Article Text

Abstract
Objectives Patient and public involvement (PPI) in research priority-setting remains limited, especially for non-HIV STI. We identify and compare the top 10 patient and public STI research priorities with those of clinicians and STI stakeholders.
Methods This two-stage study was conducted in May–August 2019. First, STI research priorities were canvassed through qualitative questionnaires issued to all patients attending a large sexual health clinic, all clinicians in region-wide mailing lists, all stakeholders identified through existing networks and the Charity Commission database, and to the Liverpool public. Raw responses were organised by theme into a shortlist of 25. In stage 2, these were ranked through priority-setting activities by telephone with patients and the public (n=8) and some clinicians (n=3), and in two workshops with clinicians (n=26) and stakeholders (n=5), respectively. The top 10 priorities were compared.
Results Of 373 surveys submitted, 106 were analysed (83 patient and public; 23 clinician and stakeholder). Exclusions included lack of completion and responses out of scope. Among patient and public respondents, 55% (n=46) were aged 18–24 years, 51% (n=42) identified as heterosexual women and 23% (n=19) as men who have sex with men. Clinicians included all cadres; stakeholders were academics, commissioners and third sector representatives. In stage 2, 4 of 10 themes (STI education, targeted services for high-risk groups, antibiotic resistance and counselling for those with STI) were prioritised by all. Remote STI services and rapid diagnostics also ranked highly but the rationale differed between groups.
Conclusion This is the first non-HIV STI research priority-setting exercise to be reported in the UK. It identifies overlaps and differences between public and provider concerns, highlights gaps in the public understanding of STI research, and shows how PPI can promote research responsive to the concerns of both those who use and deliver services.
- health services research
- patient participation
- sexual health
Data availability statement
Data are available upon reasonable request. Anonymised data are available on reasonable request from AIO (ORCHID ID: 0000-0001-6801-8889).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Non-HIV STI pose a significant risk to public health in England. In addition to the specific threat of multidrug-resistant gonorrhoea, overall rates of gonorrhoea, syphilis and chlamydia are rising.1 STIs are therefore an important research priority. Involving patients, the public and other key stakeholders or ‘end-users’ in research priority-setting (RPS) is an important means of optimising research impact by ensuring that studies address the issues which end-users feel are most pressing.2–4
Despite this and the increasing use of patient and public involvement (PPI) in HIV RPS,5 evidence of PPI in non-HIV STI RPS is limited. Instead, laypersons are more commonly advisors or collaborators in research that is already funded.6 Transparent reporting of PPI methodology within this is rarer still. Previous studies have used a modified Delphi process for bacterial STI research priorities in Canada7 and explored multidrug-resistant gonorrhoea priorities using focus group discussions with an international expert panel on STI.8 A further opinion piece identified global STI priorities but did not describe PPI.9
We report the first exercise of its kind in the UK which aimed to identify the top 10 STI research priorities through rigorous, iterative RPS involving patients, the public, clinicians and STI stakeholders. Our priority-setting exercise was conducted in the North West (NW) of England as defined by the National Institute for Health Research NW Coast Clinical Research Network region (Cheshire, Merseyside, Lancashire and Cumbria), which excludes Greater Manchester. The NW has the highest incidence of new STI in the UK outside London.10
Methods
A two-stage study was conducted using a validated approach.3 11 Priorities were first captured via a qualitative questionnaire and ranked to form a shortlist in stage 1, before interactive priority-setting in stage 2 through workshops and interviews to create a final top 10 among specific groups.
Stage 1
In May 2019 four categories of individuals were invited to participate in the questionnaire through (1) waiting room posters and paper questionnaires offered to all patients attending a large integrated sexual health clinic; (2) emails to all clinician members (nurses, healthcare assistants, health advisors and doctors) of the Cheshire and Mersey branch of the BASHH and to all lead clinicians in sexual health clinics in the study area; (3) emails to NW stakeholders (eg, support centres and advocacy groups) identified through existing collaborator networks and the 2019 Charity Commission database12; and finally (4) an open call to boost recruitment from the Liverpool public through stakeholder newsletters, social media and flyers at a local university. Minority groups such as black, Asian and minority ethnicities (BAME), lesbian, gay, bisexual and transgender (LGBT), and refugee communities were targeted through stakeholder networks. Persons aged below 18 years and not resident or working in the NW were not eligible. Invitations included a Quick Response (QR) code to the questionnaire, participation information and a request to forward the information on to staff and/or service users.
