Article Text

Abstract
Objective To determine if a structured complex intervention increases opportunistic chlamydia screening testing of patients aged 15–24 years attending English general practitioner (GP) practices.
Methods A prospective, Cluster Randomised Controlled Trial with a modified Zelen design involving 160 practices in South West England in 2010. The intervention was based on the Theory of Planned Behaviour (TPB). It comprised of practice-based education with up to two additional contacts to increase the importance of screening to GP staff and their confidence to offer tests through skill development (including videos). Practical resources (targets, posters, invitation cards, computer reminders, newsletters including feedback) aimed to actively influence social cognitions of staff, increasing their testing intention.
Results Data from 76 intervention and 81 control practices were analysed. In intervention practices, chlamydia screening test rates were 2.43/100 15–24-year-olds registered preintervention, 4.34 during intervention and 3.46 postintervention; controls testing rates were 2.61/100 registered patients prior intervention, 3.0 during intervention and 2.82 postintervention. During the intervention period, testing in intervention practices was 1.76 times as great (CI 1.24 to 2.48) as controls; this persisted for 9 months postintervention (1.57 times as great, CI 1.27 to 2.30). Chlamydia infections detected increased in intervention practices from 2.1/1000 registered 15–24-year-olds prior intervention to 2.5 during the intervention compared with 2.0 and 2.3/1000 in controls (Estimated Rate Ratio intervention versus controls 1.4 (CI 1.01 to 1.93).
Conclusions This complex intervention doubled chlamydia screening tests in fully engaged practices. The modified Zelen design gave realistic measures of practice full engagement (63%) and efficacy of this educational intervention in general practice; it should be used more often.
Trial registration The trial was registered on the UK Clinical Research Network Study Portfolio database. UKCRN number 9722.
- GENERAL PRACTICE
- EDUCATION
- CHLAMYDIA INFECTION
- BEHAVIOURAL INTERVENTIONS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis is one of the most common sexually transmitted infections in Europe,1 and systematic chlamydia testing is offered in at least eight EU countries in varied healthcare settings.1 In England, the National Chlamydia Screening Programme (NCSP) aims to identify and treat asymptomatic cases through opportunistic screening of 15–24-year-olds.1 General practices provide the first point of contact for the majority of healthcare in the community in England. They are a natural setting for detecting infections as over 60% of young people attend annually;2 the majority of contraception is prescribed in general practice,3 and in England, young people have stated a preference for being tested in their local general practitioner (GP) practice.4 Only 16% of NCSP tests come from general practices5 due to many different perceived barriers reported by staff including lack of time, knowledge, confidence discussing chlamydia or simply forgetfulness.6
Multifaceted interventions7 with clear targets and audit,8 ,9 and based on a cognitive theory10 such as the Theory of Planned Behaviour (TPB),11 ,12 are successful at changing behaviour. The aim of this study was to determine the effectiveness of a structured complex intervention13 based on the cognitive TPB11 to increase opportunistic chlamydia screening tests of patients aged 15–24 years registered in English general practice.
Methods
We used a prospective, cluster randomised controlled trial with a modified Zelen design.14–16 Random allocation is very difficult to conceal in evaluations of educational interventions, as intervention and control consenting clinicians will know they are part of a trial and may modify their behaviour. Practices may tend to participate in educational initiatives of particular interest to them; moreover, research practices may be atypical. Modified Zelen design overcomes this potential bias by not informing any participants that they are participating in a trial.
Sample sizes
(see Web only figure 1) To be able to detect at least a 10% absolute increase in screening test rates from 3% to 13%, and allowing for the estimated design effect, we needed to randomise 80 practices to intervention and 80 to control (see Web only annex 1).
Setting
We selected general practices registered with the NCSP between 2009 and 2011 from 11 Primary Care Trusts (PCTs) in the South West of England; this includes a population of 848 000, 15–24-year-olds.
