Article Text

Abstract
Objectives Previous studies have demonstrated that rectal douching (RD) is associated with HIV acquisition among men who have sex with men (MSM). However, the precise mechanism underlying the association between RD and HIV remains unclear.
Methods We recruited participants over WeChat from October 2017 to October 2018. Respondents received mailed HIV self-testing kits, uploaded images of HIV self-test results and completed an online electronic questionnaire simultaneously. The questionnaire assessed sociodemographic characteristics, RD practices and sexual risk behaviours. HIV status was measured as the result of the HIV self-testing. The Baron and Kenny statistical method was used to assess the association between RD and HIV, controlling for condomless anal intercourse (CAI) and rectal bleeding.
Results Of 1365 participants, 39.93% (545/1365) reported RD in the past 6 months, 60.07% had multiple male sexual partners and 43.08% had CAI in the past 6 months. The prevalence of HIV, based on self-testing, was 3.37% (46/1365). Multivariable logistic analysis showed RD was significantly associated with bottom sexual role (adjusted OR (aOR) 14.0; 95% CI 9.8 to 20.2), having multiple male sexual partners (aOR 1.8; 95% CI 1.4 to 2.2), CAI (aOR 1.3; 95% CI 1.0 to 1.6), rectal bleeding (aOR 2.0; 95% CI 1.6 to 2.6) and HIV infection (aOR 1.9; 95% CI 1.0 to 3.4). Baron and Kenny analysis found both CAI (aOR 2.2; 95% CI 1.2 to 4.1) and rectal bleeding (aOR 1.9; 95% CI 1.0 to 3.4) play a mediating role in the association between RD and HIV.
Conclusions Our study results confirmed the relationship between RD and HIV, and found CAI and rectal bleeding mediated HIV infection in Chinese MSM who douched. Strategies should be encouraged to strengthen health education and reduce high-risk sexual behaviour in order to reduce the risk of HIV in MSM who use enemas. Rectal microbicides may represent an efficient means of providing HIV prophylaxis among MSM.
- HIV
- gay men
- China
- epidemiology (general)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The epidemic of HIV infection remains disproportionately high globally among men who have sex with men (MSM).1 2 China also faces a significant challenge imposed by the HIV epidemic among certain populations, particularly MSM. National surveillance data have indicated that the prevalence of HIV among MSM increased from 0.9% in 2003 to 8% in 2015.3 4 Given the disproportionately high burden of HIV infection among MSM, it is essential to understand the sexual behaviours and preferences of this key population in order to develop a novel and effective strategy to prevent HIV infection.
Rectal douching (RD) is the act of using tools to insert liquid into the rectum for the purpose of cleansing. Recent research has raised concerns over the association between RD and HIV infection. A large-scale cross-sectional study, involving 112 countries and 1725 respondents, demonstrated that 66% of participants reported experiencing RD during their lifetime.5 Several previous studies have reported that RD is associated with an increased prevalence of HIV in MSM.6–9 There are various explanations for the association between RD behaviour and HIV infection. Traditionally, it was assumed that RD might result in damage being incurred by the effect of friction on the single-cell epithelium of the rectum, thereby facilitating the entry of pathogens and increasing the acquisition of HIV and other STIs.10 11 Some academics assume that RD is correlated with STIs, including chlamydia and gonorrhoea,12 hepatitis B virus (HBV) and hepatitis C virus (HCV),13 14 and therefore increases the risk of HIV infection by an indirect manner. Previous studies have also investigated the association between RD and certain high-risk sexual behaviours. For example, Noor’s study demonstrated that MSM who douched were more likely to engage in unprotected anal intercourse (AI), and more likely to be associated with HIV, compared with those who did not.7 Furthermore, MSM who practised RD also reported a history of group sex and multiple sexual partners15 16; collectively, these behaviours increase the possibility of HIV infection. However, very little is known with regard to the potential role of high-risk sexual behaviour in the pathway associating RD with the acquisition of HIV.
