Article Text

Abstract
Background The objective of this paper is to review literature in order to calculate regional estimates of the average duration of time individuals maintain a specific high-risk behaviour.
Methods The review targeted the key populations of female sex workers (FSW), male clients of female sex workers (MCFSW), people who inject drugs (injecting drug users (IDU)) and high-risk men who have sex with men (MSM). To be included in the review the study had to provide information on (1) the time a person spent at risk until death or cessation of the risk behaviour, (2) the percentage of the sample who initiated the risk behaviour in less than a year or (3) the mean or median duration of the behaviour from a representative sample.
Results 49 papers were found for the FSW population describing the period of time FSW stay in sex work to be between 2.9 years (Asia) and 12 years (Latin America). Eight papers were found for MCFSW showing the duration of the risk behaviour in this category varying from 4.6 years in Africa to 32 years in Asia. 86 papers were reviewed for the population of IDU showing that the average time a person injects illegal drugs varies from 5.6 years (Africa) to 21 years (South America). No information was found for duration of high-risk behaviour among MSM; instead, the definitions found in the literature for high- and low-risk behaviour among MSM were described.
Conclusions There is high variability of estimates of duration of high-risk behaviours at regional level. More research is needed to inform models and prevention programmes on the average duration of time individuals maintain a specific high-risk behaviour.
- Injecting Drug Use
- Prostitution
- HIV
- Gay Men
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
Public health policies must be based on estimates that can support informed decision making and guide HIV prevention resource allocation. The extremely dynamic nature of the HIV epidemic and the various forms it takes in different countries challenge public health managers to find ways to accurately monitor and evaluate its trends. Mathematical modelling plays a central role in this process. It contributes to the understanding of the dynamics of HIV spread, provides the information needed to guide responses, helps to identify gaps in existing knowledge and suggests directions for future research.1
The Joint United Nations Programme on HIV/AIDS (UNAIDS) develops models (Spectrum2 and Estimation and Projection Package (EPP)3) to analyse HIV epidemics and their impacts for incountry application. These models allow countries to estimate HIV incidence, HIV prevalence, numbers of people living with HIV, numbers of AIDS related deaths, numbers of people in need of antiretroviral therapy (ART), numbers of HIV-positive pregnant women in need of ART prophylaxis and numbers of children orphaned by HIV, along with other programmatically relevant outputs.
