Article Text

Abstract
Objectives To assess the effectiveness of an internet-accessed STI (e-STI) testing and results service on testing uptake among young adults (16–30 years) who have never tested for STIs in London, England.
Methods We conducted secondary analyses on data from a randomised controlled trial. In the trial, participants were randomly allocated to receive a text message with the web link of an e-STI testing and results service (intervention group) or a text message with the link of a website listing the locations, contact details and websites of seven local sexual health clinics (control group). We analysed a subsample of 528 trial participants who reported never testing for STIs at baseline. Outcomes were self-reported STI testing at 6 weeks, verified by patient record checks, and time from randomisation to completion of an STI test.
Results Uptake of STI testing among ‘never testers’ almost doubled. At 6 weeks, 45.3% of the intervention completed at least one test (chlamydia, gonorrhoea, syphilis and HIV), compared with 24.1% of the control (relative risk [RR] 1.88, 95% CI 1.47 to 2.40, p<0.001). For chlamydia and gonorrhoea testing combined, uptake was 44.3% in the intervention versus 24.1% in controls (RR 1.84, 95% CI 1.44 to 2.36, p<0.001). The intervention reduced time to any STI test (restricted mean survival time: 29.0 days vs 36.3 days, p<0.001) at a time horizon of 42 days.
Conclusions e-STI testing increased uptake of STI testing and reduced time to test among a young population of ‘never testers’ recruited in community settings. Although encouraging, questions remain on how best to manage the additional demand generated by e-STI testing in a challenging funding environment. Larger studies are required to assess the effects later in the cascade of care, including STI diagnoses and cases treated.
- testing
- diagnosis
- service delivery
- programme evaluation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Testing coverage for STIs remains suboptimal in England. The National Chlamydia Screening Programme (NCSP) encourages sexually active young adults (15–24 years) to test annually for chlamydia and on change of sexual partner. Yet in 2017, only 20% of local authorities reached the recommended chlamydia detection rate of at least 2300 diagnoses per 100 000 population of individuals aged 15–24 years.1
Both psychosocial and contextual factors inhibit the use of face-to-face sexual health services.2 3 Online sexual health services, including internet-accessed STI (e-STI) testing, may overcome some of these barriers by enabling users to bypass the stigma, embarrassment and inconvenience associated with face-to-face care.4–7 Typically, e-STI testing requires users to order postal self-sampling kits online, collect their own samples, return samples to a laboratory and be notified of their results by short message service text message or telephone.8 9
Public Health England recommends e-STI testing to expand access to opportunistic screening for chlamydia, particularly young adults who struggle to access conventional services, including young men and those in rural areas.9 Yet the evidence on the effectiveness of e-STI testing to increase testing uptake among those who do not use face-to-face STI testing pathways is extremely limited.
One randomised controlled trial (RCT) conducted with individuals aged 18–24 years in France provided data to suggest that among those who had never previously screened for chlamydia, a higher proportion of the intervention group (e-STI testing) completed a chlamydia test (28.2%, 1257/4453), compared with the control group allocated to usual care (7.5%, 331/4431). However, outcomes were assessed differently in the control and intervention arms, and it is not known whether participants tested for other STIs prior to the study.10
In 2015, we completed a large RCT in Lambeth and Southwark—two London boroughs with extremely high rates of STIs relative to London and the rest of England.11 We found that e-STI testing increased uptake of testing at 6 weeks among a young population (16–30 years), when offered in community settings and delivered alongside usual care (50.0% vs 26.6%, relative risk 1.87, 95% CI 1.63 to 2.15, p<0.001).12 Here we examine the effect of e-STI testing on uptake of any STI test, uptake of chlamydia and gonorrhoea tests and time to test, among a subsample of trial participants who reported never having tested for an STI at baseline. In view of the distinct policy context and barriers associated with the provision of routine HIV testing outwith specialist settings in the UK, we will report results for uptake of serological testing (including HIV) separately.
Methods
Study design
The trial procedures are described in detail elsewhere.12 Briefly, participants were recruited in community settings. The study was promoted alongside a health promotion message to encourage STI testing. Young people aged 16 –30 years of age, resident in the London boroughs of Lambeth and Southwark, sexually active (at least one sexual partner in the last 12 months), stated willingness to take an STI test and with access to the internet were eligible for inclusion.
