Article Text

Abstract
Objectives Participation in HIV prevention trials could trigger risk compensation among participants. We evaluated potential risk compensation following use of a vaginal ring microbicide by women in a phase III trial in southwestern Uganda.
Methods We used markers of sexual risk behaviour documented on standardised questionnaires, tested for STIs at baseline and quarterly for 2 years. Risk compensation was defined as a significant increase (trend p<0.05) in the proportion of women reporting risky sexual behaviour or a diagnosed STI between baseline and end of follow-up.
Results Between September 2013 and December 2016, 197 women (active arm: n=132 and placebo: n=65) were enrolled at the Masaka site. There were decreases in all markers of sexual risk behaviour with statistically significant decreases in only the proportion of women reporting ≥2 sexual partners, p=0.026 and those diagnosed with Trichomonas vaginalis p<0.001 and or Neisseria gonorrhoeae p<0.001
Conclusions No evidence of risk compensation was observed in this trial.
Trial registration number NCT01539226.
- HIV
- sexual behaviour
- vaginal microbicides
- women
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Although various prevention options are known, HIV remains a global challenge with 1.7 million new infections seen in 2018.1 Despite all efforts, women and girls continue to be disproportionately affected by HIV/AIDS in sub-Saharan Africa, where they contributed to 59% of new adult HIV infections in 2017.2 Cultural challenges about sexuality and gender norms have a huge impact on the ability of women to prevent HIV and make their own informed decisions about their sexual and reproductive health lives.3 There is therefore urgent need for HIV prevention tools that women can use to prevent themselves from acquiring HIV.4 Vaginal ring microbicides may be a potential prevention tool for women at high risk of HIV acquisition.5
Two pivotal phase III trials on the dapivirine vaginal ring (DVR) showed that the self-inserted ring was safe and could provide HIV risk reduction of up to 30%.6 7 However, data on sexual behavioural changes following use a DVR microbicide are sparse. Concerns on increased sexual risk behaviour have been raised with other prevention strategies like circumcision, condoms and oral pre-exposure prophylaxis (PrEP). Similarly, there are concerns of whether use of the DVR, a risk reduction technology, may potentially result in unintentional increase in sexual risk behaviour among women, a phenomenon defined as risk compensation.8 9 The theory of risk compensation suggests that individuals may modify their behaviour in response to changes in their perceived level of risk.10 11 The theory has been posed as an explanation for limited population-level impact of condom promotion on HIV in communities with generalised epidemics.12 It has also been thought to result in increases in sexual risk behaviour corresponding to the introduction of highly active antiretroviral therapy.13 Studies of efficacious HIV options such as condoms, circumcision and oral PrEP have provided information on risk compensation, with majority showing no increase in risky sexual behaviour following use or widespread uptake.14 15
Studies on oral PrEP among women have provided mixed results. One study showed that taking oral PrEP would result in reduced condom use,16 while a study in Ghana showed no indication of increase in risky sexual behaviour.17 Literature shows that risk compensation may be a concern for specific subpopulations, such as young women and female sex workers on oral PrEP as they may believe that they are fully protected and may participate in riskier sexual behaviours resulting in increased HIV exposure.18 Of major concern is that risk compensation has been feared to reduce the impact of HIV prevention tools on HIV incidence.14 19 Early adopters of oral PrEP have been reported to engage in riskier sexual behaviour (condomless anal sex) with fears of oral PrEP failing to reduce HIV incidence among some key populations like men who have sex with men (MSM).20 21
Majority of studies on risk compensation have been done among women using oral PrEP with none among women using the DVR. It is thus crucial to understand whether DVR use could result in risk compensation among women at high risk of HIV acquisition. Documenting this information would provide an insight to service providers during roll out of the DVR. We therefore evaluated potential risk compensation using self-reports of sexual risk behaviour and STI rates in women participating in a phase III DVR trial in southwestern Uganda.
