Article Text

Abstract
Objective In mid-2017, the Victorian Government funded a free time-limited human papillomavirus (HPV) vaccination catch-up programme for gay and bisexual men who have sex with men (MSM) aged up to 26 years through sexual health clinics or other immunisation centres. We aimed to examine the uptake of the HPV vaccine among young MSM attending the Melbourne Sexual Health Centre (MSHC).
Methods MSM aged ≤26 attending MSHC between 27 April 2017 and 31 December 2017 were included in the analysis. HPV vaccine uptake was calculated based on the first consultation of each patient during the period. Multivariable logistic regression was performed to examine the association between vaccine uptake and patient factors.
Results There were 2108 MSM aged ≤26 who attended MSHC over the study period, with 7.6% (n=161) reporting previous HPV vaccination. Of the 1947 eligible men, 1134 (58.2%, 95% CI 56.0% to 60.4%) were offered the vaccine by the clinicians, and 830 men received it on the day. The vaccine coverage among all eligible MSM was 42.6% (95% CI 40.4% to 44.9%; 830 of 1947) and among MSM who were offered the vaccine by the clinicians was 73.2% (95% CI 70.5% to 75.8%; 830 of 1134). Men with a history of genital warts (adjusted OR (aOR)=3.11, 95%CI 1.39 to 6.99) and those who had >4male partners in the last 12 months (aOR=1.38, 95% CI 1.04 to 1.85) were more likely to receive the HPV vaccine on the day. 304 men declined the vaccine; most men did not specify the reason (31.3%, n=95), while 27.3% (n=83) needed time to think.
Conclusion Although vaccine uptake was 73.2% among those offered, the actual coverage of those eligible remained unsatisfactory (42.6%) in a sexual health clinic. This highlights a clinic-based targeted MSM programme may not reach sufficiently high vaccine coverage to provide MSM with the same vaccine benefits as heterosexuals.
- vaccination
- HPV
- gay men
- prevention
- MSM
Statistics from Altmetric.com
Introduction
Human papillomavirus (HPV) is one of the most common sexually transmitted infections (STIs) worldwide.1 In 2007, Australia introduced a school-based HPV vaccination programme for girls aged 12–13 years and a catch-up programme which ran for 2 years and vaccinated females up to the age of 26 years. This female-only vaccination has reduced genital warts by at least 69%2 and the oncogenic vaccine-preventable HPV genotypes (16/18) by 87%.3 Several studies have demonstrated that unvaccinated heterosexual males also received substantial herd protection from the female-only vaccination programmes.4–7 However, gay and bisexual men who have sex with men (MSM) are unlikely to receive benefit from the female-only vaccination programme.6
MSM are likely to eventually be protected because in 2013 the Australian school-based HPV vaccination programme was expanded to include boys aged 12–13 years, followed by a 2-year catch-up programme for boys aged up to 15 years.8 The burden of HPV infection is high among MSM, with the incidence of anal cancer among MSM being similar to the incidence of cervical cancer before screening was in place.9 Therefore, it is important, in addition to the school-based programme for boys, to consider vaccinating younger MSM to reduce the burden of HPV infection and future risk of anal cancer. Indeed vaccinating MSM with a catch-up programme in addition to the school-based programme for boys is likely to have significant benefits and to be cost-effective.10
In April 2017, the Victorian Government funded a time-limited catch-up HPV vaccination programme for MSM across the state of Victoria, Australia. All MSM in Victoria and aged up to 26 years are eligible to receive a three-dose course of quadrivalent HPV vaccine free of charge at sexual health clinics and through other immunisation providers until 31 December 2018. To date, in Australia, the quadrivalent HPV vaccine is only registered for use in males aged between 9 and 26 years old.11 In January 2018, the Victorian Government has also launched two other vaccination programmes for MSM (hepatitis A vaccine and meningococcal ACWY vaccine). A state-based vaccination campaign was launched in January 2018 in Victoria and aimed to increase the uptake of the three vaccines in MSM living in Victoria together with the ongoing free hepatitis B vaccination programme. The HPV vaccine coverage in boys that is required to provide MSM with the same benefits as heterosexuals is not known but has been estimated to be of the order of 70%.10 The primary aim of this study was to examine the HPV vaccination uptake among MSM aged 26 or under at a sexual health clinic setting from the catch-up programme. The secondary aim was to explore the predictors of the HPV vaccine uptake among young MSM.