Intervention
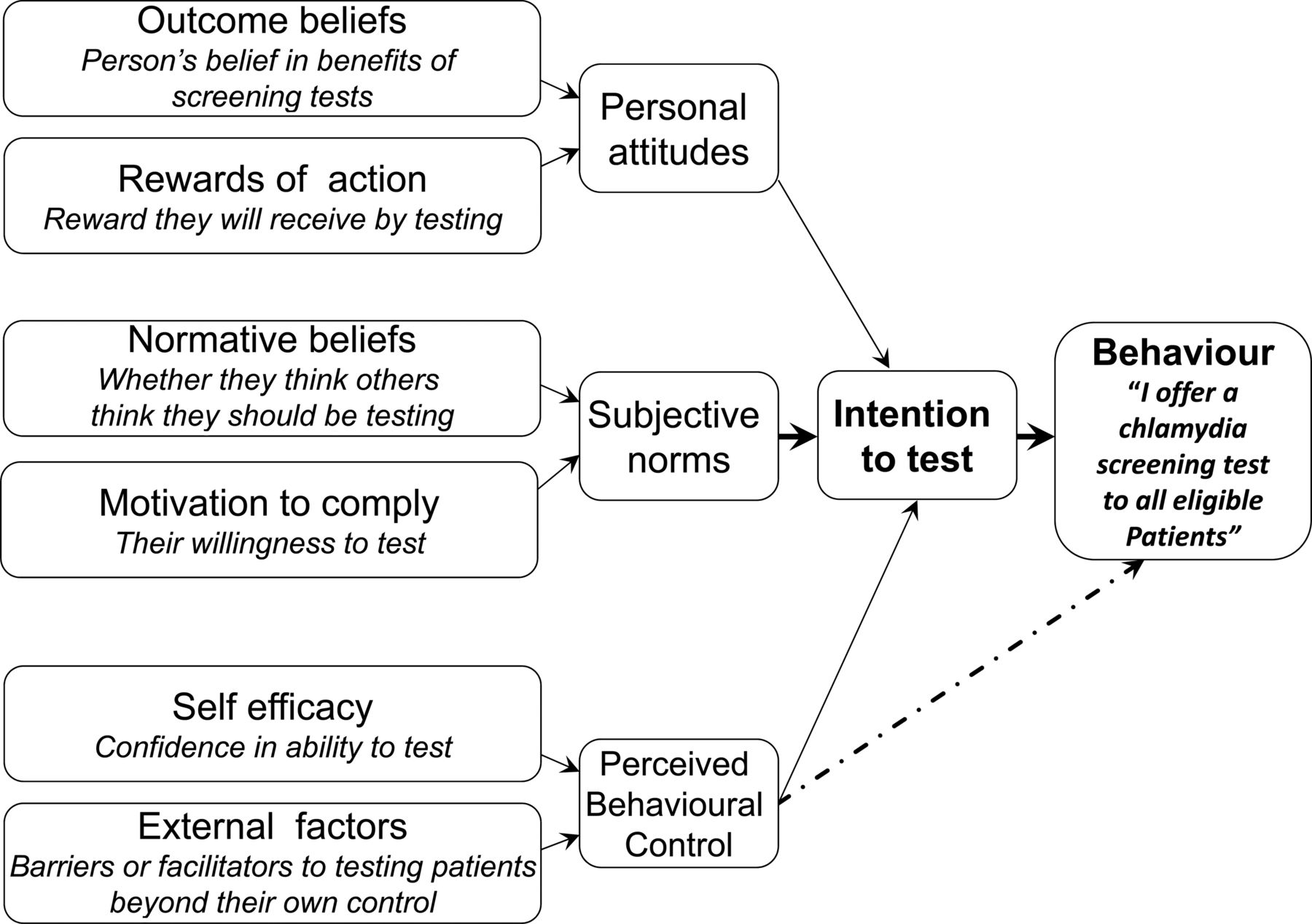
The complex intervention13 combining an outreach educational workshop7 with posters, invitation cards, targets and feedback of practice testing performance8 and ongoing support, was based on the TPB11 that proposes our intentions (in this case, intention to offer a chlamydia screening test) are derived from the combination of three key factors: personal attitude (whether a person is aware of benefits of testing),17 subjective norms (how much a person feels social pressure to test) and perceived behavioural control (whether the person feels able to offer a chlamydia test or if there are barriers beyond their own control) (figure 2) (see box 1).18 Between April and September 2010, all intervention practices were offered a practice workshop based on the TPB13 for all staff (box 1). The Health Protection Agency researcher (called chlamydia support worker to prevent unblinding of the study) gave a presentation that aimed to change personal attitudes to chlamydia testing, covering the epidemiology and benefits of diagnosing infections. The practices’ own data were used to develop realistic monthly test targets8 ,9 based on 15–24 year old practice attendance. Lack of confidence to offer screens was addressed through videos and through providing staff with a screening test ‘script’.13 To influence personal attitudes and subjective norms, practices were offered posters stating ‘WE are a chlamydia screening practice’ and patient invitation cards to raise awareness of testing in staff and patients, sent monthly newsletters including individual practice testing rates, and to influence behavioural controls, encouraged to use computer reminders. The support worker helped staff adapt the intervention to fit each practice, and identified a chlamydia champion to maintain the profile of chlamydia. During the next 9 months practices were offered two contacts to offer further support, feedback on testing rates and help implement materials. The practice staff could accept or refuse any part of the intervention.13
{kind=link}
The Theory of Planned Behaviour and clinician's intention to undertake chlamydia screening tests.
