Article Text

Abstract
Objective In 2017, there was an outbreak of invasive meningococcal disease (IMD) serogroup C among men who have sex with men (MSM) in Victoria, Australia. A government-funded free meningococcal (MenACWY) vaccination programme targeting all MSM living in Victoria was launched between December 2017 and December 2018. The aim of this study was to examine the vaccine uptake among MSM attending a sexual health clinic in Melbourne.
Methods This was a retrospective clinical audit of MSM attending the Melbourne Sexual Health Centre (MSHC) during the vaccination programme. We calculated the proportion of MSM who received the meningococcal vaccine on their first visit and at any time during the programme. We performed univariable and multivariable logistic regression to identify the factors associated with the vaccine uptake on the first visit.
Results Of the 10 370 MSM who attended MSHC, 55.5% received the vaccine on their first visit and 67.4% at any time during the programme. MSM had higher odds of receiving the vaccine on the first visit if they were aged 16–25 years (adjusted OR (aOR) 1.21; 95% CI 1.08 to 1.35) or 26–35 years (aOR 1.17; 95% CI 1.07 to 1.29) in comparison with MSM older than 35 years; were HIV-negative and not on pre-exposure prophylaxis (aOR 1.80; 95% CI 1.56 to 2.09); had more than four male partners in the last 12 months (aOR 1.16; 95% CI 1.06 to 1.27); had male partners only (aOR 2.24; 95% CI 1.96 to 2.55); or were born overseas (aOR 1.11; 95% CI 1.03 to 1.21).
Conclusions Two-thirds of the MSM attending a sexual health clinic received at least one dose of meningococcal vaccine. The vaccination programme coincided temporally with a dramatic reduction in the incidence of IMD. Vaccination should be further promoted among MSM and men who have sex with both men and women.
- vaccination
- gay men
- sexual behaviour
- vaccines
Statistics from Altmetric.com
Introduction
Invasive meningococcal disease (IMD) is fatal in around 10%–15% of cases and results in permanent disability in up to 20% of those who survive.1 IMD is caused by Neisseria meningitidis, which is carried asymptomatically in the nasopharynx and can be transmitted through respiratory droplets or direct contact with throat secretions.1 2
There are 13 meningococcal serogroups, of which serogroup B and more recently serogroup W account for most IMD cases in Australia. Serogroups C and Y are responsible for a smaller number of cases. Although IMD outbreaks occur, most cases are sporadic. The overall incidence of IMD in Australia declined substantially from 3.5 per 100 000 persons in 2001 to 0.6 per 100 000 in 2013. In recent years, there has been an increase in reported cases, peaking at 1.5 per 100 000, the highest rate since 2007.3
Since 2001, several outbreaks of IMD caused by serogroup C have been reported worldwide among men who have sex with men (MSM). The outbreaks occurred in metropolitan areas in Europe and North America, and health authorities responded by recommending vaccination either among all MSM in the area or among MSM with certain risk factors.4–10 Close and intimate contact with multiple partners, being HIV-positive, regularly visiting crowded venues, sharing cigarettes or recreational drug use were risk factors identified among MSM for being diagnosed with IMD.10 11
In response to an outbreak of IMD caused by serogroup C among MSM in 2017, the Victorian Government Department of Health and Human Services funded a time-limited vaccination programme for MenACWY (Menactra, Sanofi) between 11 December 2017 and 31 December 2018. All MSM residing in Victoria were eligible to receive the MenACWY vaccine for free through sexual health clinics, general practice clinics and other registered immunisation providers.12 The recommendation was a single MenACWY dose for HIV-negative MSM, with two doses 8–12 weeks apart for HIV-positive MSM. During this period, 26 011 doses of Menactra were distributed across Victoria through this free vaccination programme (S Pellissier, personal communication).13 The aim of this study was to examine the MenACWY vaccine uptake rate and factors associated with vaccination uptake on the first visit among MSM attending a sexual health clinic in Melbourne.