Methods
This was a retrospective cohort study of MSM aged 16–26 years attending the Melbourne Sexual Health Centre (MSHC) between 27 April and 30 December 2017. MSHC is the largest public health service in the state of Victoria, Australia. The clinic provides about 50 000 consultations per year; 37% of these patients are MSM.12 On arrival to MSHC, all patients are asked to complete a computer-assisted self-interview (CASI), which collects demographic characteristics (eg, age and country of origin), sexual history (eg, sex work, number of partners and condom use in the last 12 months, history of genital warts, and use of pre-exposure prophylaxis (PrEP) for HIV) and HPV vaccination status.
On 27 April, MSHC started to provide free HPV vaccine to eligible MSM as part of the time-limited catch-up programme. Men who were 26 or under and had self-reported as having sex with another man in the last 12 months attending MSHC during the study period were eligible to receive the HPV vaccine for free. Men who self-reported having been vaccinated against HPV were not eligible and excluded from the analysis. To remove the bias of multiple visits among patients during the study period and to ensure a consistent measure, we only included the first consult of the patients in the study period in the final analysis. Sensitivity analysis was performed among patients who did not receive the vaccine at the first consult but had subsequently received vaccine within 3 months from initial visit and this was expanded to include patients seen until 31 March 2018; hence, each individual had 3 months of follow-up.
Patients were seen by clinicians including sexual health physicians, sexual health nurses and general practitioners with considerable experience in sexual health. There was no formal training for clinicians on offering the HPV vaccine; however, all clinicians have considerable experience in offering other vaccines (eg, hepatitis A and B vaccines) to MSM attending MSHC before the launch of this HPV catch-up programme for MSM. Regular education sessions on the benefit of HPV vaccine were provided to clinicians via internal communication such as seminar presentations.
Clinicians offered the HPV vaccine to the patients based on the eligibility criteria and vaccination status. The self-reported HPV vaccination status is available on an electronic Clinic Practice Management System (CPMS) for clinicians, and a text reminder automatically appears at the top of the consultation page in the medical record of all eligible MSM. Administration of HPV vaccine for each patient was recorded on the CPMS. A retrospective chart review of each patient’s first consult was performed to collect information on vaccine offering and reasons of patients who declined to receive the vaccine. A patient was deemed to have been ‘offered’ the vaccine if there was text clearly describing this in the electronic health record.
Univariable logistic regression model was performed to examine the association between the HPV vaccine uptake and patients’ demographic characteristics and sexual practices, and this analysis was restricted to patients who were offered the vaccine documented on the CPMS. Continuous variables such as the number of male partners in the last 12 months were stratified at the median. Previous studies found that the HPV vaccine uptake in females was associated with history of sexual behaviours (ie, history of genital warts, number of partners and condom use), demographic characteristics (country of birth) and sexual orientation,13 14 and these factors were considered as independent variables in the present analysis. Age was categorised in ‘16–19 years’ and ‘20–26 years’ based on the fact that the majority of males aged 16–19 years would have been eligible for the school-based programme for boys launched in 2013 (ie, they had to be at school in Australia since 2013) and males aged 20–26 years would have not been eligible to receive the free vaccine from the school-based programme. Men were categorised as ‘homosexual’ if they reported having sex with men only and as ‘bisexual’ if they reported having sex with men and women in the last 12 months. Variables with a p>0.10 in the univariable analysis were included in the multivariable analysis.15 The Hosmer-Lemeshow test was used to determine the goodness of fit of the logistic regression model.
Results
Demographic characteristics
There were 2108 MSM aged 16–26 years attending MSHC during the study period; 161 (7.6%) had self-reported being previously vaccinated against HPV and were excluded (figure 1). Of the 134 MSM aged 16–19 years, 101 MSM would have been eligible for school-based and catch-up programme and only 27 (26.7%) MSM self-reported they had been vaccinated against HPV at school. Of the remaining 1947 men who were eligible for the vaccine, the median age was 24 years, 889 (45.7%) were born outside Australia and 68 (3.5%) were HIV-positive.