Intervention components addressing personal attitudes, subjective norms and behavioural controls
1) Changing personal attitudes:
Outcome beliefs, increasing belief in benefits of chlamydia screening tests:
-
Practice workshop demonstrating how common chlamydia is in 16–24-year-olds, and the benefits of testing a usually asymptomatic pool of infections to reduce sequelae and onward transmission.
-
Feedback through newsletters to all staff and to practice ‘champion’, of testing activity and positivity may influence attitude towards the value of testing by demonstrating successful testing over time. For example, when increases in uptake and positives are observed, practice staff may feel that it is worth offering a chlamydia test.
Rewards of action; increasing rewards they will receive by testing:
-
Develop testing targets based on a practice's 15–24-year-old population and consultations. Targets can act as a driver, so at the workshops explore the possibility of agreeing practice targets and milestones as a way of continually monitoring progress and keeping motivation high.
-
Feedback testing progress through monthly newsletters and at second practice visit/contact by chlamydia support worker.
-
Certificate of training attendance at practice workshop.
-
Certificate of personal development after doing on-line quiz.
2) Subjective norms
Normative beliefs (whether they think others believe they should be testing):
-
Invite all staff to a practice workshop (in protected learning time) to discuss how to offer a chlamydia test in all consultations, including best practice with under 16-year-olds. This should influence normative beliefs by affecting whether practice staff think offering testing is acceptable to patients, and whether they think others in the practice will value them making testing offers.
-
Practice posters indicating that ‘WE are a chlamydia screening practice’ to show that testing is routine in the practice making it more acceptable to both staff and patients.
-
Facilitate practice teamwork through inclusion of chlamydia testing as a standing agenda item at practice meetings. This may influence beliefs about whether others in the practice value the fact that ‘I am offering a chlamydia test to all my eligible patients’.
-
Personal regular newsletters to all the practice staff giving information about chlamydia testing and their latest testing figures. Make these figures available on the website, including anonymous figures for other practices, so they can see that their peers in other practices are testing too.
-
Identify a ‘champion’ for chlamydia testing who acts as a positive role model influencing whether practitioners believe that others value them offering chlamydia tests.
-
Add a pop up for the testing age group (15–24) to normalise the offer.
Motivation to comply; their willingness to test
-
At practice workshop give evidence that young people who attend general practices in UK or who have collected a testing pack do want to be tested in general practice.
-
Demonstrate how quickly and simply an offer of a test can be made, so the time to do so is not perceived as a barrier.
-
At practice workshop provide evidence that patients can take the sample and complete the form without difficulty.
-
At practice workshop give information about payment levels for testing where a Local Enhanced Service payment is in place.
3) Perceived behavioural control beliefs
Self-efficacy; confidence in ability to test
-
Practice workshop in protected learning time will improve staff knowledge and self-confidence to offer a test.
-
Demonstrate how to offer a test via film clips delivered as part of practice workshop and also available on the website will influence self-efficacy by demonstrating how easy it is to offer a test and give them a ‘script’ to use. The clips covered receptionists handing out small invitation cards to patients, and GPs offering testing to female and male patients, giving suitable ‘scripts,’ for example, ‘you may have seen the posters in the waiting room indicating WE are a chlamydia screening practice’.
-
Give practices discreet credit card sized testing invitations for receptionists or other practice staff to give to patients. This makes it easier for the receptionists to be involved; film clip demonstrating the offer will increase confidence in their ability to do so.