Methods
MSM aged 16 years and older attending the Melbourne Sexual Health Centre (MSHC) between 11 December 2017 and 31 December 2018 were included in this analysis. MSHC is the largest public health service in the state of Victoria, Australia. MSHC provides about 50 000 consultations per year; 40% of these clients are MSM. MSHC also provides specialist care in HIV with a designated HIV clinic.14 All clients are invited to complete a series of questions on arrival using computer-assisted self-interview (CASI). Data including demographic characteristics (eg, age, indigenous origin, country of birth), sexual history (eg, sex work, number of male and female partners, condom use with male sex partners during anal sex in the last 12 months), HIV status, current use of pre-exposure prophylaxis (PrEP) for HIV and use of intravenous drugs in the last 12 months are collected using CASI. Missing data were categorised into the ‘unknown/missing’ category.
All clinicians at MSHC were aware of the free MenACWY vaccine and were asked to offer it to all MSM during the vaccination programme. Reminders and updates were provided throughout the period. Informative posters and flyers were placed in the waiting room and some clinic rooms.
The frequency and proportion of MSM who received the vaccine on their first visit during the study period were calculated. For those who did not receive the vaccination on their first visit, we also examined whether these men received the vaccine at any visit during the period. HIV-positive MSM were advised to have two doses of the vaccine, and we examined the proportion of HIV-positive MSM who received two doses of the vaccine. Age was categorised into three groups (16–25, 26–35, and 36 years and above) in this analysis. We further compared the vaccine uptake rate between MSM aged 16–20 years and MSM aged 21–25 years because some men aged 16–20 years would have been eligible for the free adolescent MenACWY vaccination programme in Victoria launched since mid-2017.15
Univariable and multivariable logistic regression models were performed to identify the factors associated with the MenACWY vaccine uptake on the first visit during the study period. In the multivariable analysis, we fitted the model with all variables, and then excluded (stepwise backward) the variables with a p value of >0.2. The 0.05 level was used for statistical significance in the multivariable logistic regression model. We used the Hosmer-Lemeshow test to assess the goodness of fit of the logistic regression model. All statistical analyses were conducted using SPSS V.25.
