Article Text

Abstract
Background Considerable HIV transmission occurs among injection drug users (IDUs) in Pakistan and recently the HIV prevalence has been increasing among male (MSW), hijra (transgender; HSW) and female (FSW) sex workers. We describe past and estimate future patterns of HIV emergence among these populations in several cities in Pakistan.
Methods The density of these key populations per 1000 adult men was calculated using 2011 mapping data from Karachi, Lahore, Faisalabad, Larkana, Peshawar and Quetta, and surveillance data were used to assess bridging between these key populations. We used the UNAIDS Estimation and Projection Package model to estimate and project HIV epidemics among these key populations in Karachi, Lahore, Faisalabad and Larkana.
Results The density and bridging of key populations varied across cities. Lahore had the largest FSW population (11.5/1000 adult men) and the smallest IDU population (1.7/1000 adult men). Quetta had the most sexual and drug injection bridging between sex workers and IDUs (6.7%, 7.0% and 3.8% of FSW, MSW and HSW, respectively, reported injecting drugs). Model evidence suggests that by 2015 HIV prevalence is likely to reach 17–22% among MSWs/HSWs in Karachi, 44–49% among IDUs in Lahore and 46–66% among IDUs in Karachi. Projection suggests the prevalence may reach as high as 65–75% among IDUs in Faisalabad by 2025. HIV prevalence is also estimated to increase among FSWs, particularly in Karachi and Larkana.
Conclusions There is a need to closely monitor regional and subpopulation epidemic patterns and implement prevention programmes customised to local epidemics.
- HIV
- MODELING
- INJECTING DRUG USE
- SEXUAL NETWORKS
- COMMERCIAL SEX
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
HIV transmission in the context of injection drug use has been well-documented in many regions of the world.1–7 Pakistan lies within a large opiate-producing region and has a long history of drug use.8 Recent evidence suggests that Pakistan has large networks of injection drug users (IDUs).9 ,10 Cross-sectional survey results have indicated high rates of needle sharing in some cities11–13 and a highly variable HIV prevalence among IDUs across the country,12 ,13 as high as 52% in Faisalabad in 2011.13 Pakistan also has large populations of male (MSW), hijra (transgender; HSW) and female (FSW) sex workers,14 generally with low rates of consistent condom use.13 Hijras form a distinct sociocultural group unique to South Asia. Considered the third gender, most hijras are born as physiological men and dress in feminine attire, and some undergo castration. Many perform sex work, and clients are male.
Typically, Asian epidemics are ignited by HIV transmission among IDUs and expand into other populations through sexual networks, influenced by the size and characteristics of local key populations at greater risk for HIV infection.15–17
Pakistan's HIV epidemic is concentrated among IDUs (31% weighted prevalence in 2011),13 with a recent increase in prevalence among sex workers. The overall weighted HIV prevalence in 2011 was found to be 5.1% among HSWs, 1.6% among MSWs and 0.6% among FSWs.13 This is consistent with the patterns of other HIV epidemics in Asia18; however, Pakistan's HIV epidemics exhibit substantial geographical heterogeneity.13
In this paper, we describe the emergence of HIV in several cities in Pakistan, with an examination of differences in the size and characteristics of key populations. Specifically, we present the density of key populations in six cities and assess the sexual and drug injection bridging between these key populations. Modelling results which describe and estimate future patterns of emergence of HIV among these key populations in four cities are presented. This will provide a deeper understanding of Pakistan's heterogeneous HIV epidemics, providing valuable information to inform the design, implementation and scale up of effective HIV prevention interventions in Pakistan.
Methods
Study setting and data collection
The study setting, data collection, recruitment, and questionnaire development and interview technique have been described elsewhere.19–21 Briefly, four rounds of mapping and integrated behavioural and biological surveillance (IBBS) took place among IDUs and MSWs, HSWs and FSWs in several cities in Pakistan from November 2005 to December 2005 (Round 1), July 2006 to March 2007 (Round 2), March 2008 to June 2008 (Round 3) and March 2011 to September 2011 (Round 4). The study was restricted to MSWs age 13 years and older, HSWs and FSWs age 15 years and older, and IDUs age 18 years and older.
FSWs were not included in Round 3 data collection as the prevalence was extremely low in Round 2, but were included again in Round 4. Unlike in the first three rounds, MSWs and HSWs were surveyed separately in Round 4. For consistency, we combined the MSW and HSW Round 4 data into one group for the modelling analysis. MSWs and HSWs are similar in terms of their behaviour as both groups were born as biological men and have male clients; however, HSWs are transgender.
