Article Text

Abstract
Introduction Voluntary medical male circumcision (VMMC), an effective HIV prevention programme for men, is implemented in East and Southern Africa. Approximately 50% of VMMC clients are aged below 15 years. More targeted interventions to reach older men and others at higher short-term HIV risk are needed.
Methods We implemented a quality improvement project testing the effectiveness of an active referral-based VMMC recruitment approach, targeting men attending STI clinics and those escorting partners to antenatal care (ANC) clinics, at Bwaila Hospital in Lilongwe, Malawi. We compared the proportions aged older than 15 years among men who received VMMC following referral from STI and ANC clinics with those among men referred from standard community mobilisation. We also analysed referral cascades to VMMC.
Results In total, 330 clients were circumcised after referral from STI (242) and ANC (88) clinics, as compared with 3839 other clients attributed to standard community mobilisation. All clients from ANC and STI clinics were aged over 15 years, as compared with 69% from standard community mobilisation. STI clinics had a higher conversion rate from counselling to VMMC than ANC (12% vs 9%) and a higher contribution to total circumcisions performed at the VMMC clinic (6% vs 2%).
Conclusions Integrating VMMC recruitment and follow-up in STI and ANC clinics co-located with VMMC services can augment demand creation and targeting of men at risk of HIV, based on age and STI history. This approach can be replicated at least in similar health facilities with ANC and STI services in close proximity to VMMC service delivery.
- Africa
- circumcision
- male
- prenatal care
- preventive health services
- HIV
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction/Background
Male circumcision (MC) reduces heterosexual HIV acquisition in men by approximately 60%.1–3 Over the decade following the 2007 release of the Joint United Nations Programme on HIV/AIDS and WHO recommendation for its use,4 voluntary medical male circumcision (VMMC) was adopted by 15 African countries as an HIV prevention intervention to protect individuals and reduce population HIV incidence.5 6
The UNAIDS and WHO VMMC strategic framework recommends reaching 90% of individuals aged 10–29 years old in VMMC priority countries by 2021,7 but most countries are struggling to reach the key subset, older men at immediate risk of HIV. The US President’s Emergency Plan for AIDS Relief (PEPFAR) has supported VMMC programmes in East and Southern Africa since 2008, totalling more than 22 million circumcisions8 by the end of September 2019, but nearly 50% were among boys under 14 years old. This age skew may result from multiple barriers to VMMC uptake among older men, including cultural barriers, fear of income loss while healing, perception of low HIV risk, stigma, lack of spousal support or access, and perception that circumcision is appropriate only for the young.9 10 If this age predominance continues, much of VMMC’s impact will take more than 10 years to realise. Both intuitively and as confirmed by modelling findings,11 programmes need to target older and higher-risk men more effectively.
The growing literature on VMMC demand creation in higher-impact subpopulations (by age or sometimes behaviour) has identified interventions with some success: cash transfers, sports-based counselling and general VMMC counselling at HIV testing sites.12–15 However, WHO also recommends that VMMC be integrated with other health services16 17 as they seek to become more sustainable, such that these other services may refer appropriate clients. We are unaware of outcome data from this approach, particularly in these high-impact clients. Such efforts can be challenging for health workers to layer on while addressing acute healthcare needs, and any initiatives are not systematically documented or analysed.
In Malawi, with an HIV prevalence of 7.6% among men18 and an ongoing VMMC programme, two potential platforms for both routinising referral of older and higher-risk men and improving VMMC integration with the health system are STI clinics and antenatal care (ANC) clinics. STIs increase risk of HIV by threefold or more,19 making STI clients a priority population for VMMC recruitment. Conversely, medical MC protects against STIs, not only in men but also their female partners, and reduces risk of cervical cancer.20 In Malawi, where HIV prevalence among patients with STI is 22%,21 national guidelines already recommend VMMC referral for uncircumcised men accessing STI services22 after the STI has resolved, but uptake has not been documented. Meanwhile, Malawi’s ANC clinics already engage male partners to promote couple’s testing and family-based HIV care. How the risk of HIV of these men compares with that of the general population is unknown, but they are by definition sexually active and some have partners identified as HIV-positive through ANC. Female partners can also have important roles in men’s decisions to uptake VMMC.23 24 However, there is no documentation of VMMC promotion in these clinics.