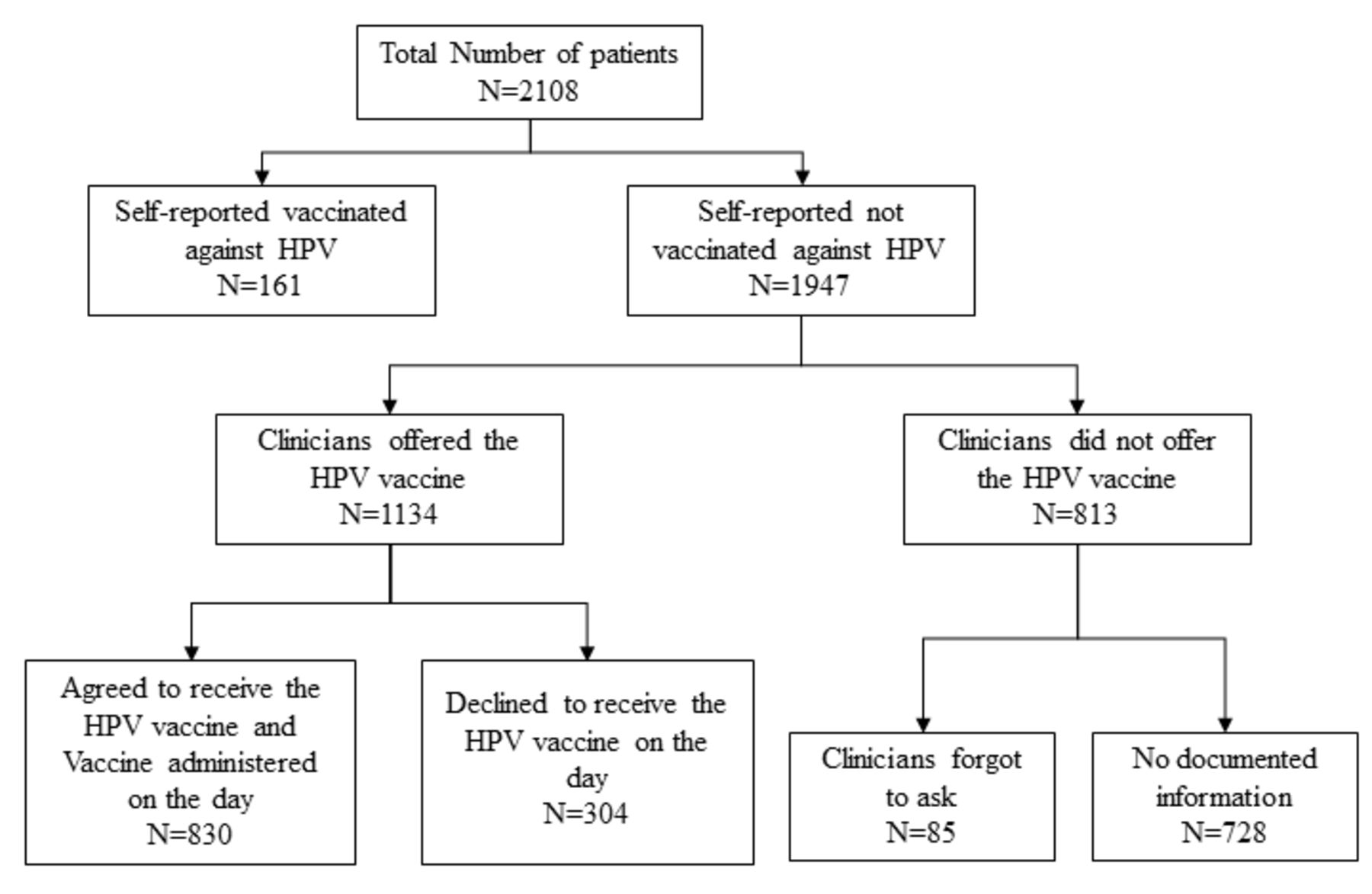
Flow chart of data selection for the final analysis. HPV, human papillomavirus.