At randomisation, participants in the intervention group were sent a text message with the uniform resource locator (URL) of SH:24 (www.sh24.org.uk). SH:24 offered free postal self-sampling test kits for chlamydia, gonorrhoea, HIV and syphilis. Chlamydia, gonorrhoea and syphilis test results were delivered by text message. Participants with reactive results for syphilis or positive results for chlamydia and gonorrhoea were signposted to local clinics for confirmatory testing and treatment as required. Reactive results for HIV were communicated by phone by a clinician. Non-returners of test kits were sent a text message reminder at 2 weeks. Additional information on the tests kits and procedures is provided in online supplementary file 1.
Supplemental material
Participants in the control arm were sent the URL of a bespoke website with the contact details, websites and location (google map image) of seven sexual health clinics in Lambeth and Southwark. All participants were free to use any other services or interventions.
At 6 weeks, we collected self-reported data online or via a postal questionnaire. We obtained objective measures for our endpoints (uptake of STI testing, cases diagnosed and cases treated) by searching the SH:24 database and patient record databases at Hospital Trusts in Lambeth and Southwark for all participants. If participants reported using another service (general practitioner (GP) surgery or sexual health service outside the boroughs), we contacted the service to collect STI testing, diagnosis and treatment data.
In these secondary analyses, we analysed a subsample (n=528) of the main trial sample (n=2063) who reported never having had an STI test at baseline. Our outcomes are: (1) the proportion of participants who tested for any STI at 6 weeks from randomisation and (2) time from randomisation to completion of an STI test in each arm. In addition, we assessed the proportion of participants who tested for chlamydia and gonorrhoea (combined) at 6 weeks.
The process outcomes are the proportion who tested positive for any STI among participants who completed a test within 6 weeks; the proportion of participants who completed an STI test by service type; and the proportion who consider the intervention to be acceptable (intervention group only).
Statistical methods
In the main trial, 50.0% of the intervention group completed an STI test compared with 26.6% in the control group (RR 1.87, 95% CI 1.63 to 2.15, p<0.001).12 We hypothesised that in this subpopulation, far fewer participants would complete an STI test in each arm but that the relative effect of e-STI testing on testing uptake would be similar. We assumed that 28% of the intervention group would complete a test compared with 15% in the control group. A sample size of 420 would lead to 90% power (two-side alpha=5%) to detect a relative risk of 1.87.
We adopted a similar statistical approach to the main trial analyses for comparability. Randomisation was based on minimisation, which required an adjusted analysis to account for variables included in the algorithm.13 To obtain more precise estimates and CIs with the correct coverage, our analysis models used an inverse probability of treatment estimator to estimate the average treatment effect (ATE). In these models, the ATE is expressed as the weighted risk difference. Covariates included all minimisation factors (gender, age, sexual orientation and number of sexual partners in the last 12 months) in addition to ethnicity, as this is also a predictor of the outcome.14 Estimates for the weighted risk ratio and their 95% CIs were obtained via the delta method of transformation.
To account for missing outcome data, we used multivariate imputation by chained equations assuming data are missing at random (MAR). We imputed our two outcomes: (1) any STI test, (2) chlamydia and gonorrhoea tests, using two separate models. Each imputation model conditioned on self-reported testing and self-reported diagnoses, which were also incomplete. We included randomised group as a covariate, which was weighted by the inverse of the propensity score to ensure compatibility with our models for analysis. We generated 100 imputed datasets for each outcome, and inference proceeded via Rubin’s rules.15
All baseline characteristics were fully observed, except for sexual orientation. A missing category was therefore used. In the main trial, a sensitivity analysis was conducted to explore departures from MAR for our coprimary outcomes of STI testing and STI diagnoses. The results were similar to the estimates under MAR for all the scenarios we investigated.12 For the purposes of these secondary analyses, we considered our assumption that data are MAR to be valid.
To explore heterogeneity of the intervention effect on our outcome, we tested for interaction at a 5% level of significance to assess whether effectiveness varied by the following baseline characteristics: gender (male, female); ethnicity (white, black/African/Caribbean/black British, Asian/Asian British/all other groups); age (16-19, 20–24, 25–30 years); number of sexual partners in the last 12 months (1, 2+), sexual orientation (men who have sex with men (MSM), other); index of multiple deprivation (linear) and recruitment source (face-to-face, online, other). These analyses were conducted in the complete cases under a MAR assumption using a log binomial model.