In concentrated epidemics, HIV tends to be focused in a small number of groups with elevated behavioural risk of HIV and their immediate sexual partners. Thus, models of such epidemics must be largely based on information about those key populations: injecting drug users (IDU), high-risk men who have sex with men (MSM), female sex workers (FSW) and their clients (male clients of female sex workers (MCFSW)). However, these populations are often not static. Each year some individuals initiate the behaviours that place them in a behavioural risk group, while others terminate these behaviours, leaving the group; that is, the groups have turnover. Such turnover has significant impacts on the prevalence and incidence in the at-risk population and also in the typically lower-risk populations to which they return.
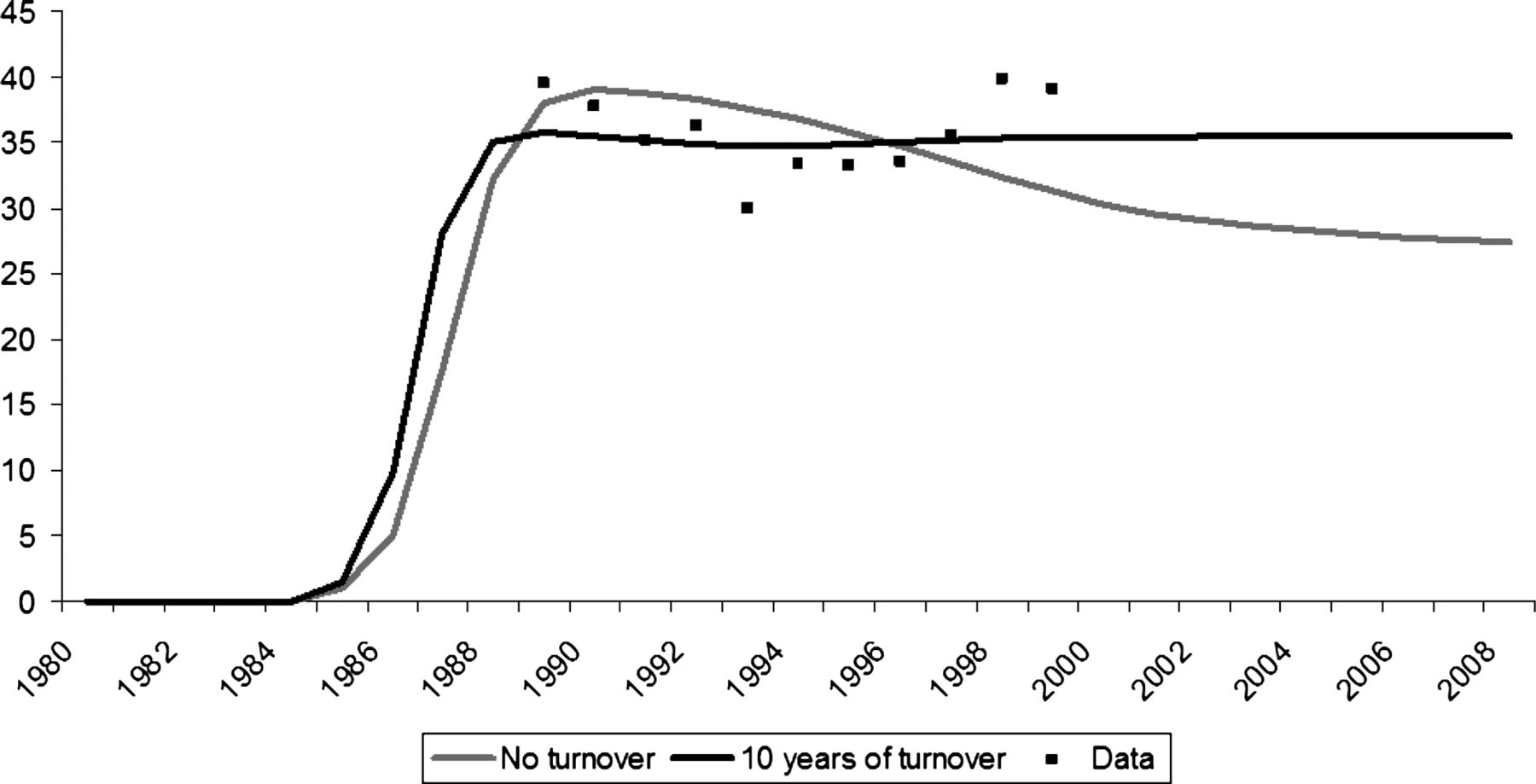
Because those entering an elevated risk population are typically coming from a lower-risk, lower prevalence group, they tend to dilute the current prevalence in the at-risk population. Similarly, those leaving the group are often a higher prevalence than the group as a whole because many of them have longer histories of exposure to risk. Both of these effects mean that in order to maintain a fixed prevalence level in an at-risk population, the incidence in the at-risk population must be higher than it would be otherwise. If models are to correctly estimate the incidence in the group for a given pattern of prevalence, then they need to account for these effects. When turnover effects are included, the prevalence curve over time is generally found to flatten out relative to what it would be with no turnover (see figure 1). This is because most HIV mortality that would normally bring down the prevalence in a closed population occurs outside of the at-risk population if the turnover is high, leading to a flatter curve.

{kind=link}
HIV prevalence (%) in the injecting drug users (IDU) population by year and turnover input, Thailand.
In addition, if the prevalence in the group is high, substantial numbers of those leaving the group and returning to a lower-risk population are HIV-positive. This drives prevalence up in the receiving population without incurring additional incidence. In some cases, 10%–20% of the overall prevalence in the receiving population may result from risk behaviours which occurred outside of that population.
It is essential in concentrated epidemics that models take this into account. Recognising the importance of turnover, the UNAIDS EPP allows users to specify turnover in specific populations. This is done by specifying three things: (1) that turnover does occur in this population; (2) the average time, that is, duration that individuals remain in the at-risk population; and (3) the lower-risk population to which they will return.
This creates additional data needs for concentrated epidemics where turnover is high and is affecting epidemic dynamics. In addition to data on the size of key populations, data are also required on the average time that people remain in the group. That is, one needs to know how many years a person injects drugs, how many years women stay employed in sex work, how many years MSM engage in unprotected, high-risk anal sex and how many years an MCFSW remains a client. The expectation is that, on average, at the end of that time period a person returns to a lower-risk population group, stopping the behaviours that put the person at a higher risk of contracting HIV.