The complex nature of this relationship suggested that a more accurate and complex model was needed in order to examine the associations between RD, high-risk sexual behaviour and HIV infection. As expected, a mediation model was previously used to assess the mediating role of high-risk sexual behaviours in the association between recreational drug use (RDU) and HIV/STIs.17 Furthermore, previous studies of RD by MSM were mainly conducted in western countries, adopted small sample sizes and were only carried out at a small number of sites, thus limiting the generalisability of the results. Therefore, we conducted a national, behavioural and epidemiological online survey of Chinese MSM in an attempt to propose a conceptual model to assess the mediating role of high-risk sexual behaviours and the association of RD and HIV. We also aimed to acquire a significant body of data relating to the prevalence of RD and its association with HIV infection and high-risk sexual behaviour.
Methods
Study design
Between October 2017 and October 2018, we invited five operators of WeChat public platforms (software product of Tencent, Shenzhen, China), which were actively followed and used by their MSM fans, to help the project release HIVST recruitment advertisements. Individuals were able to click the link of a recruitment advertisement to attend the HIVST project inclusion criteria screening. MSM participants were eligible and are included in the project if they met all the following criteria: (1) born biologically male; (2) aged ≥18 years; (3) having no HIV-positive test history previously; (4) self-reporting had oral or anal sex with other males at least once in their lifetime; (5) agreed to the study contents of this project and provided online informed consent. Then the eligible MSM participants were required to provide their address, phone number and nickname for getting HIV self-testing kits through express mail. After receiving the self-testing kit, the MSM respondents could complete HIV self-testing following the detailed steps of instructions in the express mail. Then, respondents were required to upload their image of self-testing results, and meanwhile, complete an online electronic questionnaire and add the personal WeChat account that dedicated to this project to get help for the interpretation of the HIVST results and receiving questionnaire compensation fees. The researcher staff would review the results uploaded by respondents within 24 hours and give each respondent 15 RMB (US$2.4) through WeChat for the compensation of attending with the questionnaire survey.
Measures
Participants needed to complete a self-administrated electronic survey and reported their (1) demographic data, including age, monthly income, occupation, education and sexual orientation; (2) HIV sexual risk behaviours in the past 6 months, including whether reported practice of RD, the primary venue for seeking male sexual partners, predominant sexual role during AI in the past 6 months, the number of male sexual partners, the use of condoms and rectal bleeding; (3) recreational drug use in the past 6 months, including rush poppers, methamphetamine, amphetamine, tramadol, cocaine, ketamine and ecstasy; and (4) HIV test history, including lifetime HIV test history before attending this HIVST survey and average HIV test interval.
We acquired the HIV status of each participant by self-testing. A finger-prick-based HIVST kit (Wondfo, Beijing, China), approved by the Food and Drug Administration of China, was used in our study. Blood samples were obtained using disposable blood needles and collected by an EDTA-treated capillary. Then, the specimen of blood was dropped on the specimen reaction zone. Finally, Alera Retermine Chase solution was added onto the reaction zone.18 Respondents were then instructed to read the HIV testing results in approximately 15 min.18 To ensure the accuracy of HIV self-testing results, the instructions of HIVST kits detail each step of self-testing process in the form of pictures and text. Besides, a two-dimensional code is provided in the instruction, which allows participants to watch the operation video of HIVST by scanning the two-dimensional code. Moreover, we also provide a personal WeChat account and phone number dedicated to this project, and participants can contact us if they encountered any difficulties during the testing process. For individuals with a reactive HIV test result, we would provide advice for further HIV testing in order to confirm the diagnosis. If a positive diagnosis was confirmed, then we also referred the patient for treatment and care.
Statistical analysis
Chi-square statistics were used to compare the differences in demographics, HIV risk behaviours, and HIV test variables between MSM who reported RD and those who did not. Multiple logistic regressions were also used to estimate the associations between RD and condomless anal intercourse (CAI), RDU, multiple male sexual partners, rectal bleeding, HIV infection and other variables.