We piloted the integration of VMMC messaging, referral and follow-up in ANC and STI clinics in Lilongwe, Malawi. This approach had potential to address some barriers by communicating to these men that they are valued clients for the programme and, in the case of STI clients, reaching them when they were aware of their elevated HIV risk. This quality improvement initiative was evaluated by both determining per cent uptake and absolute numbers of these men becoming VMMC clients, and comparing recruited clients with those referred from routine VMMC demand creation activities on HIV risk measures or proxies.
Methodology
Design: structure, comparator and intervention
This project tested an active referral-based VMMC recruitment approach. The primary analysis compared the major outcome, which is the number of VMMCs in men older than 15 attending ANC and STI clinics, with the number achieved in men unconnected with these clinics, attributed to standard demand creation practices. This analysis also involved monitoring numbers throughout the referral cascade as outlined in the Data Analysis section. The secondary analysis was a retrospective cohort analysis of the ages of men presenting for VMMC, based on referral source (ANC, STI, standard demand creation), to determine differences in this HIV risk proxy by source.
The standard demand creation package serving as a comparator continued unchanged during the study. It involved community sensitisation and advocacy meetings, interpersonal communication, and special events like road shows. All were concentrated in brief campaign periods, typically with 2 weeks of premobilisation before intense service periods spanning days, nights and weekends. Mobilisers leading these efforts are recruited both among satisfied clients and through community leaders identifying interested local residents. They are trained in interpersonal communication skills and relevant content on HIV and VMMC, and provide VMMC information verbally and using posters, flyers and leaflets.
The active referral approach (figure 1), specified a priori, began with training ANC and STI clinic staff on VMMC recruitment strategies; a VMMC script stipulating the benefits of MC; data collection and reporting; and responsibilities of the VMMC mobiliser and ANC and STI providers in the recruitment of clients for VMMC. Clinic nurses added VMMC education to their routine group health education sessions. Interested clients were then offered one-on-one discussion with a VMMC mobiliser stationed at each clinic. The mobiliser provided additional information on VMMC benefits, risks and wound care postsurgery, and educational materials (leaflets and posters) to both male and female ANC and STI clients. Men opting for same-day VMMC were escorted to the on-site VMMC clinic. Those preferring a later date were given appointments, and the mobiliser collected their contact information. STI clinic patients with active infections were first provided with syndromic treatment following national guidelines and then followed up to schedule appointments after treatment. Those missing appointments were called 2 weeks later by the mobiliser to reschedule, and again after 2 more weeks if needed. No financial incentives were provided. Public healthcare in Malawi, including VMMC, is free.
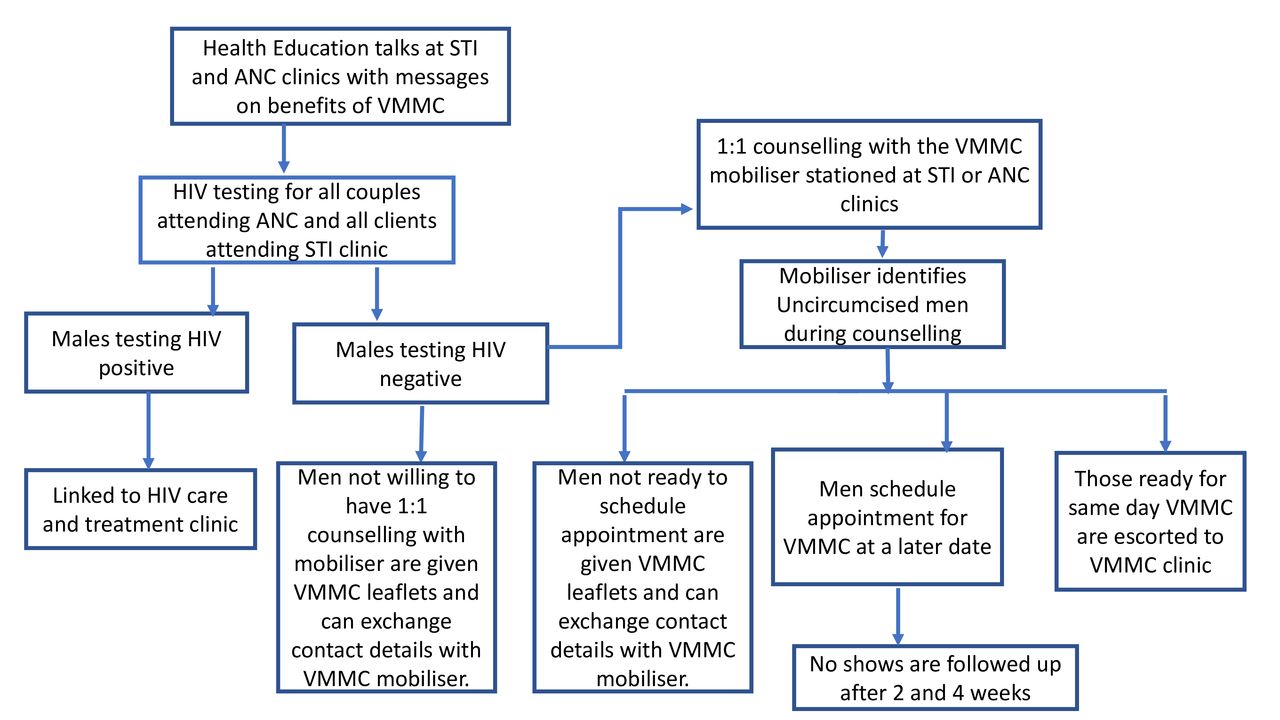
VMMC recruitment diagram for ANC and STI clinics. ANC, antenatal care; VMMC, voluntary medical male circumcision.