We used survival analysis to estimate the restricted mean survival time (RMST) from randomisation to completion of an STI test for each group. The RMST is a measure of average survival from baseline to a specified time point and corresponds to the area under the survival curve up to that point.16 We set the time horizons to t*=6 weeks (42 days), t*=2 weeks (14 days) and t*=one week (7 days) to investigate possible time dependency of the intervention among this subsample. We accounted for covariates by weighting on the inverse of the estimated propensity score.
All analyses were performed using Stata V.15.1 and R Studio V.3.5.0.
Results
Outcome data (STI testing) were available for 87% (213/244) of the intervention group and 79% (224/284) of the control group.
Baseline characteristics are presented in table 1.
Baseline characteristics of participants
Supplemental material
At 6 weeks, 45.3% of the intervention completed at least one STI test, compared with 24.1% of the control group (RR 1.88, 95% CI 1.47 to 2.40, p<0.001). For chlamydia and gonorrhoea testing combined, 44.3% completed a test in the intervention compared with 24.1% in the control (RR 1.84, 95% CI 1.44 to 2.36, p<0.001) (table 2).
Effect of the intervention on testing uptake at 6 weeks
Supplemental material
In the complete cases, the intervention reduced time to test for any STI at 42 days. A very small difference was observed at 14 days but no difference at 7 days (table 3).
Time to test (any STI)
The intervention was more effective in those recruited via face-to-face settings, compared with those recruited online or via other methods (eg, print media). No heterogeneity was observed across any other subgroups (figure 1).
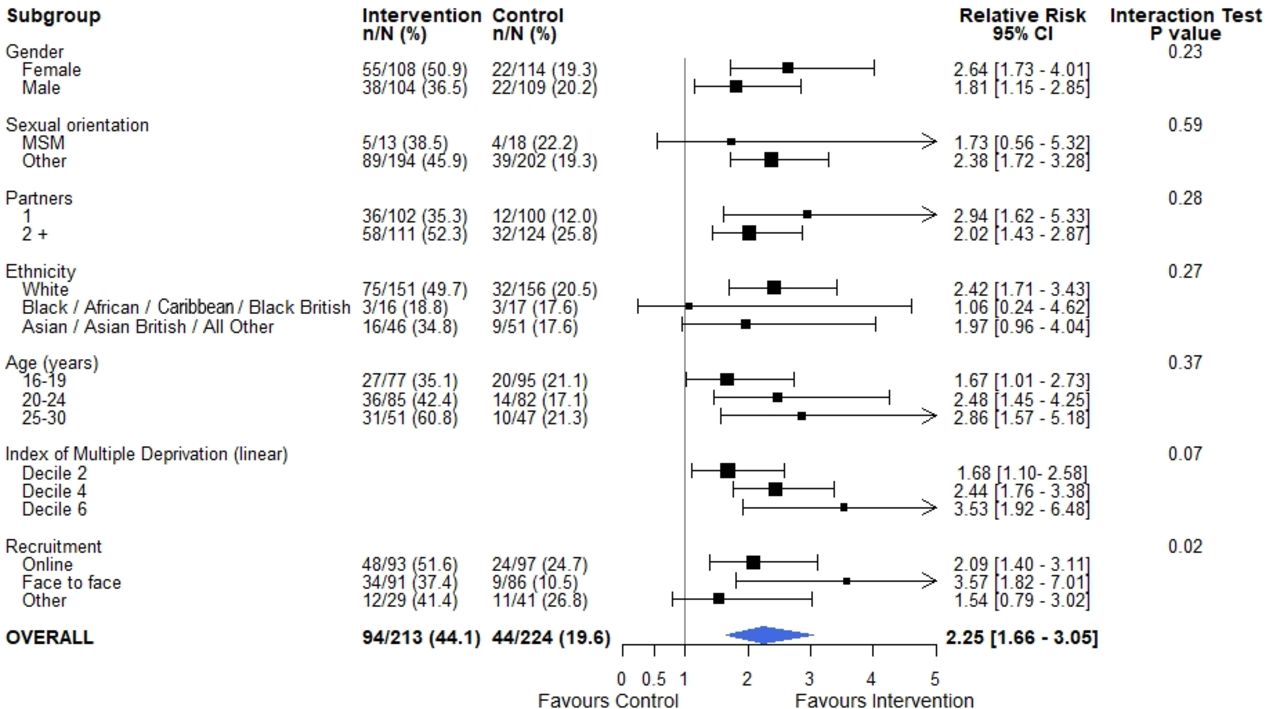
{kind=link}
Effect of the intervention on STI testing uptake by subgroup.