Capillary blood was collected for dried blood spot sampling and stored at room temperature. Samples were transported weekly to the reference laboratories for enzyme immunoassay screening (HIV Genetic Systems rLAV ELISA/enzyme immunoassay (EIA), Bio-Rad, USA) and positive tests were confirmed in duplicate with an alternative enzyme immunoassay (Vironostika HIV Uni-Form II EIA, Biomeriux, The Netherlands). Indeterminate results were resolved using Genetic Systems HIV-1 western blot (Bio-Rad, USA). All participants received an honorarium for their time and were referred for voluntary counselling and HIV testing and provided with HIV prevention and services information.
This study was approved by the institutional ethical review boards of HOPE International in Pakistan and the Public Health Agency of Canada.
Statistical analysis
Four rounds of data from Karachi, Lahore, Faisalabad and Peshawar and three rounds from Larkana and Quetta were included in the analysis of key population sizes and bridging between populations. Overall four rounds, 7118 IDUs, 6638 FSWs and 10 760 MSWs/HSWs were sampled from these six cities. Round 1 data collection did not take place in Larkana or among IDUs in Karachi, and Quetta was not included in Round 3.
Using Round 4 mapping data, the population density of each key population and city was calculated per 1000 adult men. Using Round 4 IBBS data, bridging of sexual and drug injection networks was assessed by calculating the proportion of sex workers who had sex with IDUs, the proportion of IDUs who paid for sex and the proportion of sex workers who had injected drugs in the past 6 months. We determined HIV prevalence and CI in each round, city and key population. HIV prevalence was calculated as the number of HIV-infected people divided by the total number of people surveyed in each of the respective years, cities and key populations.
Mathematical modelling
Data from Karachi, Lahore, Faisalabad and Larkana were included in the modelling analysis. As there were no data from Larkana in the first round, only three rounds of data were used for this city. The total sample size from these four cities was 5459 IDUs, 4331 FSWs and 7317 MSWs/HSWs.
All mathematical modelling was conducted using the UNAIDS Estimation and Projection Package (EPP). This compartmental model in which people move from susceptible to HIV infected compartments, has been described previously.22–24 The goal of the EPP model is to estimate and project HIV epidemics.
Within each key population group and city, we fit the model to empirically estimated HIV prevalence. To fit, we provided the following input parameters: empirically estimated HIV prevalence from 2 years to 4 years of survey data depending on the key population and city, population size of the respective cities in 2011, birth rates and background (non-HIV related) mortality rates, the estimated population sizes of the key populations in 2011, the mean number of years (duration) that people remain in respective key populations, and the estimated population sizes of the clients of FSWs and MSWs/HSWs. The population size of respective cities was obtained from the Pakistan Statistics Division25 and was extended to 2011 using a population growth rate supplied by the United Nations.26 The population sizes of key populations were estimated from mapping exercises conducted by our study group.19 The population sizes of clients were estimated from a combination of the estimated population of FSWs or MSWs/HSWs and the response to the survey question asking the number of clients that each respondent had sex with in the past month.
EPP varies four parameters in order to fit to the empirically estimated HIV prevalence. These four parameters are the start year of the epidemic, the rate of growth of the epidemic, the proportion of the population who are at risk at the start of the epidemic, and the recruitment rate or the rate at which at-risk people who die due to AIDS or otherwise leave are replaced by new at-risk people.
The goodness-of-fit procedure used by the mathematical model fits to the empirical point estimates of HIV prevalence. However, there is uncertainty in the underlying prevalence in each key population, which is why we estimate 95% CIs, in addition to point estimates. Due, in part, to the uncertainty in the value of the true prevalence for the years in which we empirically estimated prevalence, mathematical model projections are also uncertain.
We therefore examined a range of plausible HIV epidemic trends as follows. We used the year-specific point estimates of empirical prevalence to fit the model, and for this we initially ran the EPP model with many (3000) Latin Hypercube Sample intervals as recommended by UNAIDS. However, we also fit to each scenario—each city and key population—30 times, using sample intervals of 100. Using 100 intervals produced more variance in the estimated HIV epidemic and thus produced a range of possible HIV epidemics. With the exception of fitting to Faisalabad, we considered any model estimated epidemic to be plausible if it fit through at least two of the 95% CIs of empirically estimated prevalence for the respective city and key population. Using this method, we only discarded two model runs as ‘implausible’—both of the discarded runs were among IDUs in Larkana. Faisalabad was an exception. As presented in our results, the first three empirical prevalence estimates among IDUs in Faisalabad were near 15%, and the fourth estimate was >50%. As no model estimated prevalence fit through more than one 95% CI of empirically estimated prevalence among IDUs in Faisalabad, we present the results of all model runs for this city, even those that did not meet the criteria used for fitting with the other three cities.