Participation was voluntary and the questionnaire, available in identical paper and online formats, followed the James Lind Alliance (JLA) model.11 First, respondents were asked what they understood by the term STI and then to list research priorities from their own perspective under predetermined overarching categories: STI prevention, STI causes, STI diagnosis, STI treatment and care, STI service delivery, and other. Identifiable information was not collected. Participants could volunteer email or phone details as consent to be contacted regarding stage 2. This information was stored separately from survey responses to maintain anonymity.
An initial pilot questionnaire among patients and the public highlighted a potential lack of common understanding of the concept of ‘research’ and how subgroups may interpret the same item differently. Questions were refined to improve focus on research rather than personal or service queries. Public understanding of research was further explored during interviews.
Questionnaires which did not include at least one STI research priority or only included priorities out of scope (eg, questions that had already been clearly addressed) were excluded. Analysis was conducted by HLB and reviewed by senior authors to ensure integrity.
Patient and public (P&P) responses were analysed together, as were clinician and stakeholder (C&S) data. P&P priorities were further stratified by gender, sexual orientation and age to allow comparative analysis.
Where respondents identified multiple priorities, each item was considered as a ‘raw submission’. Raw submissions were analysed using a mix of thematic analysis13 and the JLA Data Management Framework11 to induce recurring STI research priority themes. Data saturation was achieved when no new themes emerged. The number of raw submissions for each STI research priority theme was calculated and used to rank and create a shortlist of 25 research priorities.
Stage 2
Shortlisted priorities were discussed during semistructured telephone interviews with P&P (n=8) and some clinicians (n=3), and two separate workshops for clinicians (n=26) and stakeholders (n=5), respectively. Participants were recruited directly from stage 1 via email or telephone call, and through promotional material, existing stakeholder networks and convenience sampling at a departmental journal club.
Each participant was sent the shortlist prior to the interview/workshop. Both interviews and workshops were facilitated by HLB to ensure consistency and followed a similar structure (to JLA methodology using an interactive, modified nominal group technique11) to group the shortlist into high (2 points), medium (1 point) or low (0 point) priority categories. This was done independently during interviews and within small groups in the workshops. Priorities were allocated a score depending on their grouping as described above, and aggregate scores from all interviews and workshops were calculated for each priority. Overall scores were used to identify and rank the final top 10 STI research priorities for P&P and C&S, respectively. Interviews and workshops were recorded, anonymised and transcribed with consent. Thematic analysis identified and explored similarities and differences between participant groups and their respective justifications for prioritisation. P&P interviews also explored participant understanding of the concept of research and its perceived relevance and importance to them as individuals.