-
Add chlamydia test to templates for consultations with individuals 15–24 years of age, including contraception, asthma, travel and new patient checks. This will provide staff with ways to approach chlamydia testing thereby increasing confidence, particularly with male patients.
-
Web-based education based on the same presentation will allow those who cannot make the practice workshop to undertake the training and receive a certificate.
-
At practice workshop provide staff with a script to use so they know how to offer a test ‘WE are a chlamydia testing practice and you are in the testing age group—could you do a test today?’
External factors/control beliefs; barriers or facilitators to testing at a practice level
-
Templates help remind practice staff to discuss chlamydia testing with the target age group.
-
At practice workshop, present evidence that patients in the age group are happy to be offered a test; thereby overcoming a perceived behavioural control.
-
Remove the barrier about asking whether the patient is sexually active and instead offer a test to all patients based on their age.
-
List the tasks of the identified ‘champion,’ thus reducing barriers to the champion to increasing testing in the practice by increasing testing services such as availability of sex-related clinics, leaflets, etc that may promote test uptake.
-
Develop computer prompts to remind clinicians and/or receptionists to give out leaflets and/or packs to 15–24-year-old patients. If this approach is adopted, the chlamydia support worker will work with the practice to develop the computer prompts.
NCSP support during study period
At registration with the NCSP, practices received a screening information pack and area-specific training. Over the study period, control and intervention practices continued to receive usual support from their local NCSP chlamydia coordinator who had an overall target chlamydia screening testing rate for 16–24-year-olds in all NCSP venues across their area in 2009 of 25% and 2010 of 35%; coordinators did not know practice study allocation. Usual support involved a single telephone contact or visit, availability to answer any queries by telephone, provision of testing kits when they were needed and partner notification.
Data analysis
Aggregate data by month, age and gender for each registered GP practice on all chlamydia screening tests in the study area submitted on a NCSP form for the 3 years (2009–2011) (inclusive) were used to assess the absolute and relative change in testing/100 and infection detection rates/1000 registered 15–24-year-old patients, between the intervention, control and non-study practices during the 1 year period of the intervention, and in the 9 months after the intervention was formally withdrawn (see Web only annex 2).
Mixed effects Poisson regression models were used to provide estimates for both an ‘intention to treat’ analysis in which all randomised practices were included and a per-protocol analysis in which intervention practices were matched with the geographically closest practice of similar size. Numbers of screening tests or chlamydia infections detected were the outcome variables and the natural logarithm of the estimated numbers of 15–24-year-old patients registered at each practice included as an offset to normalise for variation in list size. The intervention was included as a categorical variable. In all regression models, GP practice is considered as a random effect, and sex, age, PCT, the practice areas deprivation score quintile, quarter within the year and preintervention chlamydia testing rate were considered as fixed effects.
Results
No practices withdrew from the NCSP; two controls and one intervention practice were excluded, as two study practices merged and one had prior knowledge of the study. Thus we analysed data from 76 of 77 intervention and 81 of 83 controls. Forty-seven practices (62%) agreed to three contacts with the chlamydia support worker, 16 (21%) agreed to one or two contacts and 13 practices (17%) refused all contacts. Staff attendance at the first presentation varied; in some all grades of staff attended a team meeting, in others only GPs or nurses attended. A total of 76 intervention and 76 control practices have been used in the per-protocol analysis.
As expected, prior to the intervention there were no important differences in deprivation, testing rates or chlamydia infections detected in control, intervention or non-study practices (table 1).