Process outcomes
Among those who completed a test, 4.3% (4/94) of the intervention arm tested positive for an STI, compared with 2.3% (1/44) in the control. A percentage of 89.4 (84/94) of those who tested in the intervention arm tested via SH:24 (online supplementary file 4). A percentage of 75.0 (63/84) of the intervention arm who tested via SH:24 provided data on acceptability. Of those 74.6% (47/63) deemed the SH:24 pathway to be acceptable.
Supplemental material
Discussion
Statement of principal findings
When promoted in community settings and delivered alongside usual care, e-STI testing increases testing uptake among individuals who have never tested for STIs. Similar estimates were observed when we examined the effects on uptake of testing for chlamydia and gonorrhoea. The intervention reduced time to test.
Strengths and weaknesses
The strengths of the main trial have been discussed elsewhere.12 In these secondary analyses, the outcomes of uptake of any STI test, and uptake of chlamydia and gonorrhoea testing combined, were known for 83% of participants. We collected objective outcome data including for those participants who tested outside of Lambeth and Southwark or via an alternative care pathway (eg, at their GP). Our subsample of ‘never testers’ included priority groups for STI prevention: 80% (420/528) were young adults between 16 years and 24 years and 7% (35/528) were MSM. In addition, over half (294/528) reported having at least two sexual partners in the last 12 months.
Secondary analyses of RCT data are recommended to generate additional insights beyond the primary research question and to make efficient use of trial datasets.17 18 We specified our hypotheses and obtained ethical approval prior to conducting these analyses, and we had sufficient power to detect intervention effects on STI testing uptake. Selecting a subsample of randomised participants for secondary analyses can introduce baseline imbalances. Our adjusted analyses, based on inverse probability of treatment weighting, accounted for possible imbalances across key prognostic factors.
Our study has several limitations. It was not possible to assess outcomes later in the cascade of care such as STI diagnoses and STI cases treated due to insufficient power. Nevertheless, undiagnosed infections were detected in this subpopulation. Of those who tested, 4.3% (4/94) in the intervention arm and 2.3% (1/44) in the control arm were diagnosed with an STI. Four participants were diagnosed with chlamydia and one with gonorrhoea. This underlines the importance of public health strategies to reach populations who do not use conventional services.
Our subgroup analysis suggests that the effect of the intervention was greater among those recruited in face-to-face settings. A lower proportion of control participants recruited in face-to-face settings accepted the offer a test, compared with those recruited elsewhere. It is plausible that those recruited in face-to-face settings, such as further education colleges, had greater exposure to campaigns encouraging clinic-based testing and were therefore more ambivalent towards the offer of a test in a face-to-face setting. However, these analyses were exploratory and further research is warranted.
Meaning and mechanisms
To our knowledge, this is the first study to assess the effectiveness of an e-STI testing service offered to young adults who had never previously tested for STIs.
Our findings may have implications for the way e-STI testing is promoted in routine settings. In 2017, only 10.1% of all chlamydia tests in England were conducted via internet-accessed services.1 This may be indicative of patient preference, low availability of e-STI testing in some settings or data quality. It is also plausible that young people lack awareness of online care pathways. In our study, all intervention participants were sent the web link of SH:24 via text message. Text messaging is an effective medium for sexual health promotion19 and could be used to promote e-STI testing in routine care.
The effect estimate for STI testing (relative risk) is comparable in magnitude to the effect size from the main trial analyses, and this was expected. The proportions of participants who completed a test in each arm are also comparable, but this was not anticipated. We had assumed that this subsample of ‘never testers’ would be more reluctant to accept the offer of a test. Our recruitment strategy, which included a health message to promote regular STI testing, may offer insights for interventions that aim to increase demand for testing in community settings.