HPV vaccine coverage among MSM at a sexual health clinic setting
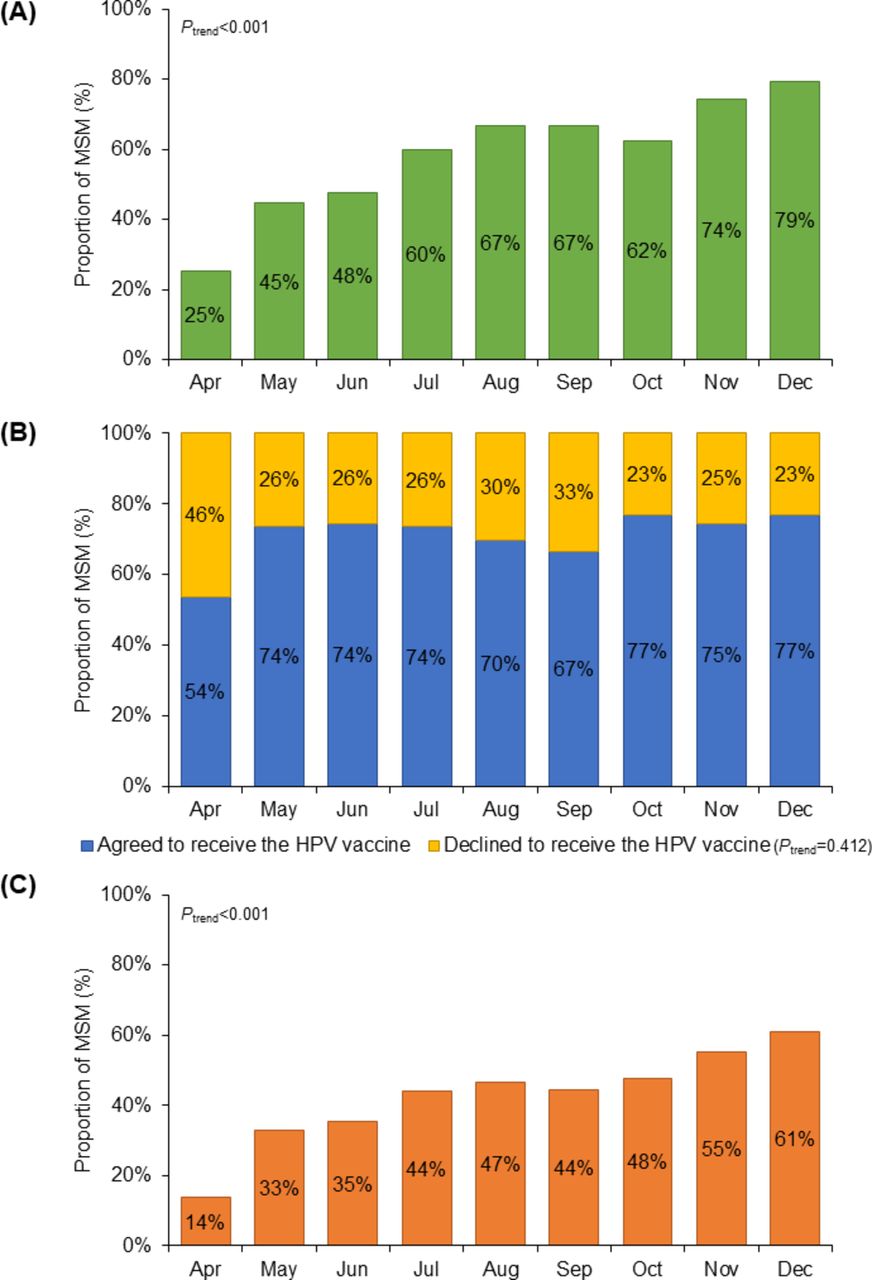
Only 58.2% (95% CI 56.0% to 60.4%; 1134 of 1947) of men were offered the vaccine by the clinicians, and this proportion increased from 25% in April to 79% in December (ptrend<0.001) (figure 2A). Of the 1134 men who were offered the vaccine, 830 (73.2%) agreed and received the vaccine on the day, and the proportion of men who agreed and received the vaccine did not change over the study period (ptrend=0.412) (figure 2B). The overall HPV vaccine coverage among all eligible MSM was 42.6% (95% CI 40.4% to 44.9%; 830 of 1947), and it significantly increased from 14% in April to 61% in December (ptrend<0.001) (figure 2C). Sensitivity analyses showed that of the 813 men who did not receive the vaccine at the first consult, an additional 152 men received the vaccine in a subsequent clinic visit within 3 months. This increased the vaccine coverage to 50.4% (95% CI 48.2% to 52.7%; 982 of 1947).