Methods
Study setting
The Ring Study was a randomised, double-blind, placebo-controlled, phase III, multicentre trial that evaluated the safety and efficacy of the DVR in healthy, sexually active women enrolled at seven research centres in South Africa and Uganda from 2012 to 2016. Participants were assigned, in a 2:1 ratio, to receive either the DVR, containing 25 mg of dapivirine dispersed in a platinum-catalysed silicone matrix or a matched placebo ring. Both groups received the standard HIV prevention package per prevailing national guidelines. Each woman self-inserted a vaginal ring every 4 weeks, for up to 24 months of follow up.6
In Uganda, The Ring Study was conducted at a research centre in Masaka by the Medical Research Council/Uganda Virus Research Institute and London School of Hygiene & Tropical Medicine, Uganda Research Unit in collaboration with the International Partnership for Microbicides. The Masaka research site in southwestern Uganda, 120 km from the capital Kampala was part of a larger trial that took place in Uganda and South Africa. Masaka district is a commercial centre and resting point for cross-border truck drivers, thus creating a demand for commercial sex. HIV prevalence in Masaka district is about 11.1%, with the prevalence of HIV among women being 12.9% compared with 8.6% in men.22
Study population
Details on the recruitment of women into The Ring Study in southwestern Uganda have been previously described and published.23 Briefly, the research site enrolled 197 women at high risk of HIV infection between September 2013 and December 2016. High risk was defined by the research centre by presence of any two of the following: (1) history of STIs in the past 3 months; (3) self-reported condomless sex with multiple sex partners or a new partner in the past 3 months; and (3) use of recreational drugs (marijuana and alcohol) in the past 3 months.
A woman was included in the main study if she was asymptomatic for genital infections at the time of enrolment. If a woman was diagnosed with any clinically significant curable STI, she must have initiated treatment at least a week prior to enrolment and have completed the full course of treatment. At the enrolment visit, eligible women were randomised to receive a DVR or placebo ring and were counselled to use the ring daily for 28 days. Monthly visits were conducted to provide all participants with counselling on HIV risk reduction, male condom use and adherence to ring use.
Data collection
Data on participants’ demographics were collected at the screening visit, while data on sexual behaviour were collected at the enrolment visit (baseline) and every 4 weeks for 2 years using standardised questionnaires. Questionnaires on sexual behaviour had specific questions on: number of male sexual partners participants had had, number of coital acts at baseline (first 4 weeks), then every 24 weeks for 2 years.
Laboratory tests
Testing for STIs was carried out at baseline and every 12 weeks thereafter for up to 2 years. Cervico-vaginal samples were collected by trained study doctors and tested at the research centre laboratory. Samples were tested for Trichomonas vaginalis (OSOM Trichomonas Test, Sekisui Diagnostics LLC, USA), Chlamydia trachomatis and Neisseria gonorrhoea (Cobas Amplicor CT/NG PCR test, Roche Diagnostic Systems, Branchburg, New Jersey, USA). Those who tested positive for STIs were treated following the Uganda national guidelines for syndromic management of STIs24 and the Centers for Disease Control and Prevention (CDC) treatment guidelines for aetiological diagnoses.25
Statistical analysis
Participants’ baseline characteristics were summarised using frequencies and percentages and stratified by trial arm (active vs placebo). Condom use was defined as participants’ self-reporting using condoms with a sexual partner at the most recent sex act. While frequency of condom use was defined as how often a participant reported condom use during vaginal sex. We defined risk compensation as a significant increase (p<0.05) in risky sexual behaviour shown by a positive coefficient in the longitudinal Poisson regression model examining the effect of time on risky sexual behaviour markers. We further provided insight (using χ2 test for trend p<0.05) on changes in the proportion of women reporting high-risk sexual behaviour or a diagnosed STI based on aetiological testing between baseline and end of follow-up using data on visits that happened every 24 weeks. High-risk behaviour was defined as any one of: two or more sexual partners in the past 24 weeks or non-condom use at the last sex act or being diagnosed with an STI including C. trachomatis, T. vaginalis or N. gonorrhoeae.
