Article Text

Abstract
Background Reducing HIV mother-to-child transmission (MTCT) is critical to ending the HIV pandemic. Reports suggest that herpes simplex virus-2 (HSV-2), a common coinfection in HIV-infected individuals, is associated with increased MTCT, but results have been conflicting. We conducted a systematic review of observational studies to quantify the magnitude of this relationship (PROSPERO no. CRD42016043315).
Methods We searched Medline (1981 to June week 3, 2016), EMBASE (1981 to week 26, 2016), relevant conferences (2013–2016) and bibliographies of identified studies for cohort and case–control studies enrolling HIV-positive women during pregnancy or peripartum that quantified the effect of HSV-2 infection on MTCT. The primary outcome was the risk of perinatal HIV transmission associated with maternal HSV-2 status. Risk of bias was evaluated using a standardised tool, and results were meta-analysed where appropriate using a random-effects model, with studies weighted using the inverse variance method.
Results From 2103 hits, 112 studies were considered for inclusion, and 10 were ultimately included. Of the included studies, three used a case–control design, three were retrospective cohorts and four were prospective cohorts. Risk of bias was low in three studies, moderate in six and high in one. The median sample size was 278.5 mother–infant pairs (range: 48–1513). The most common strategy for classifying maternal HSV-2 status was type-specific serology (n=6), followed by genital shedding (n=3) or genital culture (n=3), clinical diagnosis of herpes (n=2) or genital ulcer disease (n=1). Results from five studies that provided quantitative estimates of the association between HSV-2 seropositivity and MTCT were meta-analysed, yielding a pooled unadjusted OR=1.17 (95% CI=0.69 to 1.96, I2=58%). Three of these studies further considered key confounding variables, specifically antiretroviral use and/or viral load (n=3), and mode of delivery (n=2), yielding a pooled adjusted OR=1.57 (95% CI=1.17 to 2.11, I2=0).
Conclusions Maternal HSV-2 coinfection appears to be associated with increased perinatal HIV transmission. Further study of the effect of HSV-2 treatment on MTCT is warranted.
- herpesvirus-2
- HIV
- transmission
- coinfection
- infant
- mother
- human
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Combination antiretroviral therapy (cART) decreases mortality in HIV-infected persons, and decreases the risk of horizontal, vertical or mother-to-child HIV transmission (MTCT). Guidelines from the WHO recommend cART for all HIV-infected individuals, regardless of CD4 count or clinical status.1 Treatment of HIV-infected pregnant women is critical for reducing MTCT, but resource constraints limit access to cART.2 Until all HIV-infected persons can sustainably access cART, additional measures to decrease MTCT are needed.
Herpes simplex virus-2 (HSV-2) is a common coinfection in HIV-positive individuals (prevalence 60%–95%)3 associated with increased risks of HIV acquisition4 5 and transmission,6 7 even in HSV-asymptomatic individuals. Analogously, several reports suggest that HSV-2 is associated with increased MTCT, but results have been inconsistent.
To clarify this issue, and inform future MTCT reduction efforts, we conducted a systematic review and meta-analysis of available literature on this topic. Our primary objective was to quantify the impact of maternal HSV-2 coinfection on the risk of MTCT. Secondary objectives were to assess associations between maternal HSV-2 status and maternal HIV viral load (VL), maternal HIV shedding, infant CD4 count percentage and infant HIV VL.
Methods
Details of the protocol for this systematic review were registered on PROSPERO and can be accessed at www.crd.york.ac.uk/PROSPERO/.
Study eligibility criteria
Observational studies that examined the impact of HSV-2 coinfection on HIV MTCT were considered for inclusion into this study. Specific study eligibility criteria were: (1) cohort or case–control study design; (2) the study population was mother–infant pairs, where the mother was known to be HIV-1 or HIV-2 positive; (3) maternal HSV-2 status was determined using type-specific serology, virus detection (viral culture or PCR) or clinical diagnosis and (4) perinatal HIV transmission (including in utero and/or intrapartum transmission) was a study outcome.
