Article Text

Abstract
Objective The objective of this study was to explore young people’s perspectives barriers to chlamydia testing in general practice and potential intervention functions and implementation strategies to overcome identified barriers, using a meta-theoretical framework (the Behaviour Change Wheel (BCW)).
Methods Twenty-eight semistructured individual interviews were conducted with 16–24 year olds from across the UK. Purposive and convenience sampling methods were used (eg, youth organisations, charities, online platforms and chain-referrals). An inductive thematic analysis was first conducted, followed by thematic categorisation using the BCW.
Results Participants identified several barriers to testing: conducting self-sampling inaccurately (physical capability); lack of information and awareness (psychological capability); testing not seen as a priority and perceived low risk (reflective motivation); embarrassment, fear and guilt (automatic motivation); the UK primary care context and location of toilets (physical opportunity) and stigma (social opportunity). Potential intervention functions raised by participants included education (eg, increase awareness of chlamydia); persuasion (eg, use of imagery/data to alter beliefs); environmental restructuring (eg, alternative sampling methods) and modelling (eg, credible sources such as celebrities). Potential implementation strategies and policy categories discussed were communication and marketing (eg, social media); service provision (eg, introduction of a young person’s health-check) and guidelines (eg, standard questions for healthcare providers).
Conclusions The BCW provided a useful framework for conceptually exploring the wide range of barriers to testing identified and possible intervention functions and policy categories to overcome said barriers. While greater education and awareness and expanded opportunities for testing were considered important, this alone will not bring about dramatic increases in testing. A societal and structural shift towards the normalisation of chlamydia testing is needed, alongside approaches which recognise the heterogeneity of this population. To ensure optimal and inclusive healthcare, researchers, clinicians and policy makers alike must consider patient diversity and the wider health issues affecting all young people.
- adolescent
- behavioural science
- chlamydia infection
- general practice
- qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Background
Chlamydia is the most commonly diagnosed sexually transmitted infection (STI) in England, comprising 49% of STI diagnoses in 2018.1 Young people experience the highest rates of chlamydia, accounting for 60% of diagnoses in 2018.1 Chlamydia is largely asymptomatic and can result in serious health consequences if left untreated (eg, pelvic inflammatory disease and infertility). Testing and early treatment, therefore, are required to prevent onward transmission and potential negative health outcomes.
UK context
In the UK, with the aim of controlling transmission through early detection and treatment, the National Chlamydia Screening Programme (NCSP) was established in 2003, recommending that all sexually active individuals under 25 are tested annually or on change of sexual partner.2 Although more tests are performed in specialist settings,1 the NCSP advocates a wide range of opportunistic testing across settings (eg, primary care settings such as community pharmacies and general practice) and via tests ordered online. While online testing has increased in recent years (11% of total tests in 2017 to 17% in 2018), almost one-fifth (20% in 2017; 18% in 2018) come from primary care (including general practice).1
General practice offers considerable testing opportunities: approximately 60% of young men and 75% of young women attend annually3 and young people report positive attitudes towards general practice testing.4 Furthermore, regular opportunistic testing is facilitated by patients attending for other reasons,2 unlike testing via specialist services (including online services) which requires individuals to seek out testing. A recent review identified patient barriers to testing including lack of knowledge, perceived low risk, embarrassment, fear and stigma and facilitators including increased awareness and self-sampling.5 It remains unclear how to translate knowledge of these factors into effective interventions and clinical practice. Interventions have had varied results,6 the majority demonstrating only modest effects.7 8 These results may owe in part to a neglect of psychological behavioural theory.