This project was a collaboration between PEPFAR’s partners through the US Centers for Disease Control and Prevention: Jhpiego Project IQ, providing VMMC services; and Lighthouse Trust, supporting ANC and STI services.
Data collection
Data for ANC clinic referrals were collected from project launch in October 2018 through November 2019, and for STI clinic from November 2018 through October 2019. At these clinics, the VMMC mobiliser used a referral register to collect demographic information for all clients met one-on-one and contact details for those who scheduled VMMC appointments. Verbal consent was obtained from all clients in one-on-one counselling with the mobiliser and a written consent was obtained from all clients prior to MC surgical procedure. Clients received referral forms at the STI and ANC clinics, which they presented to the VMMC clinic when accessing VMMC services. There, it was attached to the client’s registration form, which also collected client demographics and how the client learnt about the VMMC services.
On a monthly basis, a report was generated, including the number of men presenting by age and HIV status, uncircumcised men counselled on VMMC benefits, men referred and men scheduling appointments, men escorted to same-day VMMC, phone call follow-ups on no-shows at 2 and 4 weeks, and total number of men receiving VMMC.
The total number of VMMCs performed during the preintervention period in November 2017–September 2018 was also drawn from programmatic records, for comparison with total achievements in the same months 1 year later, comprising the majority of the intervention period. These dates were chosen to allow comparison of ‘pure’ preintervention and intervention periods.
Circumcision status was determined through self-report during one-on-one counselling, and in the STI clinic, for a small proportion referred directly by STI providers, by physical examination. Attempts were also made to capture mobiliser time on the ANC clinic, STI clinic and routine community mobilisation work (see the Results section on why these are not shared).
From March to June 2019, we attempted to capture risk behaviour through a questionnaire at the VMMC clinic added to routine data collection practices, based on the risk assessment questionnaire used in the MAXZAM study of cash-based VMMC incentivisation for high-risk men.15 It was administered by the HIV testing providers, optionally, to all clients aged 15 years and above. It captured multiple high-risk behaviours and having received treatment for an STI, each within the past 6 months.
During the data collection period, key external and internal programme events (school holidays, crop-growing and harvesting periods, and circumcision campaigns) with potential impacts on referral were also tracked. The dataset is publically available (online supplemental file 1).
Supplemental material
Data analysis
Client data from the registration form were entered in the routine online client database used by the Bwaila VMMC clinic. Frequency distributions and percentages were used for descriptive analysis of referred clients and of the referral cascade: aggregate numbers of men accessing VMMC services from STI and ANC clinics by age and month, monthly referrals, and referrals receiving same-day MC. From these values, ‘overall’ conversion rates to VMMC (among all men attending each clinic), ‘partial’ conversion rates (among uncircumcised male STI and ANC clients who obtained one-on-one counselling) and contribution rates of STI and ANC clinics to total circumcisions performed were calculated. We plotted monthly conversion rates and contribution rates over time, alongside relevant external and internal events. Total MCs performed at Bwaila were compared between preintervention and intervention periods, defined above, to further clarify the project’s overall impact on VMMC performance. Finally, we performed two post-hoc statistical comparisons to determine the statistical significance of potentially important differences between (1) conversion rates from counselling to obtaining VMMC, among ANC versus STI clients; and (2) proportion aged 15 years and above of clients receiving VMMC, among men referred from ANC or STI clinics versus recruited via standard community mobilisation. These were two-tailed t-tests of proportion performed in STATA (version 16.0) with a significance threshold of p<0.05.