We also used the mediation model, using the methods described by Baron and Kenny.19 We performed a series of regression models to estimate the mediating role of CAI and rectal bleeding on the association between RD and HIV. In the mediation model, CAI (M1) and rectal bleeding (M2) served as mediators, RD served as an independent variable (X) and HIV served as a dependent variable (Y). First, we regressed CAI on RD, and then regressed HIV on RD and CAI, respectively. Finally, we regressed HIV on both RD and CAI. Similarly, we further estimated the mediating effect of rectal bleeding on the association between RD and HIV. Demographic variables, including age, monthly income and occupation, which showed statistical significance in the bivariate analyses, based on whether an enema was used, were controlled as covariates for each multiple logistic regression.
All statistical analysis was carried out using SPSS V.22.0. The regression coefficient of each equation was estimated by adjusted OR (aOR) and 95% CIs. A two-tailed alpha of 0.05 was considered to be statistically significant.
Results
Demographic data
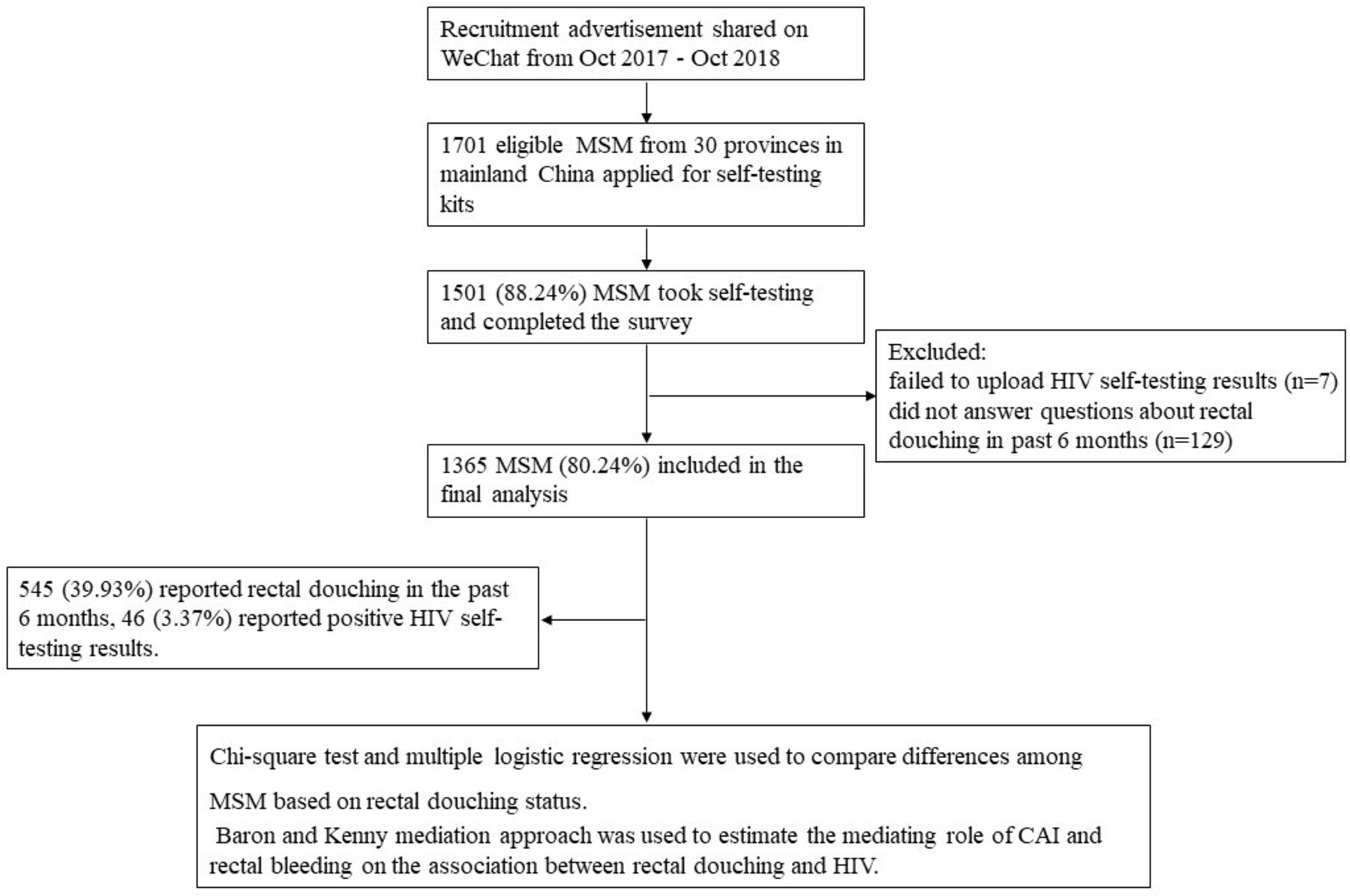
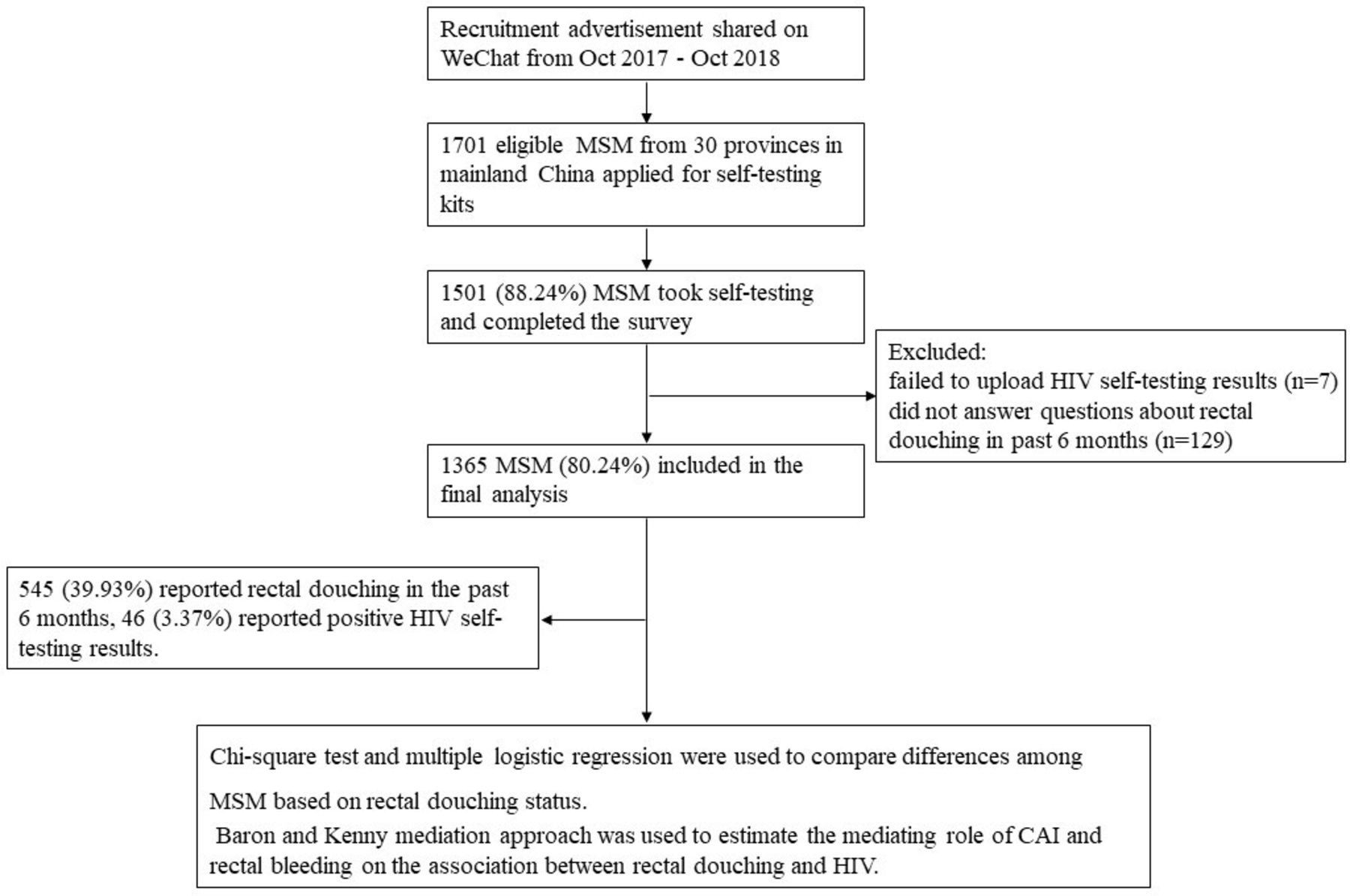
In total, 1701 MSM from 30 provinces in mainland China applied for self-testing kits during 2017–2018. Of those who applied, 1501 (88.24%) conducted self-testing and completed the survey. After the exclusion of MSM who did