Results
There were 10 370 individual MSM who attended MSHC at least once between 11 December 2017 and 31 December 2018. The median number of visits per person was 2 (interquartile range (IQR): 1–4). The median age was 31 years (IQR: 26–39). Almost half of the MSM (48.7%, n=5048) were born in Australia and a small proportion (0.9%, n=98) were Aboriginal or Torres Strait Islander. The majority of MSM (88.8%, n=9213) had sex with male partners only, but 11.2% (n=1157) had sex with both male and female partners. Half of the MSM (50.8%, n=5185) had more than four male partners in the last 12 months. A small proportion of MSM injected drugs in the last 12 months (2.4%, n=247) and had ever worked as a sex worker (2.5%, n=256). There were 1268 (12.2%) HIV-positive MSM. Of the 9102 HIV-negative MSM, 10.7% (n=976) were taking PrEP (table 1).
Baseline characteristics of 10 370 men who have sex with men attending the Melbourne Sexual Health Centre from 11 December 2017 to 31 December 2018
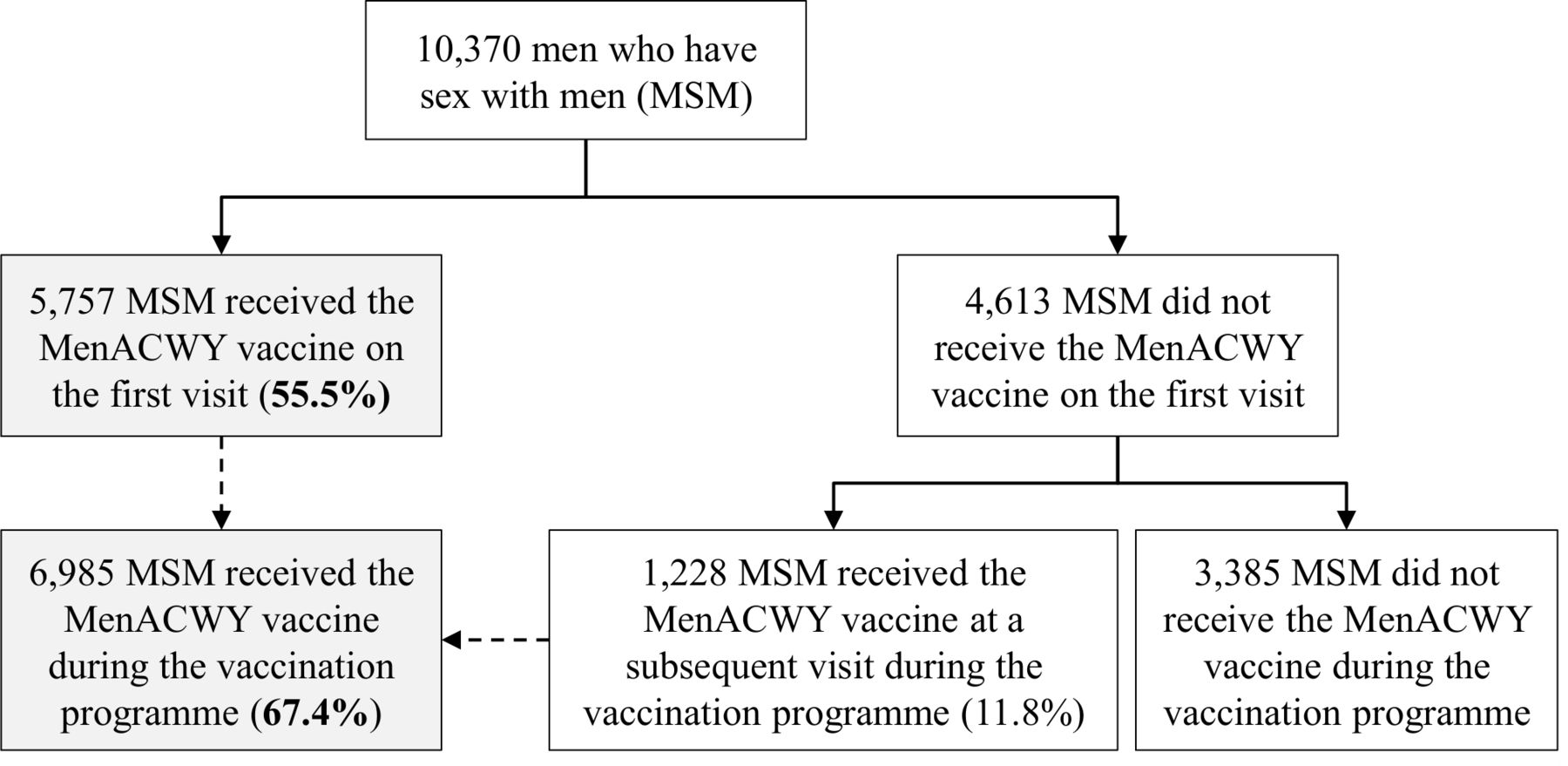
Of the 10 370 MSM who attended MSHC during the study period, 5757 (55.5%; 95% CI 54.6% to 56.5%) received the free MenACWY vaccine on their first visit. Of the 4613 MSM who did not receive the vaccine on the first visit, 1228 men received the vaccine at a subsequent visit during the study period. Therefore, a total of 6985 (67.4%; 95% CI 66.5% to 68.3%) MSM had received at least one dose of MenACWY at any time during the programme (figure 1). Among the 1268 HIV-positive MSM, 587 (46.3%; 95% CI 43.6% to 49.0%) received the vaccine on the first visit and 894 (70.5%; 95% CI 67.9% to 73.0%) received at least one dose at any time during the study period, and of them 633 (49.9%; 95% CI 47.2% to 52.7%) received two doses. Overall, there were 7618 doses of MenACWY vaccine administered at MSHC.

{kind=link}
Men who have sex with men who attended the Melbourne Sexual Health Centre (MSHC) during the meningococcal conjugate vaccination (MenACWY) programme between December 2017 and December 2018.