Predictor variables
The primary predictor of interest was HSV-2 coinfection, determined using serologic testing (Western blot or enzyme immunoassay (EIA)). Because HSV-2 infection is incurable and frequently asymptomatic, determination of HSV-2 status is most accurately ascertained through HSV type-specific serology.8 These tests were developed in the early 1990s, but only became widely available as research tools in the last decade. As such, we recognised that earlier research may have ascertained HSV-2 status using less sensitive strategies, including clinical diagnosis and viral culture,9 but may still capture information about the impact of HSV-2 infection on HIV transmission; hence these studies were still considered. Individuals who are HSV-2 seronegative at baseline may acquire HSV-2 infection during the course of a study, thus attention was paid to whether studies assessed for seroconversion.
Outcomes
The primary outcome measure of interest for this review was the relative risk (RR) or odds ratio (OR) for perinatal HIV transmission associated with maternal HSV-2. HIV antibody tests are insufficient to diagnose neonatal HIV infection due to the passive transfer of maternal antibodies during pregnancy. Instead, virologic testing such as HIV DNA PCR is recommended at 14–21 days, 1–2 months and 4–6 months of life10; testing at birth may also be warranted. Two positive tests are required for a firm diagnosis,10 which was the preferred outcome definition used in this review. If a child is 18 months or older, it is acceptable to diagnose HIV using a standard antibody test and Western blot, since this is the length of time for passively acquired antibodies to disappear in uninfected children exposed to HIV.
Secondary outcomes of interest included maternal HIV VL and genital tract HIV shedding, and infant CD4 count percentage and HIV VL, at author-specified time points among those with documented perinatal HIV transmission.
Search methods for identification of studies
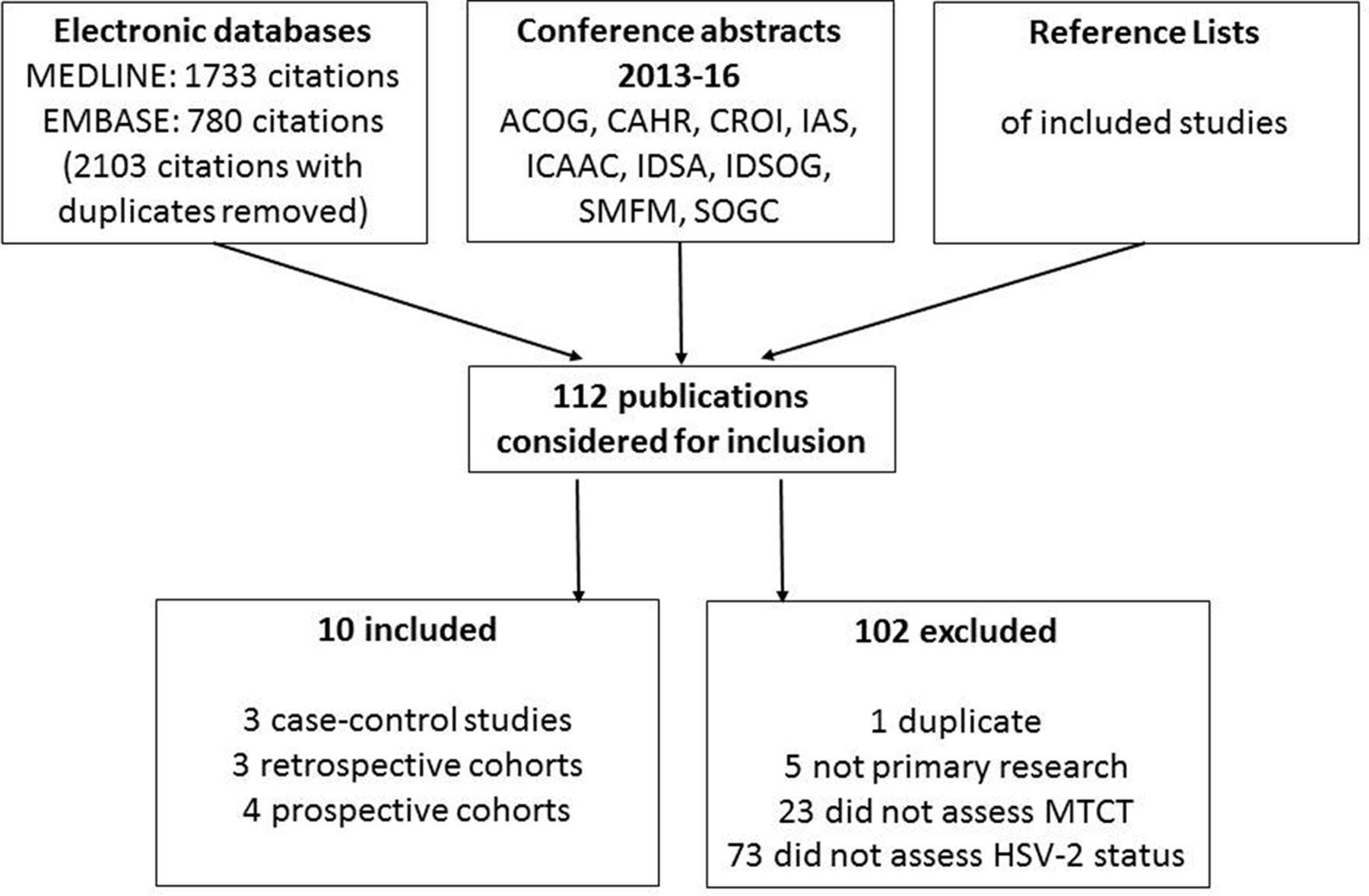
Publications were identified through searches of the Medline (1981 to June week 3, 2016) and EMBASE (1981 to 2016, week 26) electronic databases using search terms for HSV-2, HIV infection, pregnancy, vertical transmission and observational studies. Details of the search strategy are provided in PROSPERO. Conference proceedings from 2013 to 2016 were also searched from key research meetings (figure 1). Reference lists of eligible studies were also reviewed to identify others of potential relevance. No restrictions were imposed on publication language.