Using mathematical modelling to project many years into the future is always risky because of uncertainty. Using the EPP model, it is particularly risky because one cannot allow EPP to change its four varying input parameters over time. In practice, risk behaviour may change over time, which could be reflected by changing one or more of the EPP parameters if this were possible. For this reason, our main results provide HIV prevalence estimates up to 2015. Nonetheless, while relying on estimated projections more than 3 years or 4 years into the future should be done with caution, we extended the model to project through 2025 in order to roughly estimate when we might expect to experience peak prevalence in the three key populations and four cities.
Results
Density of key populations
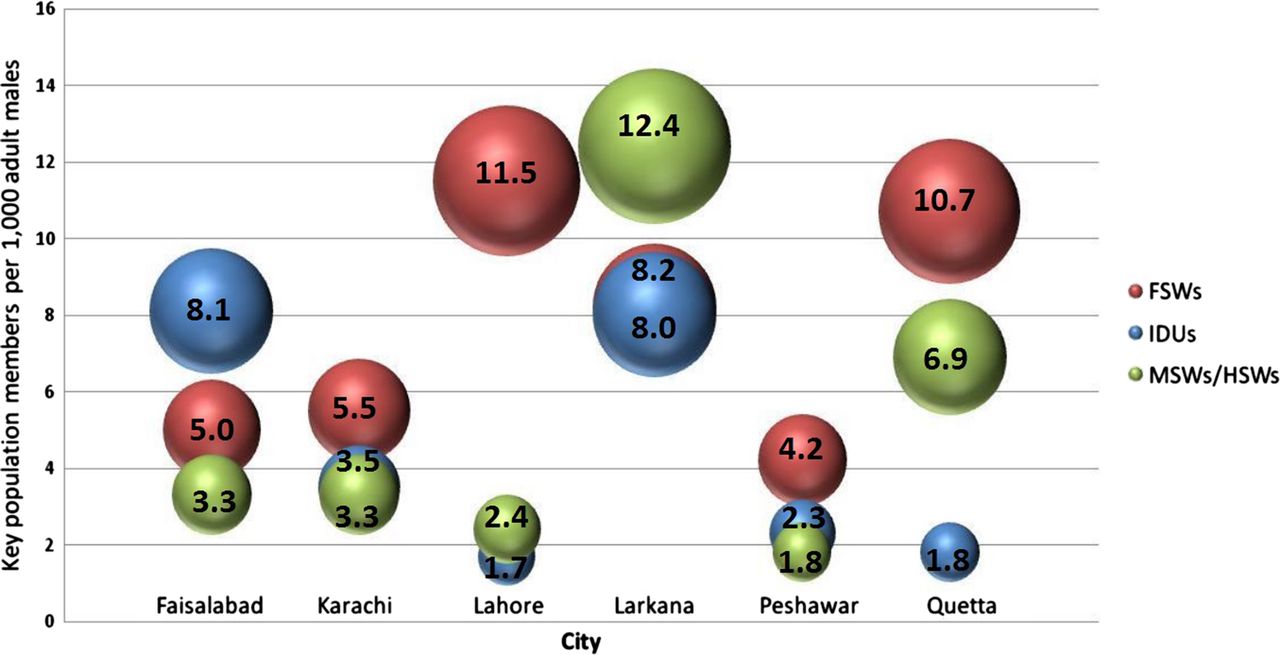
The density of each population group per 1000 adult men varies considerably across cities (figure 1). The MSW/HSW population density is smallest in Peshawar and largest in Larkana (1.8 and 12.4 per 1000 adult men). The FSW population density is smallest in Peshawar and largest in Lahore (4.2 and 11.5 per 1000 adult men). Lahore has the smallest IDU population density and Faisalabad the largest (1.7 and 8.1 per 1000 adult men). Karachi is a very large city and has the largest population size of all groups, particularly FSWs (estimated 25 399 individuals) and IDUs (estimated 16 544 individuals) (figure 2).

Injection drug user (IDU), female sex workers (FSWs) and combined male sex workers (MSWs)/hijra (transgender) sex workers (HSWs) population per 1000 adult men in six cities in Pakistan in 2011.