Behavioural theory
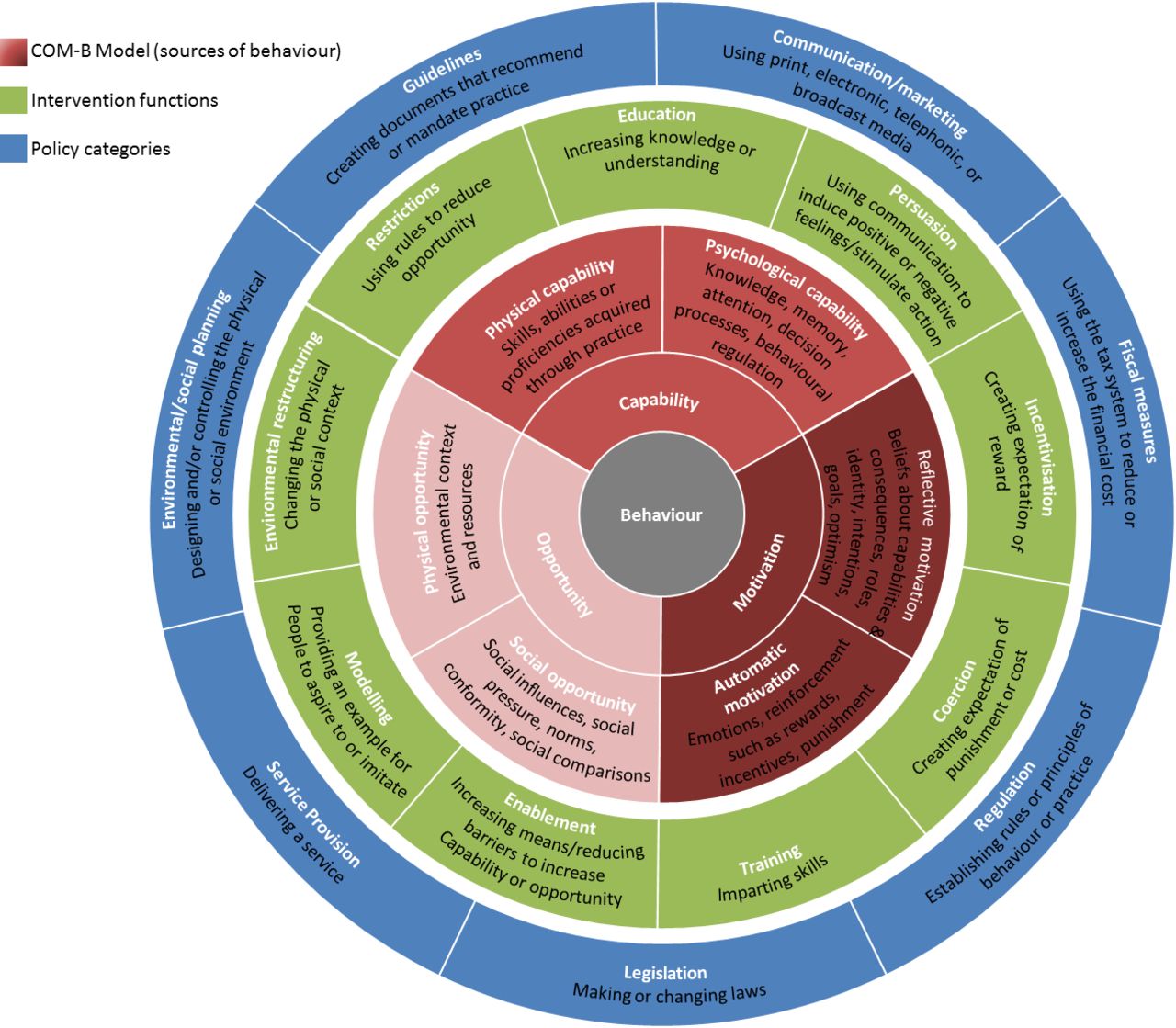
In order to change a given behaviour and develop effective interventions, it is necessary to have a theoretical understanding of said behaviour.9 The Behaviour Change Wheel (BCW) is a meta-theoretical framework and three-tiered tool to construct behaviour change interventions (see figure 1 10 11). The first tier—the Capability, Opportunity and Motivation Model of Behaviour (COM-B)—posits that behaviour results from the interaction of capability (psychological (knowledge); physical (skills)), opportunity (social (societal influence); physical (environmental resources)) and motivation (automatic (emotion); reflective (beliefs about capabilities)). For a person to engage in a specific behaviour (eg, accepting/requesting a chlamydia test), they need to (1) be psychologically and physically able; (2) have the physical and social opportunity and (3) want or need to do the behaviour. The second tier (Intervention Functions) outlines nine categories through which behaviour can be changed: education, persuasion, incentivisation, coercion, training, restriction, environmental restructuring, modelling and enablement. The third tier (Policy Categories) details seven policy strategies to support interventions functions to bring about behaviour change: communication/marketing, guidelines, fiscal measures, regulation, legislation, environmental/social planning and service provision.