Flow chart of search strategy. ACOG, American Congress of Obstetricians and Gynaecologists; CAHR, Canadian Association of HIV Research; CROI, Conference on Retroviruses and Opportunistic Infections; IAS, International AIDS Society/World AIDS Conference; ICAAC, Interscience Conference on Antimicrobial Agents and Chemotherapy; IDSA, Infectious Diseases Society of America Annual Meeting; IDSOG, Infectious Diseases Society for Obstetrics and Gynaecology; SMFM, Society for Maternal Fetal Medicine; SOGC, Society of Obstetricians and Gynaecologists of Canada.
Selection of studies and data extraction
Two authors independently assessed abstracts and publications that appeared to meet eligibility criteria, and independently extracted study data; disagreements were resolved by consensus, with a third author available to resolve the issue if needed. Study authors were contacted a maximum of three times to supply missing data wherever possible.
Assessment of risk of bias
The risk of bias was assessed for each included study using a checklist of important study features that may impact data quality (table 1). This list of items was developed by reviewing the Strengthening the Reporting of Observational Studies in Epidemiology statement, a systematically developed and well-justified checklist of items deemed important for the reporting of observational studies.11
Criteria used for assessing the risk of bias in included studies
Analysis
Study characteristics were summarised descriptively. Findings from each study related to the primary objective were summarised as an RR or OR. Unadjusted and adjusted effect sizes were extracted, and predictor variables considered in multivariable models were noted. For the primary outcome, the RR and/or OR were meta-analysed where clinically appropriate (meaning that critical confounders as identified in table 1 were appropriately accounted for) using a random-effects model, with weighting of studies according to the inverse variance method.12 Heterogeneity was quantified using the I2 statistic.