Data on risk behaviour were analysed using STATA. Overall risk was scored as the number of risk behaviours reported. Each behaviour was assessed for statistically significant associations with referral source using the χ2 test at 5% significance level.
Results
Referral cascade and contributions to MCs performed
In total, 330 clients were circumcised at Bwaila VMMC clinic after referral from STI (242) and ANC (88) clinics. The median age of referrals from both STI and ANC clinics was 23 years (range: 15–29 and 19–40 years, respectively). In contrast, 3839 clients were circumcised after referral from standard community mobilisation, with a median age of 22 years (range 10–32; 69% aged 15 years or over). The difference in proportion of VMMC clients aged >15 years between combined ANC/STI clinic referral and community mobilisation was significant at p<0.001.
Of 2483 men accompanying their spouses to the ANC clinic, 1022 (41%) received one-on-one VMMC mobiliser counselling. Of these, 88 (9%) obtained VMMC at Bwaila during data collection. Of 3182 male patients seen at STI clinics, 1997 (63%) received one-on-one counselling. Of these, 242 (12%) obtained VMMC (table 1). This difference in conversion from counselling to obtaining VMMC was significant at p=0.01. In addition to this higher conversion rate, STI clinics also made a greater contribution to total MCs performed at the VMMC clinic (6%) than ANC clinics (2%).
Cascade of VMMC referrals from STI and ANC clinics
In the preintervention period in November 2017–September 2018, Bwaila had performed 3547 VMMCs. For the same period 1 year later, with the intervention under way, 4081 VMMCs were performed, an increase of 534 (15%), of which the 315 clients referred from STI or ANC clinics during the period would represent 59%.
Trends in conversion rate
Figure 2 shows the trends towards increasing overall conversion rates from attending clinic to VMMC. The drops in October coincided with the mobiliser leave taken. The lowest rates were observed in March (3% and 1%); we are not aware of relevant events.

Number of male STI clinic patients and men presenting to ANC and conversion rates to MC at Bwaila, by month. ANC, antenatal care; MC, male circumcision.
Trends in contribution to total VMMCs performed, and relevant external and internal events
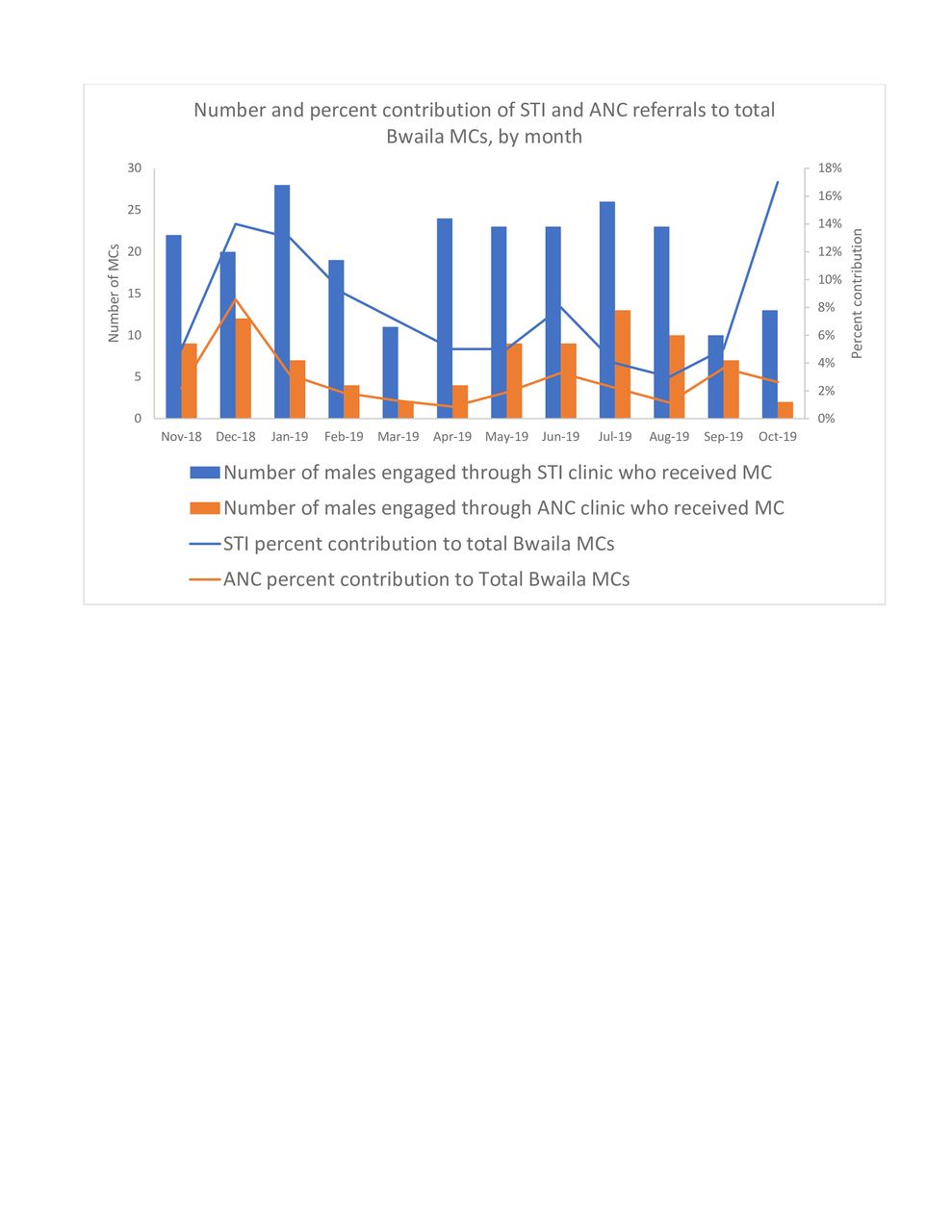
STI clinics contributed more VMMCs than ANC clinics, consistent with the higher number of men seen and counselled and the higher conversion rate (figure 3). Trends in per cent contribution show a peak in December 2018 for both STI and ANC referrals, and even a higher peak for STI referrals in October 2019; this was denominator-driven, as those were the lowest-volume months for the Bwaila VMMC clinic. Conversely, the Malawi VMMC programme conducted campaigns in March–April and July–September 2019, increasing the total number of VMMCs and decreasing proportional contributions of ANC and STI referrals.