{kind=link}
The Behaviour Change Wheel (Michie et al 10). COM-B, Capability, Opportunity and Motivation Model of Behaviour.
The advantage of the BCW is this framework helps to identify a range of factors influencing behaviour (tier one), and potential intervention (tier two) and implementation (tier three) options that could help support change in the given behaviour. The BCW has already supplied the foundation for several health-behaviour interventions;12–18 thus, applying the BCW to general practice chlamydia testing could aid intervention development to increase testing.
Current study
The purpose of this study was to explore: (1) barriers to chlamydia testing in general practice; (2) potential intervention functions to overcome identified barriers and (3) potential policy categories to support intervention functions from the perspective of young people.
Method
Participants
Semistructured individual interviews were conducted with 16–24 year olds in the UK. Purposive and convenience sampling methods were used: snowballing, social media advertisements (eg, Facebook, Twitter, Instagram) and promotions by organisations and charities. Over 600 groups from across the UK were contacted (eg, youth choirs, student unions, community colleges, football clubs, youth political parties, sexual health charities). The aim was to reach a diverse population with representation across demographics (sex, age, ethnicity, education level and chlamydia testing experience).
Procedure
Interviews were conducted in person (n=9) or via telephone (n=19). Participants could choose to participate in person or via telephone to allow people from a variety of locations to take part and to enhance participant comfort. Some individuals feel more comfortable discussing sensitive topics while being anonymous. Phone interviews can increase participants’ perceptions of anonymity, which may therefore enhance the quality of the data produced.19–25 Notably, a direct comparison of transcripts from in-person and phone interviews found that both produced similar data.24
For efficiency, the participant information sheet, consent form and demographic questions were emailed to participants 1 week in advance of the interview. An interview schedule guided discussions (online supplementary file 1) which was iteratively developed through literature reviews, expert consultation and patient and public involvement. A £10 shopping voucher was offered to all as an incentive. Data collection continued until data saturation was reached.26
Supplemental material
Data analysis
On average, interviews lasted 31 min (range=19–42 min). Interviews were digitally recorded and transcribed verbatim. Identifying information was removed.
Analysis and data collection took place simultaneously to enable emerging topics to be investigated in future interviews. Data were subject to inductive thematic analysis27 and mapped onto the BCW. The following procedure was employed: (1) The first transcript was read several times to increase data familiarity. Notes were made regarding insightful comments. (2) Transcripts were coded using NVivo12. (3) Once all transcripts were coded, a list of codes was constructed and sorted into provisional themes/subthemes. (4) The thematic list was reviewed and refined; codes and transcripts were revisited to explore whether themes/subthemes satisfactorily represented the data. (5) A final list of themes/subthemes was created and mapped onto the BCW (see online supplementary file 2 for a thematic overview).
Supplemental material
To ensure rigorous analysis and to validate findings,28 all transcripts were analysed independently by two authors (LM/HH), and other coauthors (GR/JS/JC) analysed a subset of transcripts (ie, two transcripts). Resultant codes and themes were discussed and compared at regular data-analysis meetings to ensure data were represented and displayed in a meaningful manner. No major differences were found; minor discrepancies were discussed. Consequently, BCW categorisation was conducted by the first author (LM) following expert guidelines10 11 in consultation with team members at data-analysis meetings (JMS/JAC/GR). Discrepancies were resolved by consensus.
Results
Twenty-eight interviews were conducted. Participants were predominantly heterosexual (n=19), White British (n=22), female (n=18), students (n=11) and had previously had a chlamydia test (n=17) (online supplementary file 3). Two participants were previously diagnosed with chlamydia. A thematic overview of all findings is provided in online supplementary file 3. The identified barriers to testing (see table 1), interventions functions (see table 2), and policy categories (see table 3) are described in turn.