Table 2 suggests that younger MSM had higher odds of receiving MenACWY vaccine on their first visit (adjusted OR (aOR) 1.21 (95% CI 1.08 to 1.35) in MSM aged 16–25 years old and aOR 1.17 (95% CI 1.07 to 1.29) in MSM aged 26–35; in comparison with those aged 36 years or above). Nevertheless, in the 16–25 years age group, MSM aged 16–20 years had a significantly lower vaccine uptake rate compared with MSM aged 21–25 years on the first visit (46.7% vs 61.4%; p<0.001). MSM who had more than four male partners had higher odds of receiving the vaccine (aOR 1.16; 95% CI 1.06 to 1.27) than MSM who had four or less male partners in the last 12 months. Overseas-born MSM also had higher odds of receiving the vaccine than Australian-born MSM (aOR 1.11; 95% CI 1.03 to 1.21). Aboriginal or Torres Strait Islander status was not associated with the vaccination uptake rate. MSM who injected drugs in the last 12 months had lower odds of receiving the vaccine in the univariable analysis (OR 0.74; 95% CI 0.57 to 0.95); however, injecting drug use becomes statistically insignificant in the multivariable analysis after adjusting for age, country of birth, sexual practice, number of male sex partners and HIV/PrEP status. MSM who had male partners only in the last 12 months had higher odds of receiving MenACWY vaccine compared with MSM who had both male and female partners (aOR 2.24; 95% CI 1.96 to 2.55). HIV-negative MSM not taking PrEP also had higher odds of receiving MenACWY vaccine compared with HIV-positive MSM (aOR 1.80; 95% CI 1.56 to 2.09). The odds of receiving the MenACWY vaccine were similar among HIV-positive MSM and HIV-negative MSM on PrEP (aOR 0.94; 95% CI 0.79 to 1.11). Condomless anal sex in the last 12 months and being a sex worker were not associated with the MenACWY vaccine uptake in the univariable analysis.
Factors associated with meningococcal conjugate vaccine (MenACWY) uptake on the first visit among 10 370 men who have sex with men attending the Melbourne Sexual Health Centre from 11 December 2017 to 31 December 2018
Discussion
This study shows that more than two-thirds of MSM attending MSHC had received the free MenACWY vaccine by the end of 2018 from the time-limited, government-funded meningococcal vaccination programme in Victoria. The vaccination programme coincided temporally with a dramatic reduction in IMD cases in MSM from seven cases in 2017 to one case in 2018.16 Younger MSM, MSM with more than four male sex partners in the last 12 months, HIV-negative MSM not on PrEP, MSM with male partners only and those born overseas had higher odds of receiving the MenACWY vaccine.
Health authorities in different countries have also implemented vaccination programmes in response to IMD outbreaks in MSM that were tailored to local outbreak epidemiology. In some places such as Toronto (2001), New York (2012), Paris (2014) and Chicago (2015), free vaccination was provided for MSM with specific risk behaviours or characteristics (eg, being older than 24 years old, frequenting social gay venues, HIV-positive MSM, having more than one male sexual partner or using online dating apps for seeking sexual partners).4 8 17 18 However, in some other places such as Berlin (2013), Southern California (2016) and Victoria (2017), vaccination was recommended to all MSM regardless of risk factors.9 12 19
The vaccination coverage required to prevent IMD in MSM is unknown. At present, two studies have assessed the uptake rate during outbreaks in MSM. First, in Berlin in 2013, following five IMD cases in MSM, a vaccination campaign was initiated providing free MenACWY vaccination to HIV-positive MSM; others had to request reimbursement or pay out of pocket. An internet-based survey revealed 60% of MSM were aware of the vaccination recommendation, but only 23.3% received the vaccine, and HIV-positive MSM had higher odds of receiving the vaccine.19 Second, in Southern California in 2016, after an outbreak of 31 cases with the majority of MSM, MenACWY vaccine was provided free of charge at some clinics and community-based healthcare organisations. A venue-based survey involving clinics, community-based organisations and other venues frequented by MSM showed a vaccination uptake of 37.5%; the uptake was associated with men who were aged 30 years or older, had ever had an STI, believed MenACWY vaccination was important and knew someone who had been vaccinated.20
Our findings show that younger MSM had a higher uptake rate of the MenACWY vaccine. This is important because previous studies have shown that younger MSM are at a higher risk of acquiring meningococcal disease compared with older MSM.21 The higher rate in young MSM may relate to the observation that they are more likely to kiss than older MSM.22 23 However, we also found that MSM aged 16–20 years had the lowest uptake rate of MenACWY vaccine (46.7%) than any age group. It is possible that men in this age group would have already received the vaccine through the Victorian adolescent MenACWY vaccination programme for teenagers aged 15–19 years in mid-2017.15 This state-based adolescent MenACWY vaccination programme was then expanded to a national programme for all teenagers aged 15–19 years in April 2019.24
This is the first study to provide an estimate of the MenACWY vaccine uptake rate among MSM taking PrEP. Our data show that MSM taking PrEP had a lower uptake rate on the first visit than MSM not taking PrEP and an uptake similar to HIV-positive MSM. PrEP users are likely to have an increased risk of IMD given they have a higher number of sexual partners and frequently use illicit party drugs, and thus it is important to achieve a high uptake rate to prevent transmission within these sexual networks.25 Our study was not able to determine why it was low in this group, although it is possible that they may have received the vaccine through the healthcare provider who was prescribing their PrEP.