{kind=link}
{kind=link}
Proportion of MSM aged 16–20 years who (A) were offered the HPV vaccine by the clinician; (B) agreed declined to receive the HPV vaccine among those who were offered the vaccine; and (C) received the HPV vaccine among all eligible MSM attending the Melbourne Sexual Health Centre, stratified by month, from April to December 2017. HPV, human papillomavirus; MSM, men who have sex with men.
Factors associated with HPV vaccine uptake among men offered the vaccine
Men aged 20–26 years (74.0%) had a higher HPV vaccine uptake rate compared with men aged 16–19 years (54.3%). However, the HPV vaccine uptake rate did not differ among men aged between 20 and 26 years (ptrend=0.522). HPV uptake rate was not associated with men being sex workers, indigenous origin and HIV status (table 1).
Factors associated with the uptake of HPV vaccine among 1134 gay and bisexual men who have sex with men attending the Melbourne Sexual Health Centre
Multivariable analysis showed that men who reported a history of genital warts had the highest odds of receiving the vaccine (adjusted OR: 3.11, 95% CI 1.39 to 6.99) (table 1). In addition, men who had more than four male partners had 1.38-fold (95% CI 1.04 to 1.85) higher odds of taking the HPV vaccine compared with men who had four or less male partners in the last 12 months. The Hosmer-Lemeshow test suggested a good fit between the logistic model and the data (p=0.436).
In the univariable analysis, men who were taking PrEP had 2.40-fold (95% CI 1.25 to 4.61) higher odds of receiving the HPV vaccine than men who were not taking PrEP (86.1% vs 72.1%). Similarly, homosexual men had 1.78-fold (95% CI 1.11 to 2.87) higher odds of receiving the vaccine than bisexual men (74.1% vs 61.5%). Men with inconsistent condom use had 1.35-fold (95% CI 1.01 to 1.81) higher odds of receiving the HPV vaccine compared with men with consistent condom use in the last 12 months (73.4% vs 67.2%). However, the association between the HPV vaccine uptake and these three factors—PrEP use, sexual practice and condom use—was not significant in the multivariable analysis after adjusting for other potential confounding factors.
There were 304 men who declined to receive the vaccine on the day; 95 (31.3%) did not have a specific reason documented on their medical files (table 2). The two leading reasons were ‘time to think’ (27.3%; n=83) and ‘unsure of immunisation records’ (13.5%; n=41). Other reasons included travelling (7.9%; n=24), time constraint (7.9%; n=24) and issues with needles (3.3%; n=10). Of the 304 men who declined to receive the vaccine on the day, 46 (15.1%) received the vaccine subsequently within 3 months at MSHC.
Reasons for declining to receive the HPV vaccine and subsequently received the HPV vaccine within 3 months among 304 men who have sex with men
Discussion
The purpose of this study was to examine the uptake of the HPV vaccine in MSM aged 16–26 years attending MSHC after the launch of a time-limited HPV vaccination catch-up programme for MSM aged up to 26 years in Victoria, Australia. We found that the HPV vaccine uptake was 42.6% among all eligible MSM aged 16–26 years attending MSHC on their first consult during the study period. HPV uptake was associated with a history of genital warts and higher number of male partners after adjusting for other potential confounding factors. While it is not yet known what coverage of MSM would be required to achieve the same dramatic declines achieved in heterosexuals, it has been suggested it needs to be at least as high as heterosexuals based on the higher rate of partner change,10 and the potentially greater and longer duration of infectiousness at the anus.16 These factors, combined with the rapid acquisition of HPV in young MSM and high rates of partner change before vaccination, suggest that a 42% coverage will not be sufficient to see dramatic declines in HPV and substantial herd protection.