Supplemental material
Behavioural diagnosis of chlamydia testing with the COM-B Model: barriers to testing in general practice with illustrative quotations
Potential intervention strategies: Interventions options and illustrative quotations to overcome barriers to chlamydia testing in general practice
Potential implementation strategies: policy categories and illustrative quotations to support intervention functions and overcome barriers to chlamydia testing in general practice
Barriers to testing
The identified themes and sub-themes for barriers to testing, and illustrative quotes, are provided in table 1.
Physical capability (physical skills)
Several female participants were concerned about performing self-collected vulvovaginal swabs, particularly doing something wrong and impacting result accuracy (see table 1, quote number 1.1: Q1.1). Many viewed self-sampling positively, however, and the opportunity to ask questions and raise concerns with a healthcare professional (HCP) was important for younger, less experienced and first-time testers (Q1.2; Q1.3).
Psychological capability (knowledge)
Over half of the participants discussed their—and others’—lack of chlamydia knowledge and awareness, for example, that chlamydia could be asymptomatic (Q1.4), ways of transmission (Q1.5), what testing involves (Q1.6, Q1.7) and ease of treatment (Q1.8). Some were not aware that testing is available in general practice (Q1.9; Q1.10).
Reflective motivation (evaluations, beliefs and plans)
Testing was not a high priority for many; participants cited being ‘too busy’ or forgetting to test (psychological capability; Q1.11). This stemmed from perceptions of low, or no, personal risk of acquiring chlamydia. Many discussed ‘sexual invincibility’ and viewed themselves as impervious to chlamydia, regardless of sexual behaviour (Q1.12).
Beliefs that monogamous relationships meant no risk of chlamydia were salient. However, one participant shared how she acquired chlamydia during what she believed to be a mutually monogamous relationship (Q1.13). Others had not considered that asymptomatic infections could pre-date relationships if both partners had not tested (Q1.14).
Some felt chlamydia was not serious and perceived other STIs as more severe; this was especially apparent for participants who previously had chlamydia (Q1.15). A few participants wanted to be tested for all STIs, not ‘just’ chlamydia; they felt that if there is the potential for chlamydia, there also exists potential for infection by other, ‘more serious’, STIs (Q1.16).
Automatic motivation (emotions and impulses)
Emotional responses (embarrassment, fear and guilt) were problematic for many. Young people could feel uncomfortable discussing sexual health in person, especially if they have known their general practitioner (GP) for a long time (Q1.17). Embarrassment could result from being seen by someone known to them (friends, neighbours; Q1.18 or from the testing procedure itself (perception that testing is invasive (Q1.19) and required showing genitals to HCPs (Q1.20)). Fear resulted from the long-term effects of chlamydia on infertility (Q1.21), expectations of stigma (social opportunity; Q1.22), not knowing what the testing process involves (psychological capability; Q1.23) and the possibility of receiving a positive test result (Q1.24). One participant discussed guilt as a barrier due to infidelity during a monogamous partnership and using denial (and therefore not testing) as a coping mechanism (Q1.25).
Physical opportunity (afforded by the environment)
Many felt the UK National Health Service (NHS) primary care context reduced physical opportunities for testing through structural barriers (Q1.26). One participant was not registered with a GP (Q1.27), making appointments can be difficult (Q1.28) and participants were unwilling to take time off work/study to attend (Q1.29). Although some practices offered walk-in clinics, these were usually for urgent cases. Several felt that there was no urgency with chlamydia (especially if asymptomatic) so testing can be delayed (Q1.30, Q1.31). Time within appointments is limited; people usually present with multiple concerns and their original concern gets priority (Q1.32). Several believed GPs were ‘overstretched’, felt rushed during appointments and did not have the space to discuss sexual health (Q1.33). The toilet location was a deterrent if located in an area near other patients (embarrassment; Q1.34).