Sensitivity analyses were conducted to determine whether results differed according to the use of fixed versus random effects models, and according to study quality. Subgroup analyses were planned to examine HIV MTCT according to the number of maternal antiretroviral agents used, by use of anti-HSV-2 medications and mode of delivery (Caesarian vs vaginal delivery).
Results
Studies included for review
The search strategy identified 2103 articles through electronic databases; no additional studies were identified from searching relevant conference literature or reference lists (figure 1). Of these, 112 full articles were reviewed, and 10 were ultimately included (table 2). The median study size was 279 mother–infant pairs, with a range of 48–1513.
Characteristics of included studies and assessment of the risk of bias*
Assessment of the risk of bias
The risk of bias varied among included studies (table 2). Eligibility criteria were generally well explained, with most studies nested within larger, previously described cohorts or clinical trials. Six studies ascertained HSV-2 status serologically,13–18 including four that used the HerpeSelect HSV-2 EIA (Focus Diagnostics, Cypress, California, USA).13–15 17 The primary method for classifying maternal HSV-2 status varied in quality among the other four studies, ranging from low (routine viral culture at delivery21) to moderate (protocolised clinical assessments with or without viral culture during pregnancy19) to high (clinical diagnosis at any time during pregnancy23 or no details provided22) risk of bias. Laboratory methods for defining infant HIV status were clearly described and involved appropriate use of PCR- and antibody-based testing in all but one study, in which inadequate detail was provided.21
Methods to account for confounding varied, with only three studies adjusting for, or considering adjusting for, mode of delivery and maternal antiretroviral medication use16 17 19 (a fourth did not require such adjustment because no antiretroviral medications were available), and most studies not performing adjusted analyses at all. No studies controlled for use of infant prophylaxis or anti-HSV medications, although usage was known or expected to be low in most cases. No studies controlled for feeding strategy. Statistical analyses were conducted appropriately, although only two studies provided a sample size calculation.13 14 Most studies had a moderate (10%–20%) amount of attrition.