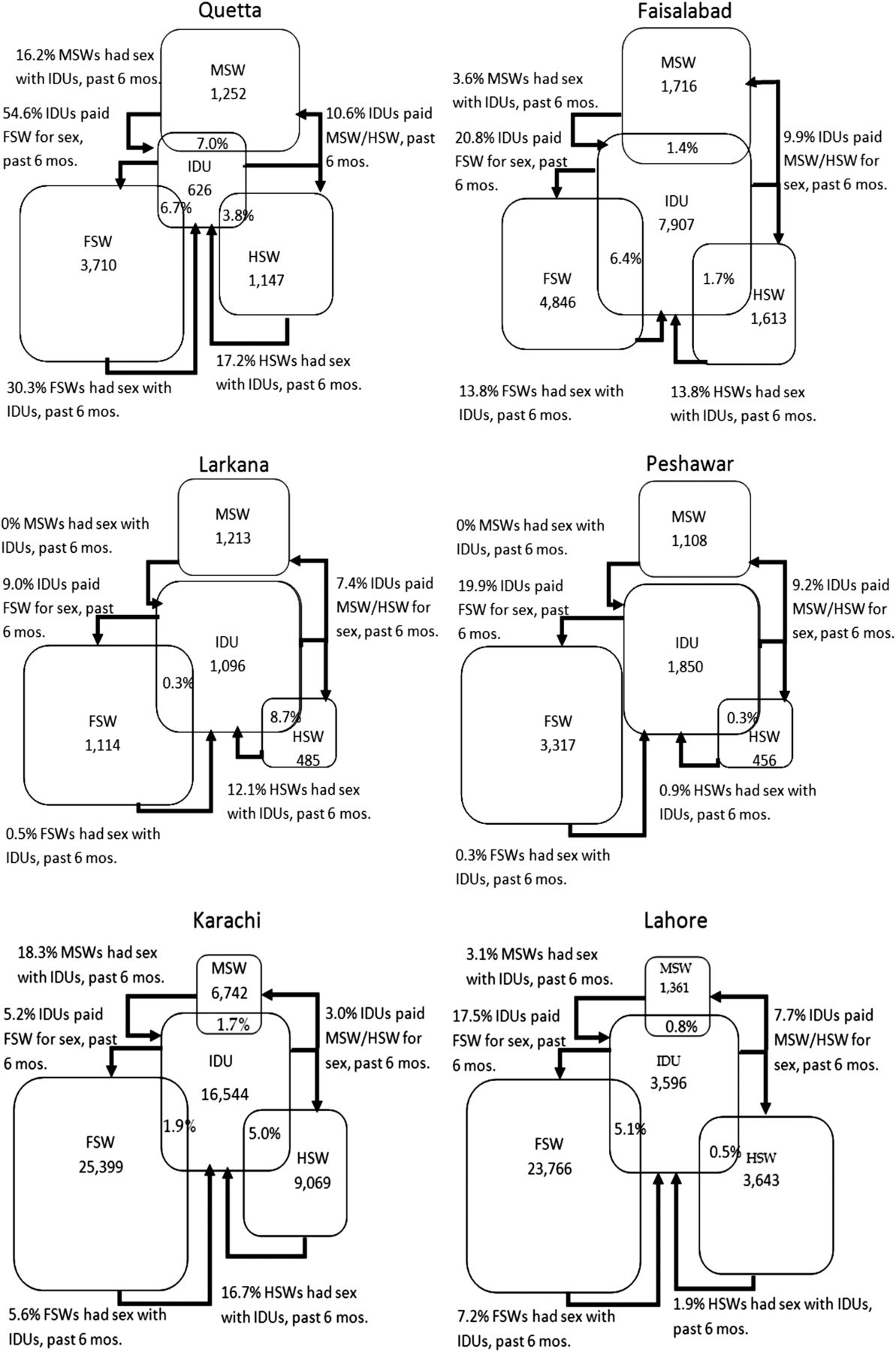
Bridging of injection drug use and sexual networks in 6 cities in Pakistan in 2011.
Bridging between key populations
The bridge population comprises individuals who engage in behaviours that create potential HIV transmission routes between different key populations (figure 2). The smallest proportion of MSWs, HSWs and FSWs reported injecting drugs in Peshawar (0%, 0.3% and 0%), and the largest proportion reported injecting drugs in Quetta (7.0%, 3.8% and 6.7%). Larkana was distinctive as many (8.7%) HSWs reported injecting drugs, but few FSWs (0.3%) and no MSWs did. Many (12.1%) HSWs in Larkana also reported sex with IDUs. Karachi also had relatively large sexual and drug injection bridging between HSWs and IDUs. Quetta had the largest percent of IDUs reporting paying for sex with MSWs/HSWs (10.6%) and FSWs (54.6%) while in Karachi very few IDUs reported paying for sex. In Quetta, a relatively large percentage of MSWs, HSWs and FSWs reported having sex with IDUs (16.2%, 17.2% and 30.3%), while very few in Peshawar reported having sex with IDUs (0%, 0.9% and 0.3%, respectively). Also, Faisalabad and Lahore had much sexual and drug injection bridging between FSWs and IDUs and Faisalabad had much sexual bridging between HSWs and IDUs. Generally, Peshawar had the smallest bridging of key populations and Quetta had the most bridging between sex workers and IDUs, sexual and drug injection.