Social opportunity (afforded by the cultural milieu)
Social stigma stemmed from the taboo nature of sex and, hence, sexual health (Q1.35). Stigma was associated with the need to test (Q1.36) and having a positive diagnosis (Q1.37), due to assumptions of promiscuity (Q1.38). Although several acknowledged that testing and diagnoses do not equate to promiscuity, they felt strongly that other people held these beliefs and feared judgement from staff for their sexual behaviour (Q1.39, Q1.40). Younger participants and those who had never tested were particularly affected, but the impact of stigma lessened with age for some (Q1.41, Q1.42, Q1.43).
Several gay, bisexual and lesbian participants discussed how sexual orientation stigma affected willingness to be tested in general practice. If they were not yet out to family/friends, they were uncomfortable disclosing their sexual orientation to HCPs (Q1.44). Of those who were out, few were comfortable sharing this with HCPs due to expected (Q1.45) and actual (Q1.46), experiences of judgement. Consequently, several preferred sexual health clinics which they felt were better equipped for their specific concerns (Q1.47).
Intervention functions
The identified themes and sub-themes for intervention functions, and illustrative quotes, are provided in table 2.
Education (increasing knowledge)
The majority expressed the need for more public awareness and information on the methods of transmission (Q2.1); existence of free general practice testing (Q2.2, Q2.3); testing processes (Q2.4); testing benefits and consequences of not testing (eg, infertility; Q2.5, Q2.6) and ease of treatment (Q2.7, Q2.8). Participants of all ages felt that younger age groups would benefit the most from education (Q2.9, Q2.10, Q2.11, Q2.12). This could be supported by school-based education (Q2.13), which most felt was either absent from their curriculum (Q2.14) and, when it was included, several felt it lacked specific elements that they perceived to be valuable (eg, emotions, pleasurable sex, STIs; Q2.15). Of the sexual minority participants who had received sex education, all felt the information they received was inappropriate for them—typically, the focus was on avoiding pregnancy (Q2.16).
Persuasion (communication to induce feelings or stimulate action)
Participants noted that communication could induce positive and negative feelings to encourage testing. Positive communication should frame testing as a responsible (Q2.17), healthy behaviour (Q2.18) and a moral obligation to others (Q2.19) to prevent transmission. Communication does not need to be explicit; subtle messages could be effective; for example, positive verbal reinforcement (praise; Q2.20) by HCPs when discussing testing could use people’s desire to conform by focusing on the message that ‘everyone does it’ (improving normalisation; Q2.21). Imagery (eg, depictions of chlamydia consequences) and data (eg, statistics on those infected) could be used to induce negative feelings (fear), to stimulate action (Q2.22). Communication should challenge beliefs and perceptions of chlamydia testing treatment, the long-term impact of undiagnosed infections which may induce fear and, potentially encourage testing (Q2.23, Q2.24, Q2.25).
Environmental restructuring (changing physical or social context)
Participants wanted more accessible appointments, flexible opening hours and walk-in clinics for non-emergency issues (Q2.26, Q2.27). Discreet access to toilets and kit collection points and sample drop-off boxes in the toilet cubical (see policy category—service provision) would help overcome barriers (Q2.28, Q2.29).
Modelling (providing examples to aspire to/imitate)
Rather than purely giving young people information and telling them what to do (or not to do), participants suggested it could be more effective to show them real life examples of how to test (eg, self-sample collection; Q2.30). Providing positive models of what they should do (eg, request a test, accept a test) could also reinforce testing importance; several spoke of credible sources such as celebrities and television/movie characters (Q2.31, Q2.32). Knowing that friends also test could help shape their thinking, which could be achieved through friend referrals or encouraging friends to attend testing together (Q2.33, Q2.34).
Policy categories
The identified themes and sub-themes for policy categories, and illustrative quotes, are provided in table 3.
Communication and marketing (print, electronic, telephonic or broadcast media)
Public awareness campaigns and advertisements were identified as essential for increasing awareness and normalisation, including adverts in the community (eg, universities, see table 3, Q3.1), on television and radio (Q3.2) and leaflets and posters in general practice (Q3.3). Social media was highlighted as an appropriate method for reaching young people due to frequent use (Q3.4) and could support modelling and persuasive interventions. An annual reminder letter (or phone call) sent to younger age groups (16–17 year olds) could increase awareness, help make testing a priority and normalise testing (Q3.5).