Primary outcomes
HSV-2 seropositivity as a predictor of MTCT
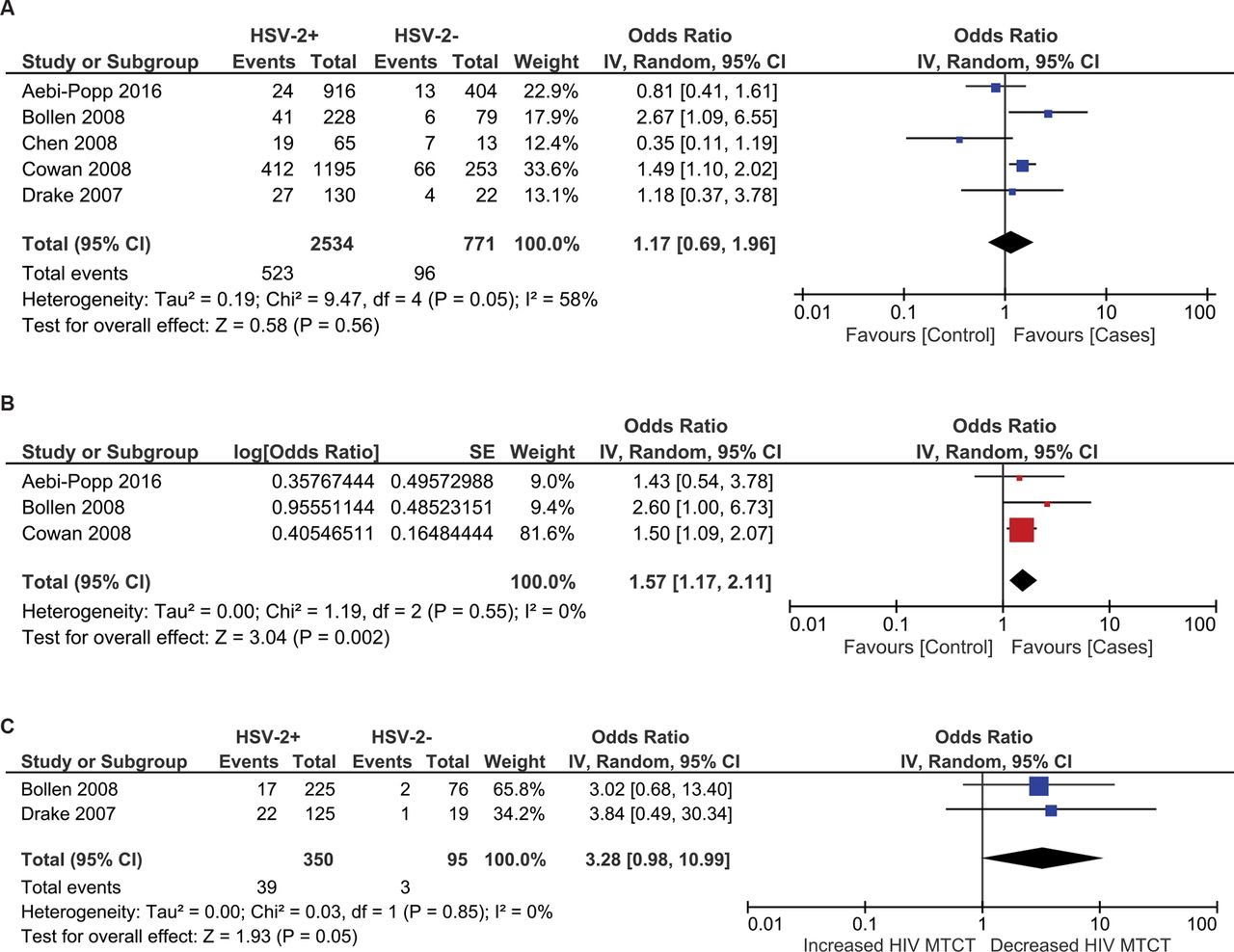
Of the six studies that assessed HSV-2 serostatus, one did not quantify the effect of HSV-2 seropositivity on MTCT and reported qualitatively that HSV-2 serostatus was not significant in univariate analysis for HIV infection by 24 months of age.18 Results from the remaining five studies were meta-analysed (figure 2A) and yielded a pooled OR=1.17 (CI=0.69 to 1.96, p=0.56) for MTCT associated with maternal HSV-2 infection and moderate heterogeneity (I2=58%).
{kind=link}
{kind=link}
(A) Forest plot of the impact of HSV-2 seropositivity on MTCT (unadjusted analysis). (B) Forest plot of the impact of HSV-2 seropositivity on MTCT (adjusted analysis). (C) Forest plot of the impact of HSV-2 seropositivity on intrapartum MTCT (unadjusted analysis). HSV-2, herpes simplex virus-2; MTCT, mother-to-child transmission.
Three of these studies considered maternal antiretroviral use and/or HIV VL near the time of delivery (in one case because antiretrovirals were unavailable in the population studied) in multivariable models.14 16 17 Two of these three studies further considered mode of delivery.16 17 Meta-analysis of the adjusted effect sizes from these three studies was performed (figure 2B), and yielded a pooled adjusted OR (aOR)=1.57 (95% CI=1.17 to 2.11). Assessment of heterogeneity between these generally well-executed studies, conducted in Ukraine, Thailand and Zimbabwe, yielded a negative I2 value, which is traditionally reported as zero.20 A fixed effects model yielded identical results.
In a sensitivity analysis including the two studies at low risk of bias, the association with MTCT was strengthened, with a pooled aOR=1.63 (95% CI=1.19 to 2.42). This analysis included a Zimbabwean study among 1448 women that adjusted for maternal HIV VL within 96 hours of delivery, CD4 count, haemoglobin, education, arm circumference and infant weight (no antiretrovirals were available at the time)14 and another among 307 women in Thailand that adjusted for zidovudine use, HIV VL at delivery, CD4 count at 36 weeks and cervicovaginal VL at 38 weeks.17 A fixed effects model yielded similar results (OR=1.59, 95% CI=1.17 to 2.16, I2=0%).