Compliance with ethical standards
Written informed consent was obtained from women who were willing to be screened and enrolled into the trial. All women diagnosed with STIs were offered free treatment from the research centre and were also given appropriate medication to give to their sexual partners. Those that tested HIV positive during the trial were immediately referred to HIV care and treatment centres of their choice within the community for further management.
Results
Baseline and sociodemographic characteristics
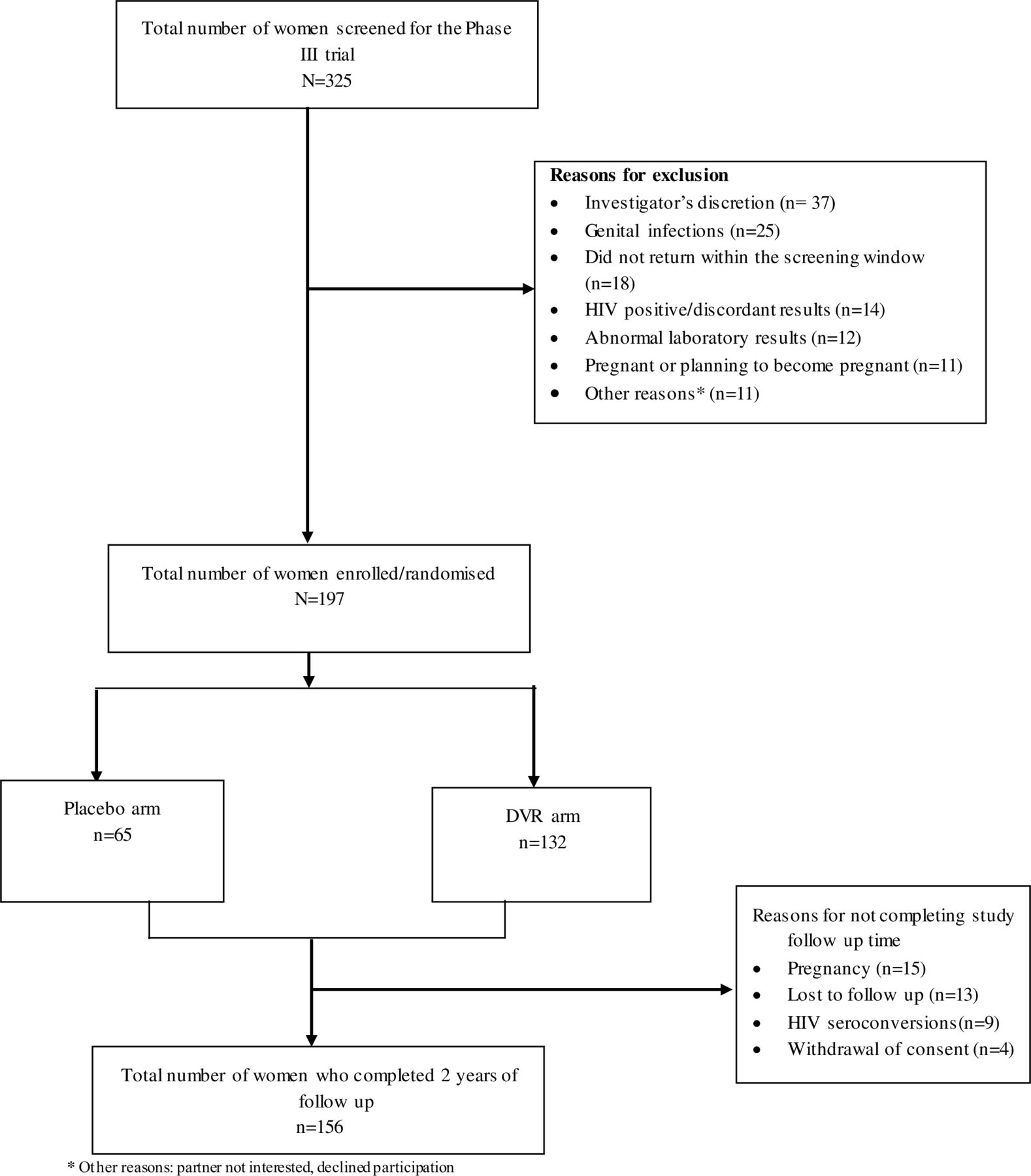
In total, 325 women were screened at the Masaka research centre of whom 197 (60.6%) were enrolled. The primary reason for exclusion were: investigator discretion that is any condition(s) that, in the opinion of the investigator, would put a participant at risk or interfere with the trial objectives or a participant’s adherence to trial requirements (37, 28.9%), genital infections (25, 19.5%), participant did not return within the screening window (18, 14.1%) and HIV positive or discordant results (14, 10.9%) (figure 1). Of the 197 women enrolled into The Ring Study (mean age 28 years, SD=6.6), 67% (n=132) were in the DVR arm (table 1). Of those enrolled, 79% (n=156/197) completed 2 years of study follow-up. The baseline sociodemographic characteristics were comparable between trial arms, except for women with primary education that were slightly more in the placebo arm (61.5%) than DVR (49.2%) and those with secondary education were more in the DVR (14.4%) than placebo arm (7.7%) (table 1).
Baseline and sociodemographic characteristics of 197 women enrolled into a phase lll microbicide trial in southwestern Uganda (September 2013–December 2014) frequencies, percentages

{kind=link}
Study profile of women screened and enrolled into a phase III microbicide trial in southwestern Uganda (September 2013–December 2014).
Sexual behaviour and STIs
At baseline, more than half, 57.4%, reported two or more sexual partners, and nearly one-third (36.4%) reported never using a condom while having sex with these multiple sexual partners. Approximately two-thirds, 64.3%, reported non-condom use at the last sex act. Furthermore, 1 in 10 women, 11.4%, were diagnosed with C. trachomatis, while about one-third (36.4%) had T. vaginalis and 12.9% had N. gonorrhoeae (table 2).
Proportion of women with risky sexual behaviour at baseline and every 24 weeks of follow-up
Assessment of risk compensation