Participants wanted clear instructions for self-sampling kits, accompanied by demonstration videos via websites to overcome capability barriers (Q3.6).
Service provision (delivering a service)
Most would welcome testing if offered; if they have to seek it out, it is unlikely to happen—particularly for those for whom testing is not a priority (Q3.7). Providing the option of attending an alternative HCP within the practice (staff not known to patient) would encourage testing (Q3.8). Only one female participant expressed a preference for a same-sex HCP; she felt female GPs could relate to her issues better (Q3.9).
Regarding the provision of alternative sampling methods, the majority preferred urine samples over swabs (Q3.10) and self-administered swabs over HCP-administered swabs (Q3.11). Two participants preferred HCP-administered swabs to ensure samples were collected ‘correctly’ (Q3.12). The provision of ‘discreet’ systems in practice (test collection points, available in toilets) and self-sampling kits to complete elsewhere (at home with return via post or drop-boxes in practice) would increase testing (Q3.13, Q3.14, Q3.15, Q3.16). This would avoid face-to-face contact and potentially embarrassing situations, enabling a sense of anonymity. It was deemed essential to provide multiple options to test—one size will not fit all (Q3.17).
The introduction of online testing, via practice websites, was raised as having the potential to encourage testing (Q3.18). Not everyone wanted testing to move completely online, with some indicating they would like the physical presence of a HCP to ask questions if doing self-sampling—at home or at the practice (Q3.19).
The inclusion of chlamydia testing as part of a young person’s annual health check was raised. Similar to the NHS Health Check for over 40 year olds, a young person’s health check could assess physical health—including chlamydia and wider STI testing (Q3.20).
Guidelines (documents to mandate practice)
Many believed a ‘test during all youth consultations’ policy would increase testing. Most would accept if offered during a non-sexual health consultation (Q3.21). However, three participants felt this could lead to embarrassment or judgement if chlamydia is raised ‘out of the blue’ (Q3.22). Offers must be approached sensitively, in a non-judgmental manner (Q3.23). Several participants said standard questions could be used (Q3.24), asked of all young people and should be non-judgemental, friendly and reassuring to alleviate embarrassment and reduce stigma (Q3.25). As well as facilitating a more comfortable environment, this would increase the likelihood of them returning (Q3.26).
Discussion
This study explored barriers to chlamydia testing in general practice for young people and identified several intervention (increasing knowledge, inducing emotional reacting, changing physical and social contexts) and implementation (communication, service delivery, guidelines for HCPs) strategies to overcome these barriers using the BCW. Barriers such as lack of awareness/knowledge, embarrassment, fear, low risk perceptions and stigma continue to be an issue for young people.5 The UK primary care context reduced opportunities for testing, potentially reflecting NHS financial pressures,29 with GP workloads surpassing ‘unsustainable levels’, due to increasing consultations and administrative tasks.30 ,w1 Several underlying reasons for barriers emerged, including the concept of ‘sexual invincibility’ as an explanation for low risk perceptions. This concept has been linked to risk-taking behaviours, including unprotected sexw2 and may be linked to cognitive developmental factors such as the ‘personal fable’—a young person’s belief that they are unique and, therefore, invulnerable.w3 Young people often believe negative health consequences will not affect them. Such cognitive immaturity declines in later adolescents; interestingly, acknowledgement of sexual invincibility was only raised by older participants (21–24 years).
Some contradictory findings emerged. Several participants felt that fear (of receiving a positive test results and long-term impact on fertility) could discourage testing. Conversely, others felt that fear tactics (imagery and statistics) could stimulate testing. The moral aspect of inducing fear for public health promotionw4,w5 has been questioned, as attempts to trigger negative emotions in response to infection may actually reinforce stigmatisation.