Empirically estimated prevalence
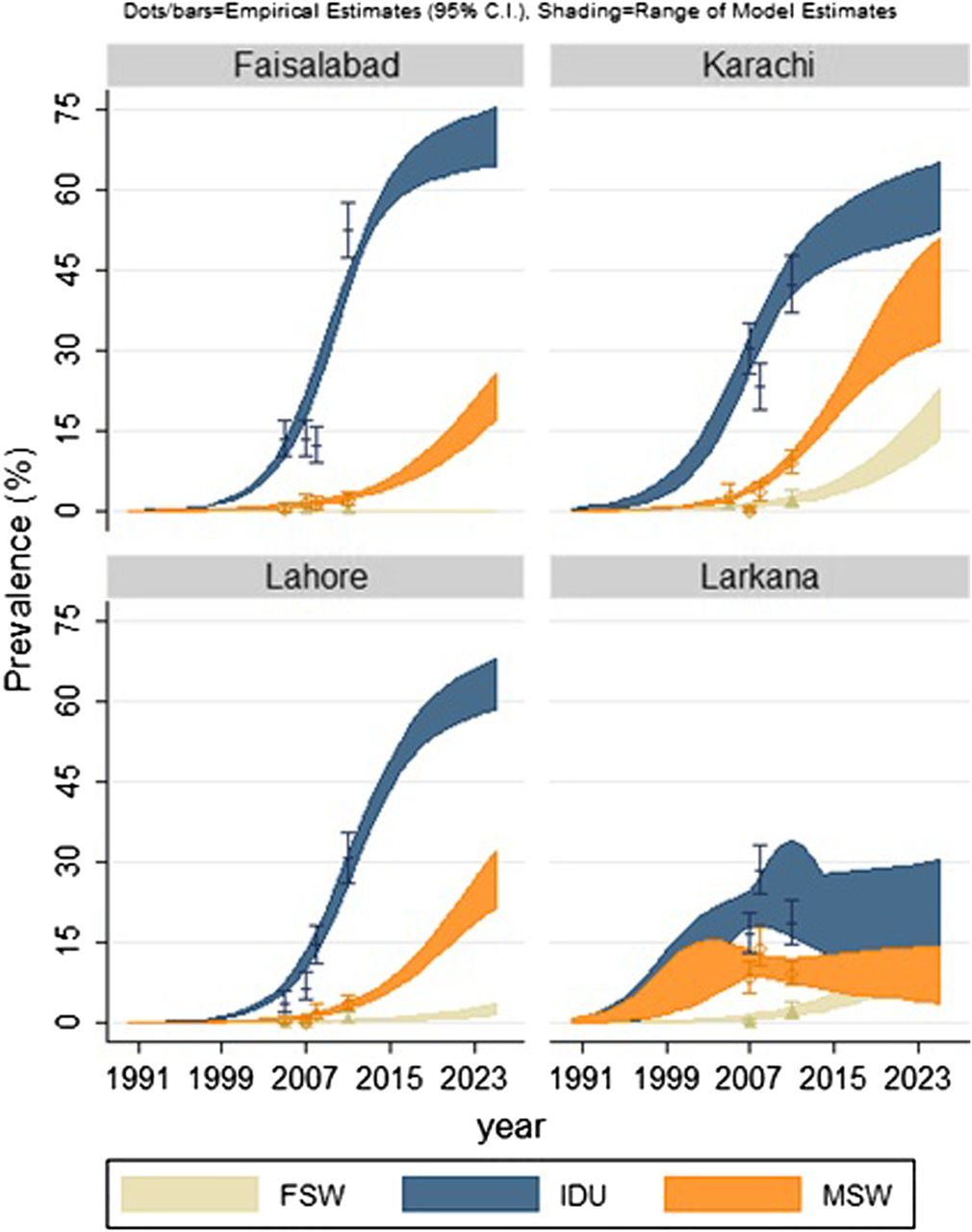
Empirically estimated HIV prevalence trends from the four survey rounds varied by city and key population (figure 3). In general, FSWs had the lowest prevalence among the three key populations, rising to just under 2% by 2011, while IDUs had the highest prevalence, with estimates in some cities and years as high as 30–40% and reaching 42.2% in Karachi and 52.5% in Faisalabad in 2011. HIV prevalence among MSWs/HSWs was higher than among FSWs, but lower than among IDUs. As with other key populations, the prevalence among MSWs/HSWs increased over time in most cities, with a maximum prevalence of 14.0% in Larkana in 2008. An exception to the rising trend in prevalence among MSWs/HSWs occurred in 2011 in Larkana, where the estimated prevalence fell from 14.0% (2008) to 9.8% (2011).