Generally, there were decreases over time in reported risky sexual behaviour at the end of follow-up, with statistically significant decreases reported for number of sexual partners (p=0.026, table 2). Similar decreases over time were seen among women diagnosed with STIs, with statistically significant decreases seen among women diagnosed with T. vaginalis, p<0.001, and those diagnosed with N. gonorrhoeae, p<0.001.
Table 3 shows the average change in risky sexual behaviour throughout follow-up and the rate ratio associated with this change estimated at every 4 or 12 (for STIs) weeks increment in follow-up time up to 104 weeks. There was a decrease in any STI diagnosis of 15% equivalent to a rate ratio of 0.86, 95% CI 0.83 to 0.90, p<0.001. It was generally observed that there was a decrease in the diagnosis of individual risky sexual behaviours achieving statistical significance of p<0.05 for T. vaginalis and N. gonorrhoeae.
Slopes of average change in a given risky sexual behaviour over follow-up and rate ratio for every 4 or 12 (for STIs) weeks increase in follow-up
Discussion
In this analysis, we assessed for evidence of risk compensation among women participating in a DVR trial. We found no evidence that vaginal ring use led to greater risk taking behaviour in participants enrolled in Uganda, a finding that is similar to what has been seen with other studies on oral PrEP,26–31 medical male circumcision14 32 33 and vaccines.34 There was an overall shift towards safer sexual behaviour as shown by the progressive decline in STIs among women at risk of HIV infection from baseline to the end of study participation. Significant reduction occurred for T. vaginalis and N. gonorrhoea. This could have been due to continuous counselling and quarterly testing for STIs. Counselling and testing have been shown to support reduction in high-risk sexual behaviour.26
Our study also found a modest decline in the number of sexual partners over time. This is contrary to what has been seen in other HIV prevention trials where the number of sexual partners reduced over time.11 35 Much as the number of partners declined slightly, there was no significant increase in condom use at last sex act. Previous research on vaginal gels showed that condom use during the last sex act increased over time.31 36–38 This is however consistent with findings from a study that was reported among women in clinical trials where risky sexual behaviour declined.26 Furthermore, this trial mainly recruited women involved in sex trade, and studies of female sex workers in Africa have shown that ‘condomless’ sex attracted better pay.39 This could make acceptance of condom use difficult.