Regarding reducing barriers to increase testing, greater education and awareness were deemed important, consistent with previous literature.5 This could be achieved via school-based education and multiplatform public awareness campaigns, including social media leaflets, posters, TV and radio. A recent study found Facebook advertisements resulted in a 41% increase in chlamydia test-kit ordered online,w6 reflecting perhaps the high internet usage in 16–24 year olds.w7 However, as illustrated by previous interventional studies focusing on patient education,w8-10 information alone would not be enough to increase testing.w11-13
Testing opportunities need to be expanded via service provision, guidelines and environmental restructuring. Young people favoured universal testing offers, delivered in a non-judgemental, friendly, manner; interestingly, previous literature has found interventions which encourage HCPs to offer tests to all young people to have an impact on testing rates.w14 Young people also want flexible appointments with options for: (1) sample collection (direct from HCP, in toilets, online); (2) sampling method (urine, HCP-administered swab, self-administered swab with easy-to-follow instructions); (3) sample completion location (at home, in practice); (4) sample return (direct to HCP, drop-box, post). Online testing was perceived favourably, linkage to general practice websites was suggested and viewed positively, but online systems should not replace in-person contact. Similar to information provision, increasing physical opportunities may not, by itself, be enough to increase testing.
It was evident that normalisation is key to increasing testing. Normalisation would require a multipronged approach which includes increasing knowledge and providing greater opportunities and also challenging perceptions of chlamydia and STIs more generally. The cognitive developmental stage of this population should be considered; early adolescence is a time when the drive to conform is strongest,w15 as are feelings of invulnerability to negative health consequences.w2,w16 Young people need to be persuaded that testing (and treatment) is easy; it is a healthy, responsible, behaviour, which ultimately will benefit them and their partners. As well as communicating these messages via campaigns, subtle positive verbal reinforcement from HCPs and the increased visibility of others who test (credible sources such as peers and celebrities) may be effective.
Limitations
We attempted to recruit a diverse sample, including paid adverts on three social media three, and emails to over 600 organisations. However, the majority of participants were female, White, students, educated and over 20 years old. All participants identified as cis-gender (gender identity corresponds with birth sex). The experiences of transgender/gender diverse individuals, cis-men, those with lower education, those under 20 years and other ethnicities may not be well represented. One potential explanation for the lack of diversity is that recruitment materials and strategies were developed with members of the public who were also White, cis-gender, educated, women, over 20 years of age. Future research should attempt to engage with more diverse populations from conception through to completion.w17
Given the sensitive nature of the subject, those who participated could differ from those who refused to take part. However, we provided the option of in-person or phone interviews to reach those who may have been reluctant to take part. Phone interviews can increase participants’ sense of anonymity regarding sensitive topics, increasing data quality.22 For the current study, we felt these benefits outweighed the disadvantages (lack of visual and non-verbal cues) of this method. Similar data were produced by both mediums in our study; however, a comparative methodological analysis is beyond the remit of this paper. The average length of the interviews (phone and in-person) was rather short; this could be due to participants having time to consider the aim of the research in advance (study materials were sent 1 week before interviews took place); indeed, several participants provided succinct, well thought out, responses.
Distinguishing between some BCW categories was challenging. For example, embarrassment is an emotional response, so we categorised this as automatic motivation. However, it is created by the presence of others and perceived socially (un)acceptable behaviours; hence, it could have been categorised under social opportunity. There is potential overlap between categorisations within psychological capability and reflective motivation; for example, perceived low risk (reflective motivation) could be due lack of information and awareness on the risk of transmission (psychological capability), illustrating the complex interplay between components of the first tier of the BCW. No themes were categorised under enablement, defined as ‘increasing means/reducing barriers to increase capability (beyond education and training) or opportunity (beyond environmental restructuring)’. Normalisation was not included as a distinct theme, but the means through which normalisation could be achieved fit into several other categories (eg, education, modelling, guidelines).