All participants gave informed consent before taking part.
Results
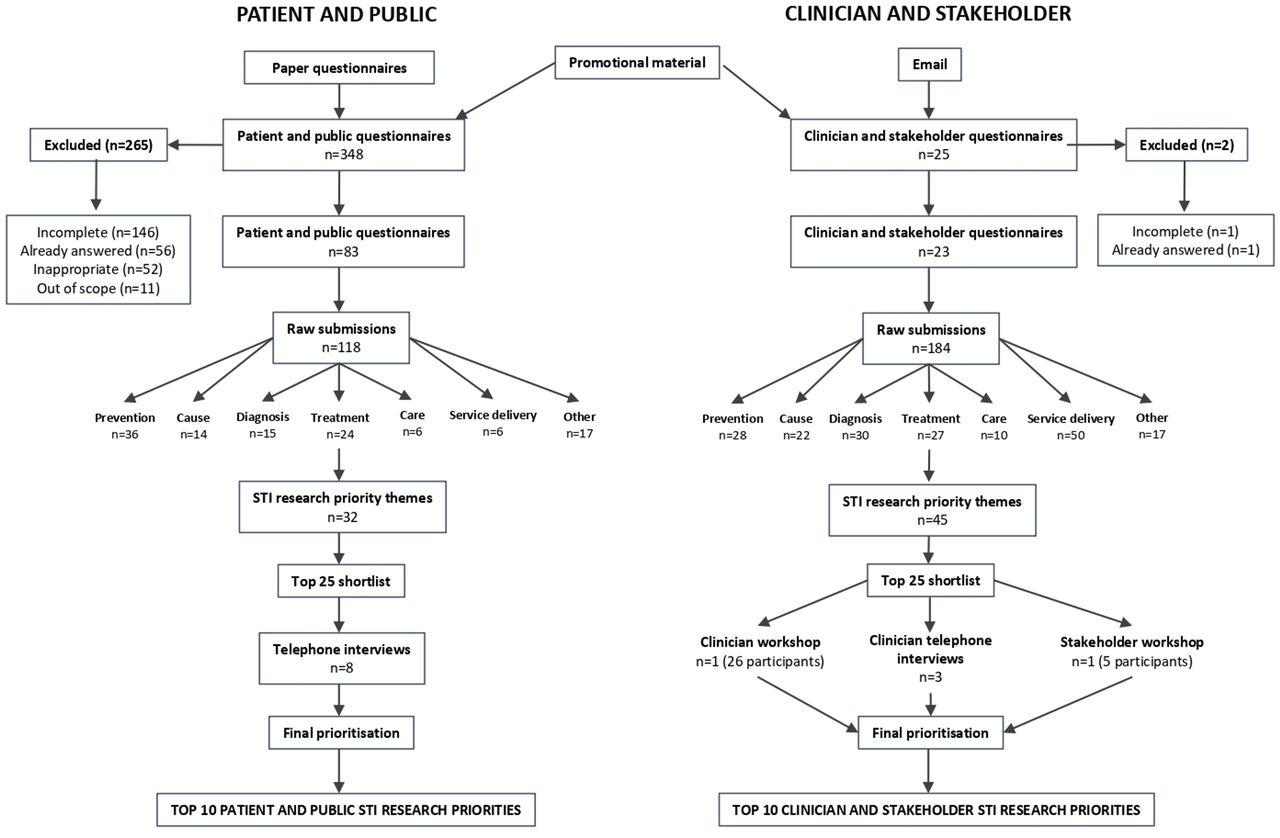
In total, 373 questionnaires were returned (348 P&P; 25 C&S), of which 226 (60.6%) answered one or more questions. Of these, 52 were inappropriate, for example, “Use a condom!” (D28); 11 were out of scope, for example, “Where did STIs come from?” (D25); and 57 were already answered, for example, “Can you catch genital warts if the person who has them isn’t having a flare up?” (D42) and therefore excluded. The remaining 106 (83 P&P; 23 C&S) were analysed (figure 1).

Flow of data outcomes.
Among P&P, 55% (n=46) were aged 18–24 years, 24% (n=20) aged 25–34 years and 19% (n=16) aged 35+ years. Half (51%, n=42) identified as being heterosexual women, 23% (n=19) as men who have sex with men (MSM) and 18% (n=15) as heterosexual men. Only one respondent identified as a bisexual woman or a lesbian, respectively.
Among C&S, 57% (n=13) were doctors, 17% (n=4) were representatives from third sector organisations including those who support commercial sex workers and those living with HIV, 9% (n=2) were nurses, 9% (n=2) were commissioners and 4% (n=1) were academics. One respondent did not state their profession. Of C&S, 74% (n=17) were female, 78% (n=18) were aged 35+ and the distribution of sexual orientation was similar to P&P.
Stage 1
The 118 raw submissions from P&P were coded into 32 STI research themes and 184 from C&S were coded into 45 themes. There were 28 themes overall, and 13 of the top 25 shortlists were the same or similar for each group (figure 2).

Details and distributions of all STI research priority themes identified from the surveys. Priorities marked with an asterisk (*) featured in both top 25 shortlists. HPV, human papilloma virus; HSV herpes simplex virus; MSM, men who have sex with men; PrEP, pre-exposure prophylaxis; SRE, sex and relationship education.
Among the P&P responses, all genders prioritised research into STI prevention measures other than condoms, rapid diagnostics, prevention of human papilloma virus (HPV), and more focus on STI health promotion and sex and relationship education (SRE). Men appeared more likely to call for increased research into STI prevention (57%, n=4 of male priorities compared with 21%, n=5 of female priorities). Women suggested a more diverse array of research priorities, including mental health, tackling STI stigma, STI treatments and drug resistance, and the role of digital service provision.
For MSM, the main priority was STI prevention, with health promotion and gonorrhoea and syphilis antibiotic resistance proving popular. All ages suggested HIV research priorities including pre-exposure prophylaxis, treatment of HPV, STI prevention measures other than condoms and SRE as important research priorities. Rapid diagnostics was the most prevalent in respondents aged 18–24 (72%, n=8 raw submissions).
Stage 2
Among the P&P interviewees, 63% (n=5) were female, 63% (n=5) were aged 18–24 years, 75% (n=6) identified as heterosexual and all were white British. Clinicians were diverse, including nurse practitioners (n=8), consultants (n=5), junior doctors (n=2), nurses (n=6), healthcare assistants (n=5), student nurses (n=2) and health advisor (n=1). Stakeholders included those in leadership roles at local third sector organisations, Public Health England and commissioners.