The number of chlamydia cases (n=4) were too few to assess care pathways for those diagnosed by online and clinic services in this study. Results from a preliminary observational evaluation of an eSexual health clinic—offering web-based results, risk management and remote treatment for chlamydia via pharmacy collection—suggest that online treatment pathways are feasible for users of e-STI testing services.20
In the intervention arm, 4.3% of completed chlamydia tests were positive. In routine settings, 9% of internet-accessed chlamydia tests reported to the NCSP were positive in 2017.1 In our study, those who chose to participate, and complete a test via SH:24, may have practised lower risk behaviours than young people who use e-STI testing in routine care. Despite this lower test positivity, it is encouraging that the intervention increased chlamydia testing among a sexually active population who were either eligible (<25 years) or recently eligible (25–30 years) for opportunistic chlamydia screening but had never tested for chlamydia (or other STIs) in their lifetime.
The effect of the intervention is time dependent. There was a reduction in time to test at time horizons of 42 days but little or no difference at 14 and 7 days. While most participants in the intervention arm ordered the kits almost immediately after randomisation, they delayed in returning the kits to the laboratory (median time from kit order to kit return=9 days (IQR 7–13.5)). SH:24 sent reminder text messages at 2 weeks to all non-returners. Future iterations of e-STI testing services could reduce delays on the care pathway by sending earlier and more frequent reminders.
The barriers to seeking sexual healthcare are multifaceted and operate at individual and structural levels.2 21 It is encouraging that in the trial sample, those who tested previously were more likely to report multiple sexual partners in the past year and to identify as MSM, compared with never testers (online supplementary file 2). Higher proportions of never testers were male, of Asian or Asian British ethnicity and younger age (16–19 years), which is in line with other studies that have reported barriers to service use among these groups.9 22 23
Importantly, over half (~54%) of the intervention group did not complete a test, which suggests that e-health services do not circumvent all obstacles associated with face-to-face care. Further research is needed to understand the precise mechanism of change among this subpopulation of never testers and to identify persistent barriers to testing.
For some first-time testers, e-STI testing services may become their preferred point of contact with the sexual healthcare system. This presents commissioners and providers with the challenge of ensuring that the package of care attainable via face-to-face and online entry points is comparable. For young adults, this should include comprehensive sexual health information, safeguarding, access to condoms, contraception and signposting to additional services as required.24 Much will depend on the integration that can be achieved between online and face-to-face clinical pathways. This includes the capacity of online providers to identify vulnerable users and those with complex health needs and to oversee their transition to face-to-face care.6 25
e-STI testing was initially positioned within a normative agenda to expand access to health services.4 In the wake of cuts to sexual health funding in England, e-STI testing is increasingly viewed as a means to meet existing demand for STI testing at reduced cost.26 27 In London, many genitourinary medicine clinics divert asymptomatic patients to online care, prioritising scarce resources for more complex cases. Yet, consistent with the findings of this study, and the main RCT,12 a study based on routine data found that the introduction of SH:24 increased basic STI testing activity across the whole system in Lambeth and Southwark.28 Meeting additional demand is challenging in this current funding climate, and has resulted in a daily cap on online orders in some areas.
The impact of demand management strategies on young adults seeking sexual healthcare in either face-to-face or online service environments remains unknown. Online services may not be appropriate for all asymptomatic cases, and some patients require additional support to use e-STI testing.28 Careful monitoring is required to determine if the benefits of e-STI testing observed in our research translate into similar benefits in routine settings.
Conclusions
This study has demonstrated that e-STI testing, delivered alongside usual care, can increase STI testing uptake and reduce time-to-test among a young population of ‘never testers’ recruited in community settings.