Implications for research, policy and clinical practice
Any attempt to improve young people’s sexual health must recognise subpopulations. Experiences will differ due to, for example, age, employment, experiences and sexual orientation. Efforts to increase testing should focus on the youngest of young people, who were believed to be affected more by stigma, embarrassment and feelings of invulnerability and were less aware of testing importance and procedures. Several participants identified as sexual minorities; most had not disclosed their sexual orientation to their HCP due to discrimination concerns and negative judgements. Consequently, several sexual minority participants were uncomfortable with testing in general practice. This warrants further attention, particularly given the current UK situation, whereby sexual health clinics are closing due to lack of funding,30 almost one-fifth of opportunistic asymptomatic chlamydia testing is conducted in general practice1 ,w18 and the NHS recommends that GPs ask patients aged 16 and older about their sexual orientation.w19
Conclusion
At this juncture, we cannot definitively state what an effective intervention to increase chlamydia testing in general practice would consist of. This study has provided novel insights into what young people believe would be effective. Interventions need to be tailored to young people; they are a heterogeneous population. Simply providing information or opportunity will not bring about dramatic increases in testing; a structural and societal shift towards normalising chlamydia testing is required. Changing social norms will not be an easy feat.w20,w21 As evidenced here, a multifaceted approach is needed which challenges their young people’s perceptions of the infection (eg, that it is a serious STI), of their peers (eg, that their friends test) and of their self-identity (eg, that young people are not invincible), while simultaneously works towards providing education (eg, testing and treatment processes), greater opportunities for testing (eg, how and where tests are conducted), role models and examples of the behaviours (eg, through credible sources) and guidelines for HCPs (eg, universal testing without judgement).
This paper has provided one piece of the puzzle in developing theory-based and evidence-based interventions to increase chlamydia testing in general practice; however, further strands of evidence are required. Future research should engage primary care staff and commissioners to understand what needs to change from their perspectives and what it is realistically possible to change in the current UK primary care context. The cost-effectiveness and long-term sustainability of efforts to increase testing also require further exploration. Then, once these strands of evidence have been triangulated, the next stage will be to identity the active ingredients and mechanisms of action required to significantly influence chlamydia testing. Nonetheless, researchers, clinicians and policy makers must keep patient diversity at the forefront to ensure optimal and inclusive healthcare. Addressing the health issues affecting all young people will be a crucial part of improving national public health and eliminating STIs.
Key messages
Increasing information and opportunities alone may not equate to increases in testing; a multifaceted, flexible approach is required which challenges negative perceptions of chlamydia.
Communication and messages to encourage testing should take into account adolescent cognitive (feelings of invulnerability) and social (desires to conform) developmental factors.
Efforts to increase testing must be inclusive and consider patient diversity; the needs of sexual and gender minorities need to be acknowledged and met.
Supplemental material
Acknowledgments
With grateful thanks to all the young people who gave up their time to participate in this study. We acknowledge members of the NIHR HPRU in BBSTI Steering Committee: Caroline Sabin, John Saunders, Catherine H. Mercer, Gwenda Hughes, Greta Rait, Jackie Cassell, William Rosenberg, Tim Rhodes, Kholoud Porter, Samreen Ijaz and Sema Mandal.
References
Footnotes
Handling editor Jo Gibbs
Twitter @Dr_L_McDonagh, @saunders_j
Contributors LM developed and refined the study protocol with contributions from HH, GR, JAC and JMS. LM prepared the manuscript. HH undertook data collection. LM and HH reviewed the transcripts and conducted data coding. LM conducted theme development, interpretation and report writing. LM conducted the model categorisation with input from all coauthors. GR, JAC and JMS provided methodological guidance and contributed to the coding, theme development, data interpretation, data synthesis and model categorisation. All authors read and approved the final manuscript.
Funding The research was funded by the National Institute for Health Research Health Protection Research Unit (NIHR HPRU) in Blood Borne and Sexually Transmitted Infections at University College London in partnership with Public Health England (PHE), in collaboration with London School of Hygiene & Tropical Medicine (LSHTM).
Disclaimer The views expressed are those of the authors and not necessarily those of the NIHR, the Department of Health and Social Care or Public Health England.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from the UCL Research Ethics Committee (project ID number: 10319/001).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Due to participant privacy concerns, data are not available for sharing.