Of note, because HIV VL at/near the time of delivery may be along the causal pathway from HSV-2 seropositivity to intrapartum MTCT, the incorporation of this variable into the adjusted estimates from these two studies may underestimate the true effect of HSV-2.14 17 The pooled unadjusted estimate from these two studies was OR=1.70 (95% I=1.06 to 2.74, I2=31%). However, HSV-2 could also increase in utero MTCT by influencing HIV VL during pregnancy. Most studies did not explicitly distinguish intrapartum from in utero HIV transmissions, the latter conventionally being distinguished by infant HIV PCR seropositivity within 48–72 hours of birth. However, two studies reported data on in utero transmissions separately (figure 2c),15 17 permitting us to calculate unadjusted ORs and a pooled OR=3.28 (95% CI=0.98 to 10.99, I2=0%). Most studies did not assess for HSV-2 seroconversion.
HSV-2 shedding
Three studies examined the relationship between genital HSV-2 shedding and MTCT, but timing of the assessments varied. A Thai study found an association between MTCT and HSV-2 shedding in cervicovaginal lavage fluid at 38 weeks gestation (OR=3.0, 95% CI=1.2 to 7.4), but this was no longer statistically significant after adjustment for ART use, maternal CD4 count, plasma VL at delivery and cervicovaginal HIV VL at 38 weeks (OR=2.3, CI=0.9 to 6.2).17 The two other studies assessed shedding either at 10–32 weeks gestation, or at delivery; neither found an association with intrapartum or in utero MTCT in univariate analyses.13 15
HSV-2 culture
Three studies classified maternal HSV-2 status according to the presence of positive HSV-2 culture results, but ascertainment methods differed considerably. In a study from New York City, medical records from 21 women clinically diagnosed with genital HSV infection were reviewed for positive HSV (not type-specific) cultures.19 In a study including 48 HIV-infected women in Seattle, genital and cervical cultures were routinely collected within 48 hours of delivery.21 In a third study, laboratory methods for diagnosing HSV infection were not stated but likely involved viral culture given the setting (USA, 1990s).22 We calculated crude ORs for all three studies using data in the original reports, and found no significant associations with MTCT (table 3).
Relationship between maternal herpes simplex virus-2 (HSV-2) and HIV vertical transmission
Clinical diagnosis
Two studies used clinical diagnosis as a measure of herpes status (table 3), defined as having a history of genital HSV during pregnancy19 23 or any point in the past.23 The higher quality study, conducted among 402 women in New York City, found a positive association with MTCT that persisted after adjustment for maternal zidovudine use, prolonged rupture of membranes (PROM), and preterm delivery, yielding an aOR of 4.8 (95% CI=1.3 to 17.0).
Genital ulcer disease
One study among 175 Kenyan women found that the presence of genital ulcer disease (GUD) at 32 weeks gestation was positively associated with MTCT (table 3). This association persisted after adjustment for maternal plasma HIV VL at delivery (aOR=5.1, 95% CI=1.1 to 24.1).15
Subgroup analyses
Quantitative subgroup analyses based on maternal antiretroviral use, anti-HSV medication use and mode of delivery were not possible due to the small number of studies identified.
Secondary outcomes
Two studies reported maternal HIV VL according to HSV-2 status, but all analyses were cross-sectional.20 23 Drake et al observed similar or higher viral loads in women with HSV-2 seropositivity, HSV shedding at delivery, and GUD at 32 weeks, but only the latter reached statistical significance.15 Bollen et al reported borderline higher maternal HIV VL at 38 weeks among HSV shedders versus non-shedders (4.2 vs 4.1 log10copies/mL, respectively, p=0.05) and among HSV-2 seropositive versus seronegative participants (4.1 vs 4.0 log10copies/mL, respectively, p=0.09).17 None of the included studies reported on HSV-related differences in our other secondary outcomes.
