmitted infections present barriers to clinical care, diagnosis and management because of the associated stigma and confidentiality issues.
Youth, African–Americans and ethnic minorities represent the most vulnerable population and bear much of the burden of sexually transmitted infections in North America.
Understanding the biology and epidemiology of sexually transmitted infections is a critical step in developing rational diagnostic, treatment and control strategies.
Areas that are paramount to understand for successful control and management of sexually transmitted infections include sexual behaviour, behaviour modification models, new diagnostics, accurate treatment, vaccine availability and provider/patient education.
References
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.