C&S results were combined to create a joint top 10. STI education, targeted STI services for high-risk groups, STI resistance, and counselling and emotional support feature in the top 10 for both P&P and C&S (figure 3).

{kind=link}
{kind=link}
{kind=link}
Top 10 STI research priorities for the North West by respondent group. Overlaps between the two lists are highlighted in grey. HPV, human papilloma virus; HSV, herpes simplex virus; PrEP, pre-exposure prophylaxis.
STI health promotion and SRE are separate for P&P but combined under ‘STI education’ for C&S. C&S considered STI education in the broader sense with a focus on STI health promotion and fewer survey responses specific to SRE. For P&P, SRE in schools was a separate focal point from the outset and during the priority-setting; the two priorities were continuously examined as separate entities.
Regardless of background or expertise, a focus on “prevention is always better than treating” (PI5) was evident, with STI health promotion and SRE highly prioritised. Most P&P interviewees argued that SRE should be “absolutely compulsory” (PI1), age-appropriate, inclusive and “more representative of a healthy sexuality rather than… the physical aspects” (PI2). Clinicians felt that health promotion research would have a profound impact on “risk reduction, [decreasing] harm and patients having the best sexual health” (C2).
Targeted STI services for high-risk groups was another priority. Similar examples were given by all participant types, such as those with learning and physical disabilities, the elderly, young people, commercial sex workers, “BAME, refugee and asylum-seeking communities and LGBT people especially the trans community” (SH1).
STI antibiotic resistance was the third most important P&P priority and over half (57.1%) of clinicians voted it as one of their most urgent. P&P clearly felt that “Mental health is a priority” (C1). Most interviewees in this group ranked counselling and emotional support as a high or medium priority and C&S also supported this with regard to late HIV diagnoses.
Although they did not appear in both top 10s, the importance of other key themes was repeatedly highlighted in both data sets. Rapid diagnostics with respect to increasing efficiency in clinic, point-of-care tests for chlamydia and gonorrhoea, and understanding risk-taking and sexual behaviours such as chemsex and dating apps to “stem the flow” (SH4) also featured.
Conflicting perspectives emerged in relation to remote STI services and a digital approach to service delivery. Most C&S prioritised research into online services and home testing kits, whereas P&P voiced concerns over their accuracy and safety.
Given the abundance of existing HIV RPS and participatory research with those living with HIV, our intention was to create a space for discussing non-HIV STI. Despite the explicit focus on non-HIV STI in study materials, HIV priorities proved popular and were linked with counselling, emotional support and mental health.
Finally, of note, there was clear enthusiasm for PPI in RPS across groups, with several respondents commenting on how pleased they were to have been given the opportunity to participate.
Discussion
Principal findings
To our knowledge, this is the first intentionally non-HIV STI RPS exercise in the UK. It therefore extends the literature on public engagement in non-HIV STI research.
STI health promotion and education, targeted services for high-risk groups, STI treatment resistance, and counselling and emotional support were among the top 10 priorities across all groups. The high priority given to STI antibiotic resistance is unsurprising given publicity surrounding increasing prevalence, especially for gonorrhoea.10 However, this was outranked by preventative activities including health promotion and education. Indeed participants evidenced nuanced understanding of prevention activities, calling specifically for research exploring risk-taking and sexual behaviours and to develop targeted services and interventions for high-risk groups. Mental health was another important priority, with counselling and emotional support ranking highly and stimulating rich discussion throughout.
Despite these shared priorities, there were significant differences between groups throughout. Although research into the role of rapid diagnostics and digital approaches to STI service delivery were repeatedly prioritised, views on the safety of the latter diverged markedly between and within participant groups.
As expected, P&P differed from C&S in their familiarity with research. C&S developed more specific research questions, more submissions overall, and were more likely to prioritise impact and effectiveness research and translation of research priorities into practice. P&P submitted more general priorities, reflected on personal experiences, submitted more disease-focused topics, and requested more innovation and developmental research. All but two of the surveys that were excluded from analysis because the research questions were already answered belonged to P&P. This highlights the need for more public and patient education on the nature of research and on currently available research evidence. However, all participants regardless of background or familiarity with research were keen to be involved in setting the research agenda and proved passionate about improving STI care.
Strengths and limitations
Use of validated methodology,3 11 including stratified participatory approaches, ensured P&P voices were adequately heard. Every effort was made during stage 2 to ensure that a fair, deliberative consensus was reached.