During the same time period, two other vaccines (ie, human papillomavirus (HPV) and hepatitis A) were also provided for free to eligible MSM as part of the government-funded vaccination programme in Victoria.26 27 Our observation that MSM with more partners were more likely to receive the MenACWY vaccine fits with previous observations at our clinic with the HPV and hepatitis A vaccine, suggesting this core group is protected against the infection within wider sexual networks to prevent ongoing transmission.26 27 Our data show that MSM who have both male and female partners were less likely to receive the MenACWY vaccine, which was consistent with the HPV vaccine uptake.26 It is possible that men who have sex with men and women may consider themselves to have a lower risk of acquiring IMD compared with men who have sex with men only, but further research will be required to confirm this.
There are several limitations to this study. First, we were unable to examine the reasons why some MSM declined to receive the MenACWY vaccine in our clinic as this information was not routinely collected. It is possible, for example, that some MSM attending MSHC had received the vaccine elsewhere, and hence our study may have underestimated the proportion vaccinated. Second, this study was conducted at a single sexual health clinic in an urban setting. It is likely that MSM attending a sexual health clinic are more sexually active and have better knowledge and awareness of sexual health, and hence would be more likely to be vaccinated. However, our estimate is likely to be roughly correct given that 26 000 doses were distributed to a Victorian MSM population of about 45 000 individuals, notwithstanding that some of the MSM in Victoria have HIV and would have received two doses.28 Third, it is noted that MSM who declined to report their sexual or drug use practices generally have a lower vaccination coverage. We were unable to investigate the characteristics among these men due to limited data; however, previous studies have shown that MSM who declined to report the number of sexual partners using CASI are at a higher risk of HIV/STI.29 Thus, this group of MSM might have lower knowledge and awareness of sexual health and vaccination.
In conclusion, an outbreak of IMD in Victoria, Australia caused by meningococcus serogroup C led to a time-limited, publicly funded MenACWY vaccination campaign. Two-thirds of MSM attending a sexual health clinic received vaccination, but specific subgroups had lower levels of vaccination at the clinic, including MSM with both male and female partners, HIV-positive MSM and MSM on PrEP. Further study will be required to understand the transmission dynamics of N. meningitidis among MSM to identify important risk factors. Men who have sex with both men and women may act as a bridge of transmission from MSM to heterosexuals, and our data suggest that it is important to increase the vaccination uptake rate among this population. Likewise, awareness should be reinforced to provide prompt vaccination to HIV-positive MSM and MSM on PrEP, given that these groups could have an increased risk of IMD.
Key messages
An outbreak of invasive meningococcal disease (IMD) serogroup C among men who have sex with men (MSM) was identified in 2017 in Victoria, Australia.
A government-funded, time-limited, free meningococcal vaccination programme targeting all MSM living in Victoria was launched between December 2017 and December 2018 in response to the outbreak of IMD among MSM.
The meningococcal MenACWY vaccine uptake rate among MSM attending a sexual health clinic in Melbourne was 67.4% between December 2017 and December 2018.
The vaccination programme coincided temporally with a dramatic reduction in the incidence of IMD among MSM (from seven cases in 2017 to one case in 2018) in Victoria.
Acknowledgments
We acknowledge Afrizal Afrizal at Melbourne Sexual Health Centre for his assistance with data extraction. We would like to thank Stephen Pellissier and Janet Strachan at the Victorian Department of Health and Human Services for providing the number of Menactra vaccines and the number of invasive meningococcal disease who were MSM.
References
Footnotes
Handling editor Joseph D Tucker
Twitter @EricPFChow
Contributors EPFC and CKF designed the study. MM-S conducted the data analysis, performed the chart review and wrote the first draft of the manuscript. All authors were involved in data interpretation, revised the manuscript critically for important intellectual content and approved the final version.
Funding EPFC was supported by the National Health and Medical Research Council (NHMRC) Early Career Fellowships (GNT1091226).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Alfred Hospital Ethics Committee, Melbourne, Australia (242/19).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.