In 2009 and 2010, the estimated average duration was based on experts’ opinion because currently countries have very little data on such movements of people in and out of the populations. But given the great impact that this can have on incidence and prevalence, it is critical that the durations used in such models be based on scientific evidence. The objective of this paper is to conduct a review of the literature to generate regional estimates of the average duration that individuals maintain a specific high-risk behaviour before returning to a lower-risk population.
Methods
The study is a literature review that aimed to compile the limited available data on duration of high-risk behaviour among key populations.
The review was performed using PubMed in October 2010. To identify additional pertinent publications, the references listed in the papers found in the search were hand-searched and researchers were contacted to obtain non-published information. Grey literature was also reviewed.
The studies had to meet the following criteria to be included in the review: (1) to be an original work instead of a literature review; (2) to be studies of one of the key populations important in concentrated epidemics (high-risk MSM, IDU, FSW and MCFSW); and (3) to include information on the duration of risk behaviour or information that could be converted into estimates of duration. Papers in English, Spanish, French and Portuguese were searched with no limits on date. The following search criteria were used:
-
FSW: ((((((((sex workers[Title]) OR sex worker[Title]) OR commercial sex worker[Title]) OR commercial sex workers[Title]) OR sex-trafficked women[Title]) OR prostitutes[Title]) OR prostitution[Title]) OR duration sex work[Title]) OR sex work[Title]
-
IDU: idu[All Fields] OR (inject[All Fields] AND “drugs”[All Fields]) AND users[All Fields] OR (inject[All Fields] AND “drugs”[All Fields] AND user[All Fields])
-
MSM: high [title] AND risk [title] AND “men who have sex with men” [title]
-
CFSW: (“clients”[Title/Abstract] AND prostitutes[Title/Abstract]) OR (“clients”[Title/Abstract] AND (“female”[Title/Abstract] AND “sex”[Title/Abstract] AND workers”[Title/Abstract]
Information on the study design, year of data collection, location, turnover, sample definition, age and gender was collected and summarised in tables that can be accessed online as supplementary tables for this paper (see online supplementary tables S1, S2 and S3).
The ideal studies to assess duration of high-risk behaviour would be surveys of former members of these key populations. The question asked would be how long they had engaged in the high-risk behaviour. In the literature review, for all groups except for IDU, no papers on former members of these key populations were found. Hence, instead of searching for data from which to actually estimate average duration of behaviour, it was necessary to search for data from surveys of current key populations that included information indicating how long the respondent had been at risk. This information was given in three different ways, depending on the study. Some authors calculated the mean or median time the respondents had been at risk, some demonstrated the percentage of the sample who started the risk behaviour in the last year and a few described the duration of the behaviour as the amount of time a person spent in the risk behaviour group until death or cessation.
Because of the diverse presentation of results, it was necessary to create an algorithm to decide how to use the results and choose the best estimate for each region. The first method of choice was direct estimation of duration (the time a person spent at risk until death or cessation of risk behaviour). This required that the person had already discontinued the behaviour that put them in that group.
If the first method was not available, the second method of choice would be used. This consisted of estimating the duration of risk behaviour by the percentage of the sample who initiated the risk behaviour in less than a year. If the population is not changing size, that is, is in a steady state, this percentage will equal the percentage who stopped the behaviour in the last year. In a steady state the entries must equal exits and thus the duration will be 1/(the proportion), so if 10% entered, then the average duration will be 1/0.1=10 years.
If data to apply the first two methods were not available, a third method was used to estimate turnover. The third method consisted of doubling the median or mean time the people remained in the risk behaviour group in the moment of the study interview. This assumes that the duration of time in the key population is randomly distributed and has a normal distribution. It is recognised that this assumption may often be violated as the distribution of time in a group is often heavily skewed toward lower durations, with many people entering the groups for a short period and then ceasing the corresponding risk behaviours. Because of that assumption we used primarily the median and in its absence the mean to calculate duration. The results for the third method are presented in a range formed by the mean and the median of the duration of the datasets.
If data were available, all three methods were applied for all the regions and key populations. The duration of high-risk behaviour has been derived for the following geographic regions: America, Europe, Asia, Australia/Oceania and Africa. When possible, the basic regions were unfolded to depict more specific information.
Results
Female sex workers
In all, 31 papers were found for Africa and they generated information about 47 different datasets.
-
Four papers described the percentage of FSW who started selling sex in the last year.4–7 Based on these studies the mean duration for FSW is estimated to be 5.5 years.