not answer questions related to RD practices in the past 6 months, or those that failed to upload their HIV self-testing results, 1365 (80.24%) eligible participants were included in the final analysis (figure 1). The sociodemographic information of these MSM participants is shown in table 1. The analysis showed that 51.36% of respondents were 25 years or older, had a monthly income of US$300–900 or higher (66.30%), and had attended high school or college (95.97%). In addition, the majority of the participants identified their sexual orientation as homosexual (70.92%).
{kind=link}
Flowchart of study recruitment, eligibility, and analysis among MSM population. CAI, condomless anal intercourse; MSM, men who have sex with men.
Social and behavioural characteristics and HIV prevalence among Chinese MSM (n=1365)
RD, high-risk sex and HIV test results
Of the 1365 respondents, 545 (39.93%) reported that they had used rectal douches over the past 6 months. Furthermore, 60.07% of respondents reported that they had multiple male sexual partners, and 43.08% had reported CAI in the past 6 months; 46 MSM participants reported positive HIV test results. The prevalence of HIV, based on self-testing results, was 3.37% (46/1365). After adjustment for demographic variables, multivariable analysis showed that those who used rectal douches were significantly associated with taking anal sex as bottom role (vs top role) (aOR 14.0; 95% CI 9.8 to 20.2) or versatile role (vs top role) (aOR 9.2; 95% CI 6.4 to 13.3), seeking male sexual partners from the Internet (aOR 1.4; 95% CI 1.0 to 1.9), multiple male sexual partners (aOR 1.8; 95% CI 1.4 to 2.2), CAI (aOR 1.3; 95% CI 1.0 to 1.6), RDU (aOR 3.3; 95% CI 2.6 to 4.1), rectal bleeding (aOR 2.0; 95% CI 1.6 to 2.6), recent testing for HIV (aOR 1.8; 95% CI 1.3 to 2.4) in the past 6 months, and a higher HIV prevalence (aOR 1.9; 95% CI 1.0 to 3.4), compared with those who did not use RD (table 2) (each p<0.05).
Multivariate association between rectal douching and behavioural characteristics and HIV prevalence among Chinese MSM (n=1365)
Association between RD and CAI, rectal bleeding and HIV
RD was significantly associated with HIV infection (aOR 1.9; 95% CI 1.0 to 3.4). Mediation analysis, in which CAI was considered as a potential mediator for the association between RD and HIV infection, showed that CAI was independently associated with both RD (aOR 1.3 95% CI 1.0 to 1.6) and HIV infection (aOR 2.3; 95% CI 1.3 to 4.3). When CAI and RD were both included in this model, the association between CAI and HIV infection (aOR 2.2; 95% CI 1.2 to 4.1) remained significant; however, non-significant associations were identified between RD and HIV infection (aOR 1.8; 95% CI 1.0 to 3.2). Thus, CAI serves as a significant mediator in the association between RD and HIV infection (table 3).