Baseline data table for GP practices (April 2009–March 2010)
Intention to treat (table 2): Absolute testing rates across all practices offered the intervention increased from 2.43 to 4.34/100 15–24-year-old patients registered with the practices during the intervention period compared with controls that increased from 2.61 to 3.00/100 patients; unadjusted rate ratio 1.66 (CI 1.1 to 2.5). The absolute increase in the screening rates (intervention compared with baseline period) in the intervention practices ranged from −9.6% to 28.8%, the lower, middle (median) and upper quartile being −0.2%, 2.0% and 3.3%, respectively. For the control practices, these are much lower than seen in the intervention practices, with the mean being zero; the range was −6.4% to 7.6%, the lower, middle (median) and upper quartile being 0.7%, 0% and 1.3%, respectively. Those intervention practices in the upper quartile of increased testing were significantly more likely to have used invitation cards, posters and prompts. After allowing for any imbalance in age, sex, PCT, month, deprivation quintile and prestudy chlamydia testing rates between each study arm, the chlamydia testing rate/100 15–24-year-olds in the intervention practices was 1.76 times as great (CI 1.24 to 2.48, p<0.001) as control practices in the intervention period. This relative difference persisted during the 9-month postintervention period (estimated rate ratio compared with controls 1.57 (95% CI 1.07 to 2.30, p=0.02; absolute testing rate intervention 3.46, controls 2.82/100 registered patients 15–24 years). There was no significant difference in the intervention effect between men and women.
Absolute numbers of chlamydia tests, testing rates and estimated testing rate ratio obtained from the mixed-effects Poisson regression model during and 9 months following the intervention period by study group
Per-protocol results (see Web only table S3) In the 47 practices that were fully engaged with the intervention, the testing rate increased by 2.33 times that seen in the control practices (RR 2.33, 95% CI 1.63 to 3.34, p<0.001; absolute rates intervention 5.55, controls 2.85, non-engaged 2.22/100 patients 15–24 years) and this remained 1.97 times as great in the postintervention period (RR 1.97, 95% CI 1.40 to 2.77 absolute rates fully engaged 4.20, non-engaged 1.32, controls 2.45/100 patients 15–24 years). In those 34 practices that used templates/computer reminders, the testing rate was 2.81 times as great as in control practices (RR 2.81, 95% CI 1.91 to 4.13, p<0.001, absolute rate if used prompts 6.52, did not use prompts 1.40/100 patients 15–24 years) and this remained two times as great in the postintervention period (RR 2.00, 95% CI 1.36 to 2.94; absolute rate if used prompts 4.11, did not use prompts 3.04/100 patients 15–24 years).
Number of chlamydia infections detected
The absolute numbers of Chlamydia infections detected in intervention practices increased from 2.1 prior to 2.5/1000 registered 15–24-year-olds during the intervention, compared with 2.0 and 2.3 in control practices; After allowing for the month of the first visit to the practice, and potential confounders including age, sex, PCT, month, deprivation quintile and baseline positive screen rates in each practice, the estimated rate ratio in the intervention practices was 1.4 (95% CI 1.01 to 1.93) times as great in the intervention practices compared with control practices (p=0.04). Positives detected remained for the 9 months after the intervention (absolute rates intervention 2.5, controls 1.68/1000 registered 15–24-year-olds; RR 1.6 (95% CI 1.09 to 2.3, p=0.02)).
In fully engaged intervention practices, the number of chlamydia infections detected was 1.8 times as great as controls during the intervention period (95% CI 1.2 to 2.5, p=0.005 absolute rates fully engaged intervention 3.2, controls 2.2, non-engaged intervention 1.0/1000 patients 15–24 years) and 1.6 times as great in the 9 months after (95% CI 1.1 to 2.4, p=0.03; absolute rates fully engaged intervention 2.7, controls 1.7, non-engaged intervention 1.7/1000 patients 15–24 years) than that seen in the control practices (see supplementary table S3).
Discussion
Main results
This complex intervention within the English chlamydia screening programme lead to a 76% increase in chlamydia screening test rates across all practices offered the intervention, with a 40% increase in infections detected. The absolute increase in testing across all intervention practices was small increasing from 2.43 to 4.34/100 15–24-year-old patients registered. However, these results include those practices that did not accept any visits (17%) from the chlamydia support worker or did not use all components of the intervention offered. The 62% of practices that agreed to three contacts with the support worker attained a 2.33 times relative increase in chlamydia testing.
Strengths
The greatest strength of our study was the modified Zelen design, which allowed us to deliver a ‘real life’ evaluation, in which all practices were invited to participate rather than research active practices or those enthusiastic about sexual health. The 62% uptake of three contacts and overall results are likely to be similar if the intervention was used in other areas with similar primary care resources. The modified Zelen design is particularly useful for the pragmatic evaluation of educational interventions 16 as participants can accept or decline components of the intervention as they would in routine practice because participants are unaware they are in a trial and so do not modify their behaviour on that account. The design was feasible as the primary outcome was measured using routinely generated NCSP data and consent for practices to take part was given on their behalf by PCT public and locally respected sexual health leads. After data collection was complete, all practices received a letter about the design and consent; no practices expressed any concerns.