-
Using the third method proposed, 43 datasets provided the average duration of sex work.8–29 This period ranged from 0.3 to 6.0 years, with a mean and a median of 2.9 years which resulted in an average duration of 5.5 years.
A total of 40 papers were found on Asia which generated information from 48 different datasets.
-
Twelve papers described the percentage of FSW who started selling sex in the last year. Based on that information, the mean duration for FSW was 2.94 years and ranged from 1.35 to 12.05 years according to the dataset.30–40
-
Thirty-one datasets showed the average duration spent in sex work. This period ranged from zero to 6.5 years, with a mean of 2 years and a median of 1.4 years which would lead to a duration between 2.8 and 4.0 years.37 ,41–63
Nine papers were found on Europe and they generated information on 10 different datasets, showing the average duration of sex work. This period ranged from 1.5 to 12 years, with a mean of 5 years and a median of 4.2 years, which would lead to a duration between 8.4 and 10 years.64–72
Six papers were found for Latin America, describing the average time FSW spend in business. This period varied from 3.5 to 8.8 years according to the dataset, with a mean of 6 years and a median of 5.6 years, which would lead to a duration of risk behaviour between 11.2 and 12 years.73–79
Three papers were found in North America, showing the duration of sex work up to the interview in median years. The median ranged from 5 to 6.4 years with a mean of 5.5 years and a median of 5.1 years. If we consider this distribution to be normal and double the values to reach turnover, the estimated duration of risk behaviour is between 10.2 and 11 years.80–82
No papers were found for Oceania/Australia.
In summary, it was possible to generate estimates for duration of risk behaviour for five regions. The results are presented in table 1.
Regional estimates of duration of risk behaviour for FSW by the method of calculation
Male clients of female sex workers
Eight papers were found describing the median or mean duration during which men routinely bought sex: three in America83–85 (two in Mexico and one in Haiti), three for Asia/Oceania86–88 (China, India and Australia) and two for Africa89 ,90 (Benin and Kenya).
In America this period ranged from 6.3 to 10.8 years, with a mean of 8 years which leads to an estimated duration of risk behaviour of 16 years. For Asia/Oceania, the estimated duration ranged from 9.0 to 30 years, with a mean of 16.2 years which leads to a duration of 32.4 years.
One paper from Africa described the percentage of men who started paying for sex in the year prior to the survey (21.9%) suggesting a duration of 4.6 years.
Estimates on duration of risk behaviour are presented in table 2. However, given the low number of studies and wide variability, these findings must be interpreted with caution. More country-specific data are urgently needed for this population.
Regional estimates of duration of risk behaviour for MCFSW by the method of calculation
Injecting drugs users
In most of the world, more duration information was available for IDU compared with other key populations; however, there was substantial geographic variation in the number of studies conducted. Only two papers were found on IDU in Africa91 ,92 and one provided the percentage of IDU who started injecting drugs in the year prior to the survey: 18%.93 Based on that information, the turnover for IDU was estimated to be 5.6 years.
Overall, 16 papers were found on IDU in Asia and they generated information on 23 different datasets.
-
Six datasets described the percentage of IDU who started injecting drugs in the year prior to the survey.92 ,94 Based on that information, the mean turnover for IDU was estimated to be 8.7 years with a range from 3.7 to 22.2 years.
-
In all, 17 datasets showed the average time a person spent injecting drugs.95–107 This period ranged from 1.9 to 17.0 years, with a mean of 6.8 years and a median of 4.4 years suggesting turnover between 8.8 and 13.6 years.
A total of 12 papers were found in Oceania, all conducted in Australia, generating 15 different datasets.
-
A study conducted in Australia108 aimed to examine mortality within the 626 IDU from the Victorian Injecting Drug Users Cohort Study (VICS). They retrospectively examined mortality comparing data from the VICS, recruited from 1990 to 1995, to data from the National Death Index containing records of all deaths in Australia from 1990 to 2006. A total of 26 IDU died before the end of 2006 and the average length of injecting career at death was 17.0 years (SD=7.05, min 3.86, max 29.79); 18 of the 26 deaths were drug-related.
-
One paper109 described the percentage of IDU who started injecting drugs in the last year. Based on that information, the turnover for IDU was estimated to be 5.2.
-
Thirteen datasets showed the average time a person spent injecting drugs.110–119 This period ranged from 2.4 to 15 years, with a mean of 9.1 years and a median of 8 years suggesting a turnover between 16 and 18.2 years.