There are several limitations in this study. First, we used only the first consult to calculate the vaccine coverage and therefore will have underestimated the coverage if this targeted programme continues for some years. We restricted the analysis to the first consult only because the clinic is set up to provide all services to patients at a single consultation and not require repeat attendances but some men will return for treatment of diagnosed STIs and routine check-up. We therefore undertook a sensitivity analysis to include men who had at least one repeated visit within 3 months, and we found that a further 152 eligible MSM who did not receive the vaccine at the first consult received the vaccine in the repeat visit. This changed the overall vaccine coverage from 42.6% to 50.4%. Second, self-reporting and recall biases might have occurred on reporting the HPV vaccination status on CASI. We were unable to verify their vaccination status through the national HPV registry in this study. Third, the nature of medical records was primarily for clinical care and therefore recording of HPV vaccine information was incomplete. Some clinicians may not have documented whether the vaccine was offered and the reason for declining to receive the vaccine. There were 728 (37.4%) patient medical records that did not have any information recorded in relation to an offer of an HPV vaccine. Incomplete recording would have increased the refusal rate but not have changed the vaccination rate because administration of the vaccine requires an electronic order. Fourth, this study was conducted at a single urban sexual health clinic. It is possible that MSM attending a sexual health clinic are more sexually active and have better knowledge and awareness of sexual health. Thus, findings from this study may not be generalisable to other MSM in other settings and in the community.
Despite the uptake rate of HPV vaccine being 73.2% (830 of 1134) in those who were offered, the overall vaccine coverage of eligible men is suboptimal (42.6%; 830 of 1947). It is possible that clinicians did not offer the vaccine or clinicians offered the vaccine but the patients declined it. A low offering rate because of the vaccine being recommended more commonly than recorded could be due to several factors, such as patients having long and complicated consultations. It is also possible that clinicians might have prioritised other clinical issues with patients, such as complicated clinical cases, or new diagnoses of HIV or STI. Due to the nature of retrospective chart records, we were unable to identify all the reasons that clinicians did not offer the vaccine to the patients. Although previous studies have shown that low recommendation rates may be due to lack of knowledge by healthcare professionals about the HPV vaccine17 18 and undisclosed same-sex attraction of patients,19 these might not be the case at a major sexual health clinic. Given 42% of the MSM were not offered the vaccine by the clinicians, further investigation and discussion with the clinicians would be required to understand the barriers of not offering.
In 2016/2017, England launched a pilot programme providing free HPV vaccines for MSM aged up to 45 years through 42 sexual health clinics. The vaccine coverage rate in England was 45.5%, which is similar to the coverage at our clinic (42.6%).20 About 15.6% of eligible MSM in our clinic declined to receive the vaccine, which is higher than the rate observed in England (3.4%). MSM declined the vaccine in our study due to a range of reasons, and these included the need for time to consider the information and to have more time to go through an information leaflet. This is consistent with a study conducted in England,21 suggesting that the knowledge surrounding the HPV vaccine and the virus itself is limited among MSM. Patients’ lack of knowledge regarding their own immunisation status is also a significant factor causing vaccine uptake hesitancy as some men would have been vaccinated from the universal school-based vaccination programme in Australia. Other interventions such as patient education and use of patient reminder and recall systems might be useful to increase the HPV vaccine uptake rate among MSM at clinic.22
It is also worth to note that this analysis only included 10-month data (from April to December) in 2017. The uptake rate may increase by extending the study period to 12 months. However, if the uptake rate increased in this period, it is difficult to interpret whether such increase was due to the introduction of the ‘Little Pricks’ vaccination campaign in January 2018 to encourage MSM to receive four free vaccines (HPV, hepatitis A, hepatitis B and meningococcal ACWY) or related to other confounding factors such as the holiday season. A more comprehensive analysis of HPV vaccine uptake rate for the whole year of 2018 will be required. It is likely the uptake rate in 2018 will increase due to the introduction of the vaccination campaign and the availability of other free vaccines.