{kind=link}
{kind=link}
{kind=link}
Number and per cent contribution of ANC and STI clinic referrals to total Bwaila MC’s, by month. ANC, antenatal care; MC, male circumcision.
Mobiliser time and HIV risk behaviour
Multiple mobiliser schedule changes were made to accommodate changes in client flow and staff holiday and leave. Estimates and attempts at time tracking became insufficiently reliable for analysis.
In total, 291 VMMC clients responded to the risk assessment questions, among 1186 age-eligible clients in March–June 2019, a 25% response rate which counsellors reported resulted from clients’ urgency to complete VMMC after long waits. No difference in risk scores was found by referral source (p=0.517). Only 11% of clients referred from STI clinics reported STI treatment within the past 6 months, although Malawi uses syndromic management, and most clients receive their treatment within the STI clinic. Based on the low response rate and clear inaccuracy of self-report, these data were considered unhelpful.
Discussion
Our findings demonstrate that integrating VMMC referral into STI and ANC services, with VMMC available on-site, can augment demand creation and targeting for men at HIV risk based on age and STI care-seeking history. The programme used readily available resources (mobiliser time and VMMC promotional materials), making it scalable to similar facilities nationwide.
All clients circumcised after referral from ANC and STI clinics were aged 15 years and above, a key achievement compared with standard VMMC community mobilisation. This is presumably because of the age of STI and ANC clinic clientele. HIV incidence modelling has shown that the VMMC programme has greater short-term impact if men aged approximately 15–29 years are targeted, with some variation by country.4 6 7
We did not perform client interviews to investigate reasons for success. Seeking these men and communicating that they are valued clients may have helped address misperceptions that VMMC is for boys. Also, VMMC programmes do recruit new clients from general populations successfully each year; our efforts may have had typical effectiveness while being better directed at crucial populations. Higher VMMC uptake in patients with STI may also result from high self-perceived HIV risk; preventing STIs and HIV is a motivator for VMMC.25 26
The presence of a mobiliser on-site may also have been crucial. Malawi has severe nurse and clinician shortages27; involving lay cadres ensured potential clients received VMMC counselling, which overburdened healthcare workers might be unable to prioritise. Conversely, when the mobilisers were absent, referrals (or at least documentation) plummeted, as most clearly seen in October 2019.