Discussion
HSV-2 is a common, lifelong infection characterised by periodic clinical and subclinical reactivations. Several studies have examined the effect of maternal HSV-2 status on HIV MTCT, but ours is the first to systematically review this literature. Our meta-analysis suggests that after considering important confounders, particularly maternal antiretroviral use and mode of delivery, HSV-2 seropositivity is significantly associated with an increased odds risk of MTCT, with a pooled aOR=1.57 (95% CI=1.17 to 2.11, I2=0).
While we were unable to meta-analyse studies that used other strategies for classifying maternal HSV-2 status due to the paucity of data and diversity of methods used, adjusted analyses from those studies reached similar conclusions. Specifically, the aOR for the impact on MTCT was found to be 4.8 (95% CI=1.3 to 17.0) for any clinical diagnosis of genital herpes during pregnancy,19 and 5.1 (95% CI=1.1 to 24.1) for the presence of GUD at 32 weeks gestation.15 HSV-2 shedding at 38 weeks gestation was nearly significant, with aOR=2.3 (95% CI=0.9 to 6.2).17 These studies did not always account for key confounders such as antiretroviral use and mode of delivery, but the direction in which such omissions may bias these findings is unclear. Our findings are also consistent with other studies reporting an increase, although not statistically significant, in the risk of MTCT with GUD.24 25
While two-thirds of vertical HIV transmissions are thought to occur intrapartum in the absence of prophylaxis and breast feeding,26 of pathophysiologic interest is whether HSV-2 also increases in utero HIV transmission. Only two studies explicitly distinguished between these scenarios.15 17 Pooling of unadjusted analyses quantifying the association between HSV-2 seropositivity and in utero transmission yielded an overall OR=3.28 (95% CI=0.98 to 10.99), but neither article conducted adjusted analyses for this outcome, likely due to low numbers of events. Given that HSV-2 reactivations during the antenatal period (ie, clinical diagnoses, GUD, HSV-2 shedding weeks before delivery) seem to be associated with MTCT overall, it seems likely that many of these HIV transmission events occur in utero. Alternatively, antenatal HSV-2 reactivations may simply predict intrapartum HSV reactivations that in turn increase neonatal exposure to HIV during delivery. In addition, because two of the included studies adjusted for HIV VL at or near the time of delivery, which may be along the causal pathway from HSV-2 seropositivity to intrapartum MTCT, our pooled adjusted odds ratios might disproportionately reflect in utero transmission events. Future studies should differentiate between these possibilities, as they have different implications regarding the optimal timing for intervention.
Analogous to our findings on MTCT, studies have also suggested that HSV-2 increases horizontal HIV transmission6 7 by increasing HIV replication in both the plasma and genital compartments. Many molecular mechanisms for this epidemiologic synergy have been proposed.27–30 Of note, a prior systematic review found no studies linking HSV-2 seropositivity to statistically significant increases in plasma HIV VL, and only one study linking genital HSV-2 shedding with increased plasma HIV viremia.31 However, a meta-analysis suggested that HSV-2 is associated with increases in HIV plasma VL, and that HIV plasma VL was significantly reduced by HSV-2 treatment.32 These contrasting conclusions are likely due to methodological differences between these reviews. Moreover, HIV is present at high levels in herpetic ulcers,33 and longitudinal analyses suggest a positive association between HSV-2 and HIV shedding in the female genital tract.34
Regardless of mechanism, our finding that HSV-2 seropositivity is associated with MTCT suggests that anti-HSV therapy may be warranted in HIV/HSV-2 coinfected pregnant women without access to cART. Although current WHO guidelines strongly recommend the ‘Option B+’ strategy of universal cART for all HIV-infected pregnant women, uptake remains inadequate, with a recent review showing that 30% of such women in prevention of MTCT (PMTCT) programmes in Sub-Saharan Africa did not receive any antiretroviral prophylaxis.35 As programmes continue to increase cART access, a clinical trial could assess the incremental benefit of anti-HSV therapy, but the required sample size may prove challenging. Assuming a 25% baseline risk of vertical transmission in the absence of any PMTCT interventions,36 315 participants would be required in each arm of a 1:1 randomised trial to test the hypothesis that the 1.57-fold increase in MTCT associated with HSV-2 seropositivity could be completely reversed by therapy, with 80% power and alpha=0.05. The required sample size per arm increases rapidly to 1114 if the transmission rate in the control arm is 8.4% (as seen with the PACTG 076 zidovudine regimen37), 1573 if 6% (single dose mother/infant nevirapine plus zidovudine38 39) and 4884 if 2% (cART).36