A total of 24 papers were found in Europe generating 37 different databases.
-
A study conducted in Scotland aimed to identify the mortality risk and explore the causes of death in all IDU who attended a family medical practice in northwest Edinburgh.120 They were followed for 21 years, and the mean time from first injection until death was 13.9 years.
-
Four datasets described the percentage of IDU who started injecting drugs in the year prior to the survey.121–123 Based on that information, the mean turnover for IDU was estimated to be 8.9 years.
-
Thirty-two datasets124–142 described the mean duration of injecting career up to the moment of the interview. It varied from 1.3 to 14.3 years, leading to a mean and a median of 8.6 years. If we consider this distribution to be normal and double the value to reach turnover, the estimated turnover would be 17.2 years.
Six papers were found on South America generating nine different datasets and they all described the duration of injecting career up to the moment of the interview by medians and means. This period ranged from 2.2 to 21 years, with a mean of 10.5 years and a median of 9.8 years suggesting turnover between 21 and 19.6 years.143–148
A total of 26 papers were found in North America generating 34 different datasets.
-
A prospective study conducted in the USA aimed to examine both the incidence of injection cessation and the change in injection frequency among those who did not quit injection.149 The study included 901 IDUs who were recruited from a Needle Exchange Program (NEP) or an area with no NEP in Chicago between 1997 and 2002. Cessation of injection, the main outcome variable, was defined as no injection drug use since the last interview (1 year prior). In all, 116 IDUs ceased injection during the study, and the median number of years from first injection until cessation was 9.5 years.
-
Five datasets described the percentage of IDU who started injecting drugs in the last year.150–153 Based on that information, the mean duration for IDU was 4.7 years.
-
33 datasets showed the average time a person spent injecting drugs.133 ,152–173 This period ranged from 1.3 to 23.9 years, with a median of 4.4 years and mean of 7 years, suggesting a duration between 8.8 and 14 years.
Duration estimates were generated for six regions. The results are presented in table 3.
Regional estimates of duration of risk behaviour for IDU by the method of calculation
High-risk MSM
MSM are also a key population because of the increased risk of HIV transmission through anal intercourse. However, anal intercourse can be safe when between faithful, uninfected partners or when consistent condom use is practiced. A literature review was completed of surveys of MSM looking for the turnover between high-risk MSM and low-risk MSM. However, no studies assessing turnover for this population were found. At this point it is not possible to estimate average duration in the high-risk MSM population. We decided then to compile the different definitions used in surveys for high- and low-risk MSM to contribute to the characterisation of these two different patterns of sexual behaviour among the MSM population. The MSM sexual practices are described below according to the risk of exposure to HIV.174–181
High-risk sexual behaviours
-
Barebacking
-
Unprotected anal intercourse (UAI) with an HIV-seropositive partner
-
Rimming (anal/oral sex play)
-
Fisting (insertion of the hand into the anus)
-
Use of sex toys and shared drug implements
-
UAI with casual partners
-
UAI with partners of an unknown or discordant HIV status
-
Having multiple sex partners
-
Trading sex
-
Having unprotected anal sex and anal sex while drunk or high in the past 6 months
Low-risk sexual behaviours
-
Men who had been involved in a mutually monogamous relationship for 2 or more years with a male partner known to be negative for HIV antibodies.
-
Men who had been involved in a mutually monogamous relationship for 2 or more years with a male partner under ART treatment.
Very few studies cover duration of risk behaviours for male sex workers and transvestites and therefore were not included in the study.
Discussion
This literature review provides estimates of the average duration people spend in high-risk behaviours categories by mode of exposure and geographical region. As described earlier, mathematical models of the HIV epidemic can use this information to estimate changes in the epidemic due to new susceptibles entering (ie, the population newly joining the high-risk populations) and older, higher prevalence members leaving. Spectrum/EPP, a model used by over 150 countries, requires this as an input for countries with concentrated HIV epidemics if the user wishes to apply turnover in their fits. This paper provides a more scientific basis for making turnover estimates using published and unpublished data that can be used by countries as inputs for the Spectrum/EPP model.
The results of the review showed that average duration of female sex work varies dramatically by region with the shortest durations (and highest turnover) found in Asia and the longest average duration of sex work found in the Americas.