A further strength was TPB-driven intervention design whereby components (see Web only annex 3) addressed personal attitudes, subjective norms and perceived behavioural controls. Further, our results demonstrate the importance of engaging general practices in all parts of such an intervention, as those practices that only partially engaged or did not use posters, invitation cards or computer prompts, had non-significant increases in testing. Those practices that agreed to three contacts with the support worker, demonstrating a positive personal attitude and practice attitude (subjective norm) to chlamydia testing, had a greater increase in screening. These three contacts also allowed the support worker to discuss testing rates against targets set at the initial workshop; targets influence both personal attitudes and subjective norms. Posters and invitation cards had a significant effect on testing rates and addressed all components of the TPB, normalising screening within the practice and increasing awareness, and acted as prompts for testing invitations for patients, which was demonstrated in the workshop videos. Behavioural controls, including lack of time and forgetfulness, were addressed with the computer prompts used by 45%.
Limitations
Because of the modified Zelen design we could not make practices use all the components of the TPB; however, our per-protocol analysis allowed us to explore the importance of individual components. Computer reminders were used by 45% of the intervention practices, and therefore, the intention-to-treat analysis for this component is probably valid; however, as all of the 62% fully engaged practices also used posters and testing invitation cards, it is not possible to determine the independent effect of these latter components. GP practices were not asked to deliver chlamydia results or undertake contact tracing. Although NCSP coordinators knew about the study, they were asked not to discuss it and did not know which practices were randomised but awareness may have motivated them to increase their practice support.
How our work fits in
A systematic review has shown that a multifaceted workshop approach addressing barriers to screening is more effective than single-component interventions.19 Several studies have demonstrated that the long-term support is pivotal to increase testing by maintaining the importance of chlamydia testing (addressing personal attitudes) and for it to become normal practice (a subjective norm). This approach was successfully used both in an American adolescent clinic20 in which clinicians participated in a four-stage clinical improvement initiative with monthly visits and in two London PCTs where workshops were given with long-term support.21 In contrast, a single outreach interactive workshop with several practices together16 led to a lower increase in testing rates.16 Changing the subjective norms at the practice and area level are both important. Our initiative involved single practices across a wide area, and so, they had little influence from peers outside their practice, but the London intervention involved all practices in just two PCTs and gave testing feedback; 21 this localisation of the intervention may have had greater influence on subjective norms and motivated practices to increase tests.21 The London intervention continued support for 3 years (compared with only 1 year in our study) allowing a longer period for testing behaviour change.
Another reason for the greater absolute increase in testing rates in the London study may have been the financial incentives offered.21 Systematic reviews show that financial incentives for providing a prespecified level of healthcare activity are generally effective.22 Financial incentives used to encourage chlamydia testing will strongly influence personal attitude and practice subjective norms, but have been shown to be ineffective in isolation23 or to have a short-term effect24 as they are unlikely to influence long-term attitudes about the importance of testing unless combined with other interventions, as in Kalwij's initiative.21 We also saw a temporary increase in testing prior to April 2009, 2010 and 2011 (see Web only figure 3), as practices sought to reach local targets.
Our intervention included a website containing all the presentations, materials and testing rates already provided in direct practice feedback. However, few GP staff in our study reported using it, indicating this was not a key part of the intervention. The need for direct contact with practices is reinforced by the lack of effectiveness of an internet-based intervention based on cognitive theory.25
GP staff considered that giving them the skills and confidence to offer chlamydia tests (overcoming one of the perceived behavioural controls) was an important part of the intervention; this was attained through video clips showing clinicians how to offer chlamydia testing in different consultations. This approach cannot be used in isolation as shown in a Belgian GP study, in which a package using commented video footage on communication skills increased appropriate testing but had no effect on overall testing rates.26
A Cochrane review found that computer reminders achieved a median improvement in targeted behaviour of 4.2%,27 but as the range of change was wide, they suggested further research to identify other factors consistently associated with larger improvements.27 Integration of computer alerts to remind Australian clinicians to screen increased chlamydia testing by 30%.28 Practices that incorporated computer prompts within our intervention had the greatest increase in testing rates and this was maintained beyond the end of the intervention. We consider this is a very cost-effective way of increasing testing but should not be used in isolation as GP staff may ignore alerts unless education also increases their belief in testing.