The findings lend weight to national guidance, which recommends e-STI testing as a measure to expand access to opportunistic chlamydia screening. Yet questions remain on how best to manage the additional demand generated by e-STI testing in a challenging funding environment. e-STI testing services can be delivered to scale as demonstrated by SH:24 and other national online providers. e-STI testing requires ongoing monitoring and evaluation. Larger studies are needed to assess outcomes later in the cascade of care such as STI diagnoses and cases treated.29
Key messages
Internet-accessed STI (e-STI) testing is an effective measure to increase uptake of STI testing, including chlamydia testing, among young people who do not use conventional services
The effect of e-STI testing on outcomes later in the cascade of care including cases diagnosed and treated requires further evaluation
In this current funding environment, questions remain on how best to manage the additional demand generated by e-STI testing
Acknowledgments
We are very grateful to Kate Folkard (Public Health England) for insightful comments on earlier drafts of the manuscript. We also thank Dr Tim Morris for advice on the statistical methods. We thank Jonathan Syred for his support in the management of the randomised controlled trial. We thank all the participants who took part in the study. We are very grateful to Lambeth College, Lewisham Southwark College, London Southbank University, Camberwell College of Arts, London College of Communications, Goldsmiths University, City and Islington College, and Kings College London for their support during recruitment. We also thank all the individuals and organisations that promoted the trial among their networks: Miranda Young and Nick Batley (KCLSexpression), Susy Langsdale (Brook Young People), Emma Corker, Lorraine Baker, Deirdre Love (Southwark Council), Constantia Pennie (SHAKA services) and Chitra de Caires (Healthwatch Southwark). We would like to thank Robert DeLuca (Kings College Hospital NHS Foundation Trust) and MatthewCraven and Zeenat Kazi (Guy's and St Thomas' NHS Foundation Trust) for providing us with data. We would like to thank the following NHS trusts for their assistance in providing follow-up data: Chelsea and Westminster Hospital NHS Foundation Trust, Barts Health NHS Trust, Central and North West London NHS Foundation Trust, London North West Healthcare NHS Trust, Imperial College Healthcare NHS Trust, Croydon Health Services NHS Trust, Epsom and St. Helier University Hospitals NHS Trust and St. George's University Hospitals NHS FoundationTrust. We would like to thank the Residents Advisory Group from Lambeth and Southwark for its support in reviewing the study documentation and procedures. We would also like to thank Brook Young People and the many general practitioner surgeries in London that conducted patient record checks. We thank the Trial Steering Committee: Dr Catherine Lowndes (chair), Dr Sarah Woodhall, Dr Andrew Copas, Dr Nigel Field, Dr Christopher McKevitt, Dr Katy Turner and Dr Katherine Looker. Research assistants: Laura Parry-Billings, Shannon Williams, Harriet Pittaway, Mathilde Duquesnel, Phoebe Whitehouse, Yvonne Adebola and Holly Farler. Trial database and randomisation system: Irrfan Ahamed. Recruitment and trial promotion: Samantha Tedeshi, Oliver Glave, Joshua Garfield, Jacob Laurent-Farmer, Miranda Young, Nick Batley, Rasheeda Russell, Megan Pickering, Amani Alam, Hanna Qureshi, Hasan Taner, Layla Ismail, Mehanaz Shamie Alom, Ugne Ratkute, Muna Esmail and Paula Demeterova. Intervention development: the SH:24 online service was developed with a grant from Guy's and St Thomas' Charity. We would like to acknowledge the contributions of the whole SH:24 team and in particular Gillian Holdsworth, Chris Howroyd and Glyn Parry, who led the development of this innovative online sexual health service. SH:24 team: Gillian Holdsworth (managing director), Chris Howroyd, Glyn Parry, Andre Marty, Vicki Spencer-Hughes, Molly Courtenay, Sarah Cox, Dr Michael Brady and Dr Anatole Menon-Johansson.
Footnotes
PB and CF are joint senior authors.
Handling editor Sevgi O Aral
Contributors EW, PB and CF conceptualised the study. EW conducted the statistical analyses with guidance and supervision from CL. EW wrote the first draft of the manuscript. CL, PB and CF reviewed and commented on drafts of the manuscript. All authors approved the final version. PB secured funding for the project. PB and CF are both senior authors on this work. EW had full access to the data and had final responsibility for the decision to submit for publication.
Funding This study was funded by Guy's and St. Thomas' Charity, grant number: MAJ120505. PB secured the funding for this work.
Competing interests EW reports receiving a PhD studentship from Guy’s and St Thomas’ Charity via SH:24 (a not-for-profit community interest company). PB report grants from Guy’s and St Thomas’ charity via SH:24 (a not-for-profit community interest company) during the conduct of the study. CF reports receiving funding for her time from Guy’s and St Thomas’ Charity paid via SH:24 (a not-for-profit community interest company). PB is a director of SH:24 (a not-for-profit community interest company).
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.