{kind=link}
{kind=link}
{kind=link}
Estimated HIV prevalence among female sex workers (FSWs), injection drug user (IDUs) and hijra (transgender) sex workers (HSWs)/ male sex workers (MSWs) in four cities in Pakistan.
HIV prevalence also varied by city, with the lowest prevalence among all three key populations in Lahore and, other than IDUs in 2011, Faisalabad. From 2005 to 2011, the trend in prevalence was only clear in Lahore, where prevalence increased across all three key populations. In Karachi, HIV prevalence may be expanding, after having declined during the mid-2000s. By contrast, among IDUs and MSWs/HSWs in Larkana, it appears that the epidemic may be declining after having peaked around 2008.
Model estimated prevalence
In Karachi, Lahore and Faisalabad, the range of model estimated prevalence produced similar epidemic pictures. In each of these three cities, the 30 plausible epidemic trajectories that were found by fitting to empirical data had no overlap between the prevalence trends of IDUs, MSWs/HSWs and FSWs, respectively (figure 3). Our model estimates give evidence that prevalence among IDUs is likely to peak very high. By 2015, it may already rise to as high as 55–60% in Karachi and Lahore, and 65–70% in Faisalabad. The 30 model estimates among IDUs range from 46.2% to 55.9% in 2015 in Karachi, from 40.9% to 49.1% in 2015 in Lahore, and from 58.8% to 62.5% in Faisalabad. While empirically estimated HIV prevalence among IDUs in 2007 and 2008 was lower in Faisalabad than in Karachi, the estimated prevalence in 2011 was higher in Faisalabad. However, none of the 30 model estimated epidemics in Faisalabad were able to completely replicate this (figure 3). The model estimated prevalence among IDUs in 2011 in Faisalabad ranged from 40.5% to 44.5%, which was significantly lower than the empirical estimate of 52.5% and more in line with the Karachi estimates in that year. With the caveat described previously that projections too far into the future should be interpreted cautiously, it appears that without intervention or behaviour change, prevalence among IDUs will continue to rise beyond 2015 in Faisalabad, Karachi and Lahore (figure 3), while the outlook in Larkana is less clear and will be described separately later in this paper.
We also examined model estimated prevalence among FSWs and MSWs/HSWs. In Karachi, the estimated prevalence by 2015 ranged from 17.0% to 22.1% among MSWs/HSWs, and 2.9% to 5.6% among FSWs. In Lahore, the model suggests the 2015 prevalence to be in the range of 5.9% to 8.3% among MSWs/HSWs, and 0.4% to 1.0% among FSWs. In Faisalabad, the 2015 estimates ranged from 4.4% to 6.3% among MSWs/HSWs, and were consistently 0% among FSWs.
Despite fairly consistently estimated epidemics across all 30 model estimates in Karachi, Lahore and Faisalabad through 2025, extending estimates this far into the future is uncertain. Even projecting through 2025, however, indicates that HIV prevalence in all cities but Larkana is unlikely to peak soon. The model evidence suggests that HIV prevalence among MSWs/HSWs may be nearing a peak in Karachi by 2025, but will still be expanding among MSWs/HSWs in the three cities of Karachi, Faisalabad and Lahore, and among FSWs in Karachi and Lahore. Model estimated prevalence among FSWs in Faisalabad was 0% from 2005 to 2011, mirroring the empirically estimated prevalence among FSWs in this city.
In Larkana, the model estimates of prevalence among FSWs was consistent, with all 30 plausible model estimates suggesting that prevalence will continue to rise through 2015 and onto 2025. The range of model estimated prevalence among FSWs in Larkana in 2015 was 2.6–5.4%. When extended to 2025, there was more uncertainty, and the range widened to 11.9–20.3%.