Finally, having co-located intake and destination clinics, with dedicated spaces, probably enhanced success. Most district hospitals and community rural hospitals in Malawi have similar set-ups.
The single-digit per cent contributions made to overall VMMC performance and the single-digit conversion rates should be interpreted in light of the typical annual progress of VMMC programmes. A recent review using data from the Demographic Health Survey, AIDS Indicator Survey, Multiple Indicator Cluster Survey and others28 found that over 2008–2017, the first decade of large-scale VMMC in sub-Saharan Africa, MC coverage among men aged 15–49 years in VMMC priority countries on the first administrative unit level rose by a median of 15% (range 1.0%–22.9%), or less than 2% per year. Increasing coverage through VMMC is a slow, steady process. In this context, increasing coverage of a group expected to have extraordinarily high risk (current STI clients at the major public hospital in Malawi’s capital city) by 8% in a single-year intervention is meaningful progress.
Limitations
The most notable limitation is the unavailability of formal preintervention ANC/STI clinic referral cascade data for comparison. However, at ANC clinics, preintervention VMMC referral can safely be considered non-existent; it is not standard or nationally recommended. At STI clinics it is encouraged and the national STI register can capture it, but at Bwaila it was rarely documented (10 clients in October–December 2017). The large drops in referrals when VMMC mobilisers were absent during the study period also make substantial preintervention referral seem unlikely.
The true conversion rate, VMMCs obtained among all uncircumcised men attending the clinics, could not be calculated because mobilisers did not determine circumcision status among men who did not meet them for one-on-one counselling. Our ‘overall’ and ‘partial’ conversion rates represent lower and upper bounds for this value, respectively. MC coverage in Malawi remains low, with the last Demographic Health Survey reporting 72% of men aged 15–49 years nationally and 81.2% of men aged 15–49 years living in Lilongwe City29 as uncircumcised by self-report in 2015–2016. If these findings apply to the male populations seen in the ANC and STI clinics, the true conversion rates were nearer 5% (ANC) and 10% (STI).
The lack of accurate mobiliser time tracking prevents determining our approach’s time efficiency. However, transportation is a major mobilisation cost in some settings and, with vehicle breakdown or diversion, is sometimes unavailable. The risk behaviour data were similarly unhelpful. We believe it remains likely that potential VMMC clients referred from STI clinics are at high risk of acquiring HIV.
The intervention effect may be underestimated due to censoring. Some men referred from ANC clinics reported wanting to wait on VMMC until their partners delivered.
Finally, it is unknowable how many men circumcised through this clinic-based intervention would have been circumcised anyway through existing community outreach efforts. However, most of Bwaila’s year-over-year performance increase was accounted for by ANC/STI referrals, suggesting these made unique contributions.
Conclusion
This quality improvement project effectively recruited men aged 15 years and above to VMMC and is replicable where ANC and STI services are near VMMC services. Total numbers and conversion rates were sufficient to be meaningful for high-risk subpopulations, particularly in STI clinics.
Key messages
Voluntary medical male circumcision (VMMC) programmes protect men against HIV and several STIs, but reaching those at highest short-term risk for HIV remains challenging.
In Malawi, we implemented WHO guidance in a novel manner by recruiting such men from STI and antenatal care (ANC) clinics to VMMC services.
This approach successfully recruited VMMC clients, totalling 6% (STI) and 2% (ANC) of the total VMMCs performed, and should be replicable in similar settings.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Ethics approval
This project was conducted as programme improvement consistent with WHO guidance, under a non-research determination by the CDC Human Subjects office.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Joseph D Tucker
Contributors WM, SMD, NF and MH initiated the idea and oversaw all implementation. GM directed implementation on the ground. HG, NB and MK provided additional implementation oversight. FS, MB, SS and AM performed data analysis and quality control. CT, CL, EK and AA provided intellectual input on the manuscript. AB, SJPP, KD, ML and Alinafe Mbewe were directly responsible for executing implementation and data collection. SMD and WM are responsible for the overall content as guarantors.
Funding This work received funding from the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC) under the terms of GH001469. CDC funders initiated, designed and participated in the analysis of this project.
Disclaimer The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.