We found that men with a history of genital warts had the strongest association with receiving the HPV vaccine. This could be because these men with history of genital warts were more aware of HPV.23 Men aged 20–26 years were more likely to receive the vaccine than men aged 16–19 years, but this may have been related to younger men having already received the vaccine through the school-based programme. Higher HPV vaccine uptake rate among men with higher number of partners will improve the overall effectiveness and cost-effectiveness of this time-limited catch-up programme because they are at a higher risk of acquiring HPV.24 25 The association between HPV uptake and PrEP use also highlights the fact that patients who take a positive approach to looking after their sexual health are more likely to protect themselves with the vaccine.
Previous studies have demonstrated a dramatic reduction in genital warts and vaccine-preventable HPV genotypes (6/11/16/18) among females after the introduction of the female-only vaccination programme with vaccine coverage of at least 70%.2 3 Similar reductions have also been observed among unvaccinated heterosexual men due to herd protection.4 5 26 In order to observe a similar reduction in MSM, it is hypothesised that the vaccine coverage in MSM would need to reach at least 70%, which effectively protects 91% of partnerships (100% (30% by 30%)).27 Furthermore, an Australian-based mathematical model has predicted that implementing both school-based vaccination programme for boys and a targeted programme for MSM aged up to 26 years would be highly cost-effective.10 Currently, very few countries have adopted either a universal school-based HPV vaccination programme or a targeted MSM HPV vaccination programme,28 and even fewer in combination with both programmes. With the launch of a targeted HPV vaccination programme for MSM, the HPV vaccine uptake rate is at a level similar if not higher than what has been found in other studies. Two studies have shown that the HPV vaccine uptake rate was 21%17 and 17%29 among MSM aged 18–26 years in the USA. This highlights the fact that a targeted MSM programme is not sufficient to reach the critical vaccination threshold for MSM (at least 70%).10 27 In addition, regular educational training to clinicians to offer the HPV vaccine to eligible MSM would be required to increase the vaccine coverage at a clinic level. Therefore, to have a significant public health impact in the population and to be cost-effective, it is important that a targeted MSM programme is adopted in combination with a universal school-based vaccination programme.
Key messages
A time-limited free human papillomavirus (HPV) vaccination catch-up programme for men who have sex with men (MSM) aged up to 26 years has been introduced in mid-2017 in Victoria, Australia.
The HPV vaccination uptake rate among young MSM through a sexual health clinic was 42.6% between April and December 2017.
HPV vaccination uptake was significantly associated with men with a history of genital warts and who had more than four male partners in the last 12 months.
Acknowledgments
We acknowledge Afrizal Afrizal for his assistance with data extraction.
References
Footnotes
Handling editor Jackie A Cassell
Contributors EPFC contributed to the conception of this study. LM conducted the literature review, performed data analysis and wrote the first draft of the manuscript. EPFC provided statistical advice. All authors were involved in data interpretation, revised the manuscript critically for important intellectual content and approved the final version.
Funding EPFC is supported by the National Health and Medical Research Council (NHMRC) Early Career Fellowship (1091226).
Competing interests EPFC has received educational grants from Seqirus Australia to assist with education, training and for academic purposes in the area of HPV. EPFC has received travel grants from Seqirus Australia, presenting the finding from this study at the 16th Public Health Association of Australia (PHAA) National Immunisation Conference in Adelaide, Australia. EPFC has been the principal investigator on Merck Investigator Initiated Studies and received funding to conduct HPV studies. CKF has received honoraria from CSL Biotherapies and Merck, and research funding from CSL Biotherapies. CKF owns shares in CSL Biotherapies. CKF, MYC and CSB have been investigators for investigator-initiated research grants from Merck Sharp & Dohme.
Patient consent Not required.
Ethics approval Ethical approval was obtained from the Alfred Hospital Ethics Committee, Melbourne, Australia (project number 542/17).
Provenance and peer review Not commissioned; externally peer reviewed.