Mediating effect of CAI and rectal bleeding on rectal douching and HIV infection in Chinese MSM
Analysis of the potential mediating role of rectal bleeding in the association between RD and HIV infection is also presented in table 3. A significant association was identified between rectal bleeding and HIV (aOR 1.9; 95% CI 1.0 to 3.4) in mediation analysis. We also identified that rectal bleeding also served as another mediator in the association between RD and HIV infection.
Discussion
To our best knowledge, this is the first national-level study to assess the RD behaviour and its correlation with HIV in MSM population, and this study also demonstrates the role of some high-risk sexual behaviours in the mediating of association between RD and HIV. Our mediation models found that CAI and rectal bleeding behaviours make a significant contribution to HIV risk in MSM who reported RD. The practice of RD was also associated with CAI, RDU, rectal bleeding and multiple male sexual partners. These findings provided further understanding of how RD is associated with HIV infection and provides valuable information for the prevention of HIV with regards to the use of enemas by MSM.
Though the prevalence of RD in Chinese MSM is lower than previously reported in developed countries (39.23% vs 49%–54.3%),6 15 20 nearly 40% MSM in our study reported RD in the past 6 months, indicating the significant international prevalence of these behaviours. In our study, we found MSM with RD practice had higher odds of HIV infection. The odds of acquisition with HIV among MSM with RD practice in our study was relatively lower compared with that of a recent peer meta-analysis study (1.9 vs 2.8).21 One possible explanation is that because of fear of privacy leak, some MSM participants who attended the HIVST project were more reluctant to feed-back after a positive HIVST result is found. Moreover, the HIV prevalence of those MSM respondents who did not feed-back HIVST results may be higher than those who feed-backed, which may underestimate the effect on the actual total estimated prevalence of HIV among total MSM respondents. In addition, this may be due to differences in recruitment methods, over half study MSM subjects in the meta-analysis study were recruited through hospitals or clinics (60.7%), while all the MSM participants in our study were recruited through online sampling.
Our mediation analysis found that CAI and rectal bleeding act as mediators for the association between RD and HIV. The possible explanation is that the rectum’s single-celled epithelium could be damaged by friction and stimulation because of RD, thereby facilitating the entry of pathogens.11 22 Further, MSM who reported rectal bleeding had a higher risk of HIV infection during anal intercourse compared with those who did not. Simultaneously, high-risk sexual behaviours, such as CAI, may represent another potential mechanism underlying the association between RD and HIV. One possible explanation is that MSM who reported RD often co-occurs with CAI, and the behaviour of CAI increased the odds of HIV infection among MSM. The findings of our study support the hypothesis of the association between RD and HIV, and provide a useful source of information to develop interventional strategies to help reduce the risk of HIV infection in MSM enema users.
Among Chinese MSM, there is a lack of social attention and media coverage of RD, which likely contributed to a general lack of awareness. Notably, our study found that MSM who reported RD mainly sought male sexual partners from the Internet and had recently tested for HIV. These findings provide a potential mode with which to offer educational materials via online and offline routes. Crowdsourcing, a scalable, cost-effective tool to aggregate community wisdom to solve problems and share solutions with the public, has already been proven to have an effect on the HIV testing and HIV pre-exposure prophylaxis (PrEP) among MSM.23 The novel approach of crowdsourcing that can improve community awareness of RD are needed (eg, a crowdsourcing video and image contest, etc). In addition, public health departments, community-based organisations and HIV testing agencies should also adopt significant roles in the improvement of awareness with regards to enema use, and provide strategies during HIV testing and consultation.