Implications of this research nationally and for commissioners
Our study and the London service evaluation demonstrate that a workshop approach with materials and long-term support will work and is feasible. Although the absolute increase in testing was small, it is important, as other interventions across the NCSP have generally not been able to produce a sustained increase in GP screening and an associated rise in positive tests. We recommend the NCSP and primary care commissioners consider using this intervention more widely in England and other countries with similar primary care services. Our analysis indicates that use of all parts of the intervention that influence different parts of the TPB components and ongoing support are important to attain the greatest increase in chlamydia screening tests. Our modified Zelen design should be considered more often in educational and public health research as it gives a much more realistic indication of take-up of the education and outcomes.
Key messages
-
A 76% increase in chlamydia screening tests and a 40% increase in infections detected can be attained across an area where GP surgeries are offered a multifaceted educational intervention.
-
Sixty-two per cent of randomly selected practices in the area fully engaged with the intervention, and only 17% refused any contacts; suggesting roll out more widely is feasible.
-
GP practices that fully engaged with the intervention, accepting an initial workshop and two further contacts with the support worker performed 2.33 times more screening tests during the intervention period compared with control practices.
-
The modified Zelen trial design gives unbiased information about uptake and success of interventions in randomly selected GP practices where routine outcome data are available, and as it is acceptable to practices, should be used more widely for evaluation.
Acknowledgments
We wish to thank all the practice staff involved in the development of the intervention, and the intervention itself, the NCSP coordinators and NCSP staff including Alireza Talebi who provided data. The laboratory staff who provided data, Pete Mathews for developing the website, Katie Elford and Jill Whiting for administration support and Gemma Lasseter for helping with ethics applications. Thanks to Heathville Road surgery for video development and Rosie Cox and Aislinn Watkins for giving their time to do the videos. Also thanks to Elizabeth Pottinger, Andrew de Burgh Thomas, the audit committee and PCT staff who willingly gave their time to make this trial possible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Annex 1
- Data supplement 2 - Online Annex 2
- Data supplement 3 - Online Annex 3
- Data supplement 4 - Online figures
- Data supplement 5 - Online table 3
Footnotes
-
AHH and EJR Joint second authors.
-
Handling editor Jackie A Cassell
-
Contributors CAMM had the idea for and led the project, was involved in evaluation and wrote the paper. AHH was involved with final design and delivery of the intervention, project management, data collection, was on the steering group and commented on the paper. EJR was involved in delivering the intervention, project management, data collection, evaluation, was on the steering group and commented on and approved the final paper. LW was involved with study design, led the TPB questionnaire, was involved with qualitative work and was on the steering group and commented on the paper. RC was involved with study design, was on the steering group and approved the paper. IO was involved with study design, was on the steering group and approved the paper. EO was involved in data collection, evaluation and commented on and approved the final paper; SK was involved with study design, was on the steering group and commented on and approved the final paper. AC was involved with study design, was on the steering group, led the statistical analysis, commented on and approved the final paper.
-
Guarantor(s) for the study Paul Boseley, Deputy Director, Research & Development Division, Public Health England, Porton Down, Salisbury, Wilts, SP4 0JG.
-
Funding This study was funded by a Health Protection Agency Research and Development grant (Grant Number: 107499). The funders had no influence on the design or running of this study.
-
Competing interests All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that ‘(1) CM, ER, AH, LW, RC, IS, EO, SK, AC have support from the Public Health England for the submitted work. Dr Cliodna McNulty leads the Public Health England Primary Care Unit that has an ongoing programme of work aimed at improving the management of infectious disease in primary care. Public Health England leads the National Chlamydia Screening Programme in England.
-
Ethics approval The study was approved in May 2008 from Warwickshire Research Ethics Committee (REC Ref: 08/H1211/57) and two further substantial amendments were approved in March 2010 and May 2011 (REC Ref: 08/H1211/167).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Statistical code (and/or) dataset is available from the corresponding author at cliodna.mcnulty@phe.gov.uk. Participants did not give consent for data sharing, but the presented data are anonymised and risk of identification is low.