A trial of anti-HSV therapy was conducted in the context of horizontal transmission, and disappointingly found that twice daily acyclovir 400 mg did not prevent HIV transmission from HSV-2/HIV coinfected adults to seronegative partners.40 However, subsequent work has shown that this dosing provides incomplete HSV-2 suppression,41 suggesting that higher doses or alternative medications may be required. Yet a 12-week crossover trial found that valacyclovir 500 mg twice daily reduced plasma HIV VL by 0.37 log10 copies in 18 cART-untreated HIV/HSV-2 coinfected adults, suggesting direct anti-HIV activity.42 Another trial that randomised 148 HIV/HSV-2 coinfected pregnant Kenyan women to valacyclovir 500 mg twice daily versus placebo showed 0.51–0.56 log10 copies/mL reductions in breast milk and plasma HIV RNA, respectively,43 providing further support for the safety44 and acceptability of this intervention in pregnancy.
Strengths of our study include our broad search strategy that included multiple infectious diseases and obstetrics research conferences, and no language restriction. We also observed no significant heterogeneity in our meta-analysis of adjusted effect sizes quantifying the relationship between HSV-2 seropositivity and MTCT.
A limitation of this review was that studies included in our meta-analyses did not all adjust for important confounders, including mode of delivery, considered in two of three studies in the adjusted pooled analysis, as well as infant ARV prophylaxis and anti-HSV medication use, both of which were seldom reported on but likely uncommon. Conversely, obstetrical factors that increase MTCT such as PROM and preterm birth were also generally omitted, as was feeding strategy, though breast feeding was unlikely or reported to be negligible in most included studies.
Maximising cART access for HIV-infected pregnant women must remain the primary objective for PMTCT programmes worldwide. However, implementation gaps, and our finding of a significant increase in MTCT with HSV-2 coinfection, suggest that further efforts to treat and prevent HSV-2 in this population are warranted.
Key messages
Prior to this review, several studies have attempted to quantify the correlation between maternal herpes simplex virus-2 (HSV-2) seropositivity and increased mother-to-child transmission (MTCT), but results have been conflicting.
HSV-2 seropositivity is associated with an increased odds of MTCT.
It is unclear whether HSV-2-related increases in HIV transmission occur in utero, intrapartum or both.
Although providing combination antiretroviral therapy to all HIV-infected pregnant women is the key priority for the prevention of vertical transmission, the incremental benefit of HSV-2 suppression in this setting may warrant further study.
References
Footnotes
Acknowledgements We thank Elizabeth Uleryk for her assistance in developing and conducting the search strategy for this systematic review.
Contributors All authors contributed significantly to the work, as follows: DHST conceived the study idea; DHST designed the protocol in consultation with MHY and KEM; VS and KV conducted database searches; VS, KV, SAM and DHST selected eligible articles for inclusion; KV and VS conducted the data extraction; DHST, KV and VS designed and conducted the statistical analysis; VS and DHST wrote the original draft of the manuscript; all authors provided critical input into and approved the final version of the manuscript.
Funding DHST is supported by a New Investigator Award from the Canadian Institutes of HealthResearch / Ontario HIV Treatment Network.
Competing interests DHST has received honouraria from Abbvie, Gilead, Merck and Viiv Healthcare, has been awarded grants for investigator-initiated studies from Gilead and Viiv Healthcare and is a site principal investigator for clinical trials sponsored by GSK.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with ’BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.