However, despite widespread dissemination of promotional material, for logistical reasons, the majority of participants were recruited through a single large urban sexual health clinic and the number of C&S is small; this increases risk of bias, limits generalisability and precludes identification of significant differences between age and gender groups. Challenges in scheduling meant that the majority of clinicians in the workshop worked for the same National Health Service trust. The fact that this is the largest STI service provider in the NW ensures representation of a key constituency, but means that more remote and smaller clinics are likely under-represented. Despite these limitations, our study size is comparable with published RPS studies in other disease areas.14–16
While telephone interviews are comparable with inperson interviews,17 there was no opportunity for interaction between P&P participants in stage 2 and subsequent generation of the rich discussion seen in the C&S workshops. Conversely, given the sensitive nature of STI, P&P may have appreciated the opportunity for private discussion.5 18 19
Despite our efforts, minority groups were under-represented in stage 2, which further limits the generalisability of the findings. This lack of representation is not uncommon and has been noted as a barrier to PPI in many areas of research.5 20 Finally, limited understanding of the nature of research and the current state of STI knowledge meant that a large number of P&P responses were ineligible.
Comparison with other studies
Reports of STI RPS exercises are few. Our priorities are similar to those identified in Canada’s STI RPS exercise7—antimicrobial resistance, point-of-care tests for hard-to-reach groups, education in schools and targeted prevention activities—and are similar to those discussed in an international RPS exercise for multidrug-resistant gonorrhoea.8
A recent reflection on case studies on PPI in sexual health research6 advises that researchers should be flexible and adaptive and use creativity to ensure meaningful PPI. The authors suggest that PPI earlier in the research process, most notably in identifying research priorities, would be advantageous to sexual health research and echoes the purpose of this study. Within their case studies one-to-one discussions were initially preferred by lay participants and affirms our decision to use telephone interviews with P&P. We feel this may have boosted recruitment and ensured participants remained comfortable. McDonagh et al 6 describe difficulties engaging potential end-users and recommend involving stakeholders as ‘professional proxies’ to gain insight into the needs of hard-to-reach, target populations, which are traditionally more difficult to access. This further supports our strategy of working synergistically with stakeholders throughout this study.
Our research methods have been clearly documented to ensure transparency and enhance trustworthiness. To date this has been rare in priority-setting research16 and facilitates both replicability of the methods and development of strategies to address limitations in future research.
Conclusions
Until now, the P&P voice has typically been absent from STI RPS despite the public health importance of STI and the role of PPI for good research practice. This study addresses this gap by (1) identifying the top 10 STI priorities for STI research for C&S and for P&P, respectively; (2) demonstrating that large-scale PPI is feasible in STI agenda setting, although additional efforts are needed in improving public understanding of research and coverage of minority and vulnerable groups; and (3) by showing that while there is significant overlap between priorities, there are differences which highlight the need for inclusion of P&P perspectives in priority-setting. This must be supported by P&P education about the nature of research and the current state of STI knowledge if PPI is to be optimised.
Key messages
This is the first published UK STI research priority-setting exercise and therefore adds to the limited literature on public engagement in non-HIV sexual health services.
STI education, targeted services for high-risk and vulnerable groups, STI treatment resistance, and counselling and emotional support were the highest research priorities.
Key differences between patient concerns and those of clinicians and stakeholders highlighted the need to ensure patient and public involvement in STI research priority-setting.
Despite sensitivities, patient and public involvement within STI research priority-setting is feasible and ensures that future research better meets the needs of service users.
Data availability statement
Data are available upon reasonable request. Anonymised data are available on reasonable request from AIO (ORCHID ID: 0000-0001-6801-8889).
Ethics statements
Patient consent for publication
Ethics approval
Research was granted ethical approval (ref: 1905) by Liverpool School of Tropical Medicine Research Ethics Committee.
Footnotes
EC and AIO are joint senior authors.
Handling editor Joseph D Tucker
Twitter @dremilyrclarke, @Obasi_TropMed
Contributors EC conceived the idea for the study and all authors contributed to study design. HLB was the lead researcher, facilitated and conducted the research, and prepared early drafts of the paper. AIO and EC supervised HLB throughout and reviewed raw data and subsequent analysis. HLB prepared the final manuscript with contributions from both AIO and EC. AIO is the manuscript guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. All authors read and approved the final draft.
Funding This study was supported by a grant from the NIHR North West Coast Clinical Research Network. The grant was £3200 from end of year overflow funding for 2019 and was not allocated a grant number.
Disclaimer The funder had no role in the study design, data collection, data analysis, data interpretation, writing of the report or in the decision to submit the article for publication. All authors confirm that they worked independently from funders. All authors had full access to all of the data (including statistical reports and tables) in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.