Similarly, the average duration of injecting drug use varies by region. In Africa, average duration of injecting drug use was approximately 6 years while in South America and Oceania the duration was closer to 20 years. Large differences in turnover have important implications for prevention activities and services for key populations. In areas with very high turnover more frequent outreach activities and surveillance activities are required. Where turnover is slower, activities can focus more on reaching divergent subgroups of the key populations to ensure the entire population is reached with services.
The variability of these estimates at regional level suggests that there are substantial differences at national levels as well. Differences in duration might be due to different public health interventions by region, country or subnational level or due to different reasons for the high-risk behaviour such as financial need for sex work or poor future prospects for injecting drug use. Also, duration of injecting drug use is highly dependent on mortality, thus the differences in average injecting drug duration could be associated with differences in healthcare for the injecting drug population.
This study has several limitations. First, the definitions of key populations present minor variations among the different surveys analysed. Also, it is important to highlight that for the calculation of duration of risk behaviour for FSW, some studies that included FSW who practice injecting drug use were included. Similarly, studies on IDU who practice commercial sex work were included in the calculations of the average duration of time of injecting drugs. It was decided not to separate such information because the estimates of duration of risk behaviour calculated in this study are intended to serve as input for mathematical HIV/AIDS models. In such models, the stratification of an epidemic structure, in terms of populations, can be made as far as strategic information is available for each population. And rarely do countries have detailed information about HIV prevalence and population size for, for example, the sex workers who use injected drugs and the ones who do not.
Another point to be addressed is the differences found between the estimates generated by methods 2 and 3. These methods generated most of the time similar estimates of duration of risk behaviour, except for the population of IDU in Asia, Oceania and North America. In these regions, the estimates of duration calculated by method 2 are lower than the ones calculated by methods 1 and 3. One possible explanation is that the assumption of stability is being violated. In this case, method 2 may be underestimating duration. Given the limited number of studies allowing method 2 to be used, another likely explanation is that the specific populations of IDU being examined in the different papers have widely varying durations. In those few cases where data were available to apply both methods 2 and 3 the variation was not as extreme as the table averages would imply. And as (1) populations of IDU and FSW are likely to fluctuate due to economic changes, legal changes, changes in demand and changes in supply for the behaviour and (2) many samples are censored, the estimates of duration calculated by methods 2 and 3 among FSW and IDU should be compared which determine whether violations of the assumption of a steady state have a significant impact on the estimates.
Another limitation is that the estimates for MCFSW must be interpreted cautiously due to two reasons. First, to the low number of studies found. And second, because in many countries, young men may go through a period during which they frequent sex workers often, but then this behaviour ceases or slows once they marry. In countries where this is the most common male behavioural pattern, a better estimator of duration of high-risk behaviour for this population may be the difference between average age at first intercourse and average age at marriage.
Last, it is important to highlight that very few surveys collect data on duration of high-risk behaviour and thus the analysis was limited to the countries that have been collecting these data. Therefore, the geographical coverage in this review is limited to a few countries that have collected information on duration or time since initiation of risk behaviour.
Despite the many limitations to the calculations presented in this paper, these are, to the authors’ knowledge, the best available estimates of durations of risk behaviours. One important implication of this review is the need to include questions from which to estimate duration of risk behaviour in surveys among members of key populations in concentrated epidemics. These questions should be, for example: How long have you been exchanging sex for money? How long have you been injecting illegal drugs? How long have you been buying sex from FSW? From these questions, it is possible to demonstrate the proportion of members who have had the behaviour for less than 12 months and easily calculate duration of risk behaviour.
More research on turnover among key populations is needed to inform both models and prevention programmes. Future reviews on this subject should attempt to identify surveys in other databases such as Embase and Medline, rather than PubMed, and should also search for additional grey literature.
Key messages
-
This paper provides a more scientific basis for making turnover estimates using data that can be used by countries as inputs for the Spectrum/Estimation and Projection Package model.
-
There is high variability of estimates of duration of high-risk behaviours at regional level.
-
More research is needed to inform models and prevention programmes on the average duration of time individuals maintain a specific high-risk behaviour.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
Footnotes
-
Contributions EF: Conception and design of the study, acquisition of data, analysis and interpretation of data, article draft, paper review for important intellectual content, final approval of the version to be published. PC and MM: Conception and design of the study, analysis and interpretation of data, paper review for important intellectual content, final approval of the version to be published. TB: Interpretation of data, paper review for important intellectual content, final approval of the version to be published.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/