Model estimated prevalence for IDUs and MSWs/HSWs in Larkana was considerably less consistent (figure 3). This is due to the model fitting to empirical prevalence estimates which, in these two key populations, rose considerably from 2007 to 2008, and were lower in 2011. The EPP mathematical model was unable to simultaneously fit within the 95% CI of the 3 years of empirical prevalence data for these two key populations. Among IDUs, approximately half of the 30 model estimates suggest that the HIV prevalence will continue to rise through 2015, while approximately half suggest a peak happened in the mid-2000s, followed by a decline. If the prevalence continues to rise, the expected prevalence among IDUs in 2025 will range from 26.8% to 30.6%. However, if the prevalence is now declining, then the expected prevalence among IDUs in 2025 will range from 6.2% to 19.8%. The maximum among these estimates occurred between 2008 and 2011, and ranged from 18.1% to 34.2%.
Similar to IDUs, the model estimated prevalence trends for MSWs/HSWs in Larkana show two distinct and divergent patterns. About half of the estimates suggest that the prevalence among MSWs/HSWs may reach its highest point by 2020 and then approximately stabilise. The other half of the estimates suggest that the prevalence in this key population peaked in the early 2000s, and is currently declining. If the prevalence rises until 2020, then the expected prevalence among MSWs/HSWs by 2020 ranges from 11.7% to 13.7%, and by 2025, the expected prevalence is very similar with a range from 12.5% to 14.4%. However, if prevalence is now declining, then the expected prevalence among this key population by 2025 ranges from 3.6% to 6.4%. The highest estimates occurred between 2003 and 2007, and ranged from 8.7% to 15.5%.
Discussion
The results, from modelling estimates and analyses of ‘bridge’ populations due to injecting and sexual networks, presented in this paper indicate the overall potential for an HIV epidemic expansion beyond the IDU population to other key populations in Pakistan. Specifically, considering the rising HIV prevalence among IDUs, low condom usage, risky injecting practises27 ,28 and large population densities of FSWs and MSWs/HSWs in certain cities, there is the risk of spillover from the IDU populations into networks of sex workers and their clients. This inference is consistent with HIV transmission trends in other regions, particularly eastern Europe, the Russian Federation and central Asia, where transmission began among IDUs and subsequently moved into sex worker populations and onward to the general population.29 ,30 As a result, there is an urgent need to develop and scale up HIV prevention programmes designed specifically for IDUs, the intersection between IDUs and sex workers in Pakistan, and within sex worker networks. Furthermore, given the variable degrees of bridging between key populations of IDUs and sex workers, any intervention also needs to be tailored to the population composition and behavioural dynamics in particular cities.
Karachi is a large city with the largest key population sizes, particularly IDUs and FSWs, and had a high HIV prevalence among IDUs in 2011 (42.2%) and a high projected prevalence in 2015 (ranging from 46.2% to 55.9%) among IDUs. There was also much sexual and drug injection bridging between HSWs and IDUs in Karachi and the 2015 projected prevalence among MSWs/HSWs was high (ranging from 17.0% to 22.1%). This evidence may warrant implementing HIV prevention programmes targeting all key populations and particularly targeting risky sexual and drug injection behaviours linking HSWs and IDUs.
Lahore has a large population density of FSWs, with sex and drug injection linking FSW and IDU populations. The 2015 projected HIV prevalence is high among IDUs in Lahore (ranging from 43.7% to 49.1%). HIV prevention programmes in Lahore may therefore benefit from targeting risky sexual and drug injection behaviours between these two populations.
In Larkana, IDUs and HSWs are linked through sex and drug injection which may warrant HIV prevention programmes in this city targeting this link. Furthermore, as HIV prevalence among FSWs in the model estimates rises significantly higher in Larkana than in Lahore and Faisalabad, and to approximately the same level as in Karachi, more aggressive interventions may be required to contain the epidemic among FSWs, than among IDUs or MSWs/HSWs in this city.
Faisalabad has a high HIV prevalence among IDUs (52.5% in 2011) and the prevalence may increase to range approximately from 57.0% to 62.5% by 2015, assuming that current trends continue. Sexual behaviours link IDUs to HSWs and sex and drug injection links IDUs to FSWs in Faisalabad. As a result, it would be important to implement large-scale HIV prevention programmes in Faisalabad, particularly targeting IDUs, their sexual behaviours with HSWs and FSWs, and the drug injection behaviours of FSWs.
Quetta has the most significant bridging of all of the cities, with a large proportion of all sex workers reporting sex with IDUs and drug injection. HIV prevention programmes in Quetta should therefore target risky sexual and drug injection behaviours among all key populations.