We found that MSM who reported RD was positively associated with a number of high-risk sexual behaviours, including CAI, multiple male sexual partners, RDU and rectal bleeding; these findings were consistent with the existing literature.12 15 20 Specifically, more recreational drugs were reported in those who practised RD than those who did not. This may be partly explained by the fact that RDU bypassed safer sex practices; for example, those who used enemas were also associated with unprotected sex during AI.24 In addition, the use of certain substances (eg, opioids) is associated with the possibility of intestinal dysfunction and constipation, thus potentially creating a demand for RD.25 26 Our data provide further evidence for the link between RD and high-risk sexual behaviour. The co-occurrence of these risk behaviours, including RD, is more likely to contribute to the acquisition of HIV among MSM,7 which indicates a need for interventional strategies to reduce HIV infection in this high-risk sexual environment. Antiretroviral therapy for PrEP has been widely applied in MSM population.27 Rectal microbicides represent another feasible option for HIV prophylaxis, if proven to be efficacious. Some academics have demonstrated high levels of interest in rectal microbicides in the MSM population.28 A gel and douched-based rectal microbicides, which meet the RD need of MSM population, could also provide them an important option for both hygiene and HIV prophylaxis in the future. Future research should also examine the acceptance and potential barriers of rectal microbicides in Chinese MSM.
There are some limitations to this study that need to be considered. First, recall bias, and social desirability bias, may represent an issue as all variables in this study were measured via self-reporting. Second, a cross-sectional study cannot clarify the causal inference and mechanism between RD and HIV infection, and more longitudinal studies are further needed to determine the relationship between RD and HIV among MSM. Third, this study and most previous peer studies did not evaluate the effect of the timing of anal douching (before or after anal sex) and the anal douching devices (commercial RD devices or non-commercial RD devices) on HIV among MSM; further research is required to address this issue. Fourth, compared with the number of HIV-negative MSM (n=1319), the number of HIV-positive MSM (n=46) was much relative smaller, which limited the statistical power for some data analysis results of our study, so further related HIVST should be conducted to MSM population with larger sample size or having higher HIV-prevalence level. Finally, the data described in this manuscript were mainly derived from HIV self-testing users; those who underwent HIV testing in the community or medical facilities were not included; this factor may reduce the generalisability of our data.
In summary, the practice of RD is highly prevalent among Chinese MSM. CAI and rectal bleeding both serve as mediators for the association between RD and HIV acquisition. MSM who reported the use of RD were also more likely to report multiple sexual partners, RDU and a high prevalence of HIV. The public health departments, community-based organisations and HIV testing agencies should now develop strategies to educate the MSM population about the risk of RD and provide health materials to increase awareness. Interventions to reduce high-risk sexual behaviour should be encouraged in the MSM population who practise RD. Rectal microbicides may represent a considerable asset for HIV prophylaxis and therefore mitigate the HIV epidemic in China.
Key messages
Rectal douching (RD) is associated with HIV among men who have sex with men, although the precise mechanism underlying the association between RD and HIV remains unclear.
Condomless anal intercourse and rectal bleeding mediate the association between RD and HIV.
Men who practise RD should be informed of the increased risk of this behaviour and use appropriate interventions to reduce high-risk sexual behaviours.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Acknowledgments
We thank the staff of Rainbow Harbor, the First Affiliated Hospital of China Medical University, and all of our participants for contributing to this project.
References
Footnotes
Handling editor Henry John Christiaan de Vries
Contributors TL, XM, Y-JJ and JX conceived and designed the experiments. TL, XM, EP, YG, ZC and WZ carried out the study and experiments. TL, XM and WD analysed and interpreted the results of study. TL, Y-JJ and JX wrote and revised the manuscript. All authors reviewed the manuscript.
Funding This research was supported by the National Natural Science Foundation of China (81872674), National Science and Technology Major Project (2018ZX10101-001-001-003), and Mega-Projects of Science Research for the 13th Five-Year Plan (CN) (2017ZX10201101-002-007).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics committee of the First Affiliated Hospital of China Medical University (2018-174-2). All procedures were in accordance with all relevant guidelines and regulations. Informed consent was obtained from each participant prior to the survey being provided.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.