Peshawar is a more conservative city, with relatively low key population sizes and low reported bridging. Key populations may be more difficult to reach by programmes (and surveillance), and therefore programmes designed for these populations may benefit from venue-based and network-based outreach.
Characterising cities in terms of their key population composition and HIV transmission dynamics is useful for the design of HIV prevention programmes. Prevention among key populations remains a key challenge for Pakistan's efforts to curtail the HIV epidemic. Without intervention or behaviour change, the HIV prevalence is expected to continue to rise among key populations in cities across Pakistan over the next 10–15 years. However, intensive efforts are required to bring about these changes. Modelling work to explore the potential impact of various interventions across the cities may help to inform policy makers about the most cost-effective options. Understanding the extent and pattern of interactions between the different key populations in the cities and the coverage of prevention programmes targeting these groups is also vital to contain or reverse epidemic trends.
Limitations
The UNAIDS EPP model is designed to estimate and project HIV epidemics, but is not designed to evaluate potential interventions. As such, the model does not incorporate changes in behaviour over time or turnover of members of key populations. We therefore estimated the HIV epidemic under the assumption of unchanging behaviour. Model results were not able to replicate the high empirical prevalence estimates among IDUs and MSWs/HSWs in Larkana in 2008, or the high empirical prevalence estimates among IDUs in Faisalabad in 2011. It is possible that these estimates were simply spuriously high. However, it is also possible that behaviour change accounts for the varying prevalence estimates. For example, if something occurred in Faisalabad between 2008 to 2011 which made it more difficult for IDUs to obtain clean syringes, this change could result in a very rapid increase in HIV prevalence among this group. We were unable to test this possibility using the EPP mathematical model.
Because antiretroviral therapy (ART) use in Pakistan is extremely low,31 we did not consider the distribution of ART in the model. The IBBS did not include questions about ART use initiation and distribution among HIV-infected individuals in each subpopulation.
The model estimated prevalence among FSWs in Faisalabad was 0% through 2025. This is likely an underestimate, but was based on the fact that no FSW participants from Faisalabad were infected. As there is evidence of population bridging in Faisalabad, the true prevalence is probably greater than 0%, but would require a larger sample size to detect. If the model were being fit to low but positive prevalence among FSWs, then the projections through 2025 would likely have showed an increasing trend.
Although our main results present findings of model-estimated HIV prevalence through 2015, we wanted to assess when we might see a peak in prevalence. For this reason, we also projected HIV prevalence to 2025. Projecting as far as 2025 comes with much uncertainty, primarily because changes in behaviours and public health policies impacting HIV incidence are likely to occur over time. Estimates through 2025 should therefore be interpreted cautiously and with the caveat that these estimates assume that behaviour, population growth and migration remain unchanged.
Key messages
-
Cities across Pakistan have variable degrees of bridging between key populations of injection drug users and sex workers, representing potential HIV transmission routes.
-
Model estimates suggest that the HIV prevalence may reach 17–22% among male and hijra (transgender) sex workers in Karachi and 46–56% among injection drug users in Faisalabad by 2015.
-
Model estimates suggest that the HIV prevalence may increase among female sex workers, particularly in Karachi and Larkana.
-
There is a need to closely monitor regional and subpopulation epidemic patterns and implement prevention programmes customised to local epidemics.
Acknowledgments
We thank the HASP surveillance team for their efforts in mapping, data collection, specimen collection, data entry and knowledge translation. We also thank the participants who took part in the surveys.
References
Footnotes
-
Contributors TR was involved with the design of the study and interpretation of results and critically reviewed the manuscript. DYM performed the data analysis and co-wrote the manuscript. LAS co-wrote the manuscript, led the analysis, critically reviewed the manuscript, and revised later drafts. MS was involved in the design of the study and critically reviewed the manuscript. AA was involved in the design of the study and critically reviewed the manuscript. AS was involved in the design of the study and critically reviewed the manuscript. GCJ critically reviewed and revised the manuscript. FE was involved with the design of the study and interpretation of results and critically reviewed the manuscript. LHT co-wrote the manuscript, critically reviewed the manuscript, and revised later drafts. JFB was involved with the design of the study and interpretation of results and critically reviewed the manuscript. He led the development of the special supplement strategy.
-
Funding The Canada-Pakistan HIV/AIDS Surveillance Projected was funded by the Canadian International Development Agency (contract number CIDA PK 30849).
-
Competing interests None.
-
Ethics approval HOPE International; Public Health Agency of Canada.
-
Provenance and peer review Commissioned; externally peer reviewed.