Various studies have reported risk compensation following use of microbicides.19 40 However, this is the first study to look at risk compensation following use of a DVR microbicide for HIV prevention. Second, our analysis included aetiological diagnosis of STIs as a study procedure. Mainly in such a rural setting where there is little or no laboratory services, repeated diagnosis of STIs and collection of sexual behaviour data is sparse. This therefore provided for good markers of risky sexual behaviour.
One of the limitations of our study is that we used data on sexual behaviour that was self-reported. This could have resulted in social desirability bias and recall bias. Second, this analysis was limited by sample size and may not be representative of all women in sub-Saharan Africa, as it was part of the phase III trial that enrolled 1959 women in six other research centres in South Africa. However, these findings may be applicable to women in southwestern Uganda. While the phase III study was double blinded, we did not explore perception of risk among these women in view of an efficacious DVR. Although we collected information on number of sexual partners and type of sexual partner, no additional information was collected. This was mainly because the focus of our study was on sexual behaviour among women who participated in the main study. Our study had 20% of women discontinue study follow-up mainly due to pregnancy, being lost to follow-up and HIV seroconversion. We recruited a high-risk group of women who were provided with contraception and HIV prevention services.
These findings reveal a marked reduction in the proportion of women diagnosed with STIs with a moderate decline in the proportion of those reporting risky sexual behaviour over time. There was no evidence of an increase in risky sexual behaviour or diagnosis of STIs in this trial suggesting that there was no substantial evidence of risk compensation with DVR use.
Key messages
Use of the dapivirine vaginal ring (DVR) for HIV risk reduction does not result in significant increase in risky sexual behaviour.
Regular STI screening among high-risk women is required with the provision of the DVR.
Risk reduction counselling with provision of the DVR remain critically important.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the UVRI Research Ethics Committee (GC/127/13/03/33), Uganda National Council of Science and Technology (HS1362) and National Drug Authority (166/ESR/NDA/DID-07/2013).
Acknowledgments
International Partnership for Microbicides’ (a not-for-profit product-development partnership) work is made possible by generous support from many donors including: the Bill and Melinda Gates Foundation, Irish Aid, the Ministry of Foreign Affairs of Denmark, the Ministry of Foreign Affairs of the Netherlands, the Norwegian Agency for Development Cooperation, the UK Department for International Development, the American people through the US Agency for International Development and the President’s Emergency Plan for AIDS Relief. We would like to thank the study team who worked tirelessly in planning, recruitment and data collection for this study; Sarah Nakato, Beatrice Kimono Washi, Sylvia Masawi, Vincent Basajja, Henry Ssemaganda, Victoria Mugwaneza, Joseph Kitumba, Penelope Akankunda, Aeron Namirembe, Wilson Kakeeto, Paul Taire and Elizabeth Mbabazi Atuhura. We also appreciate Jonathan Kitonsa for providing valuable comments to the manuscript.
References
Footnotes
Handling editor Adam Huw Bourne
Twitter @Kushylvia
Contributors SK, AA, AK and MO designed the study, and AA did the analysis. AK and MO conducted the study, while SK directed the work. JOM contributed to the writing and editing of the manuscript. All authors contributed to the interpretation of the results and critically commented and provided revisions to the manuscript. All authors approved the final version of the manuscript.
Funding The study was funded and sponsored by the International Partnership for Microbicides (www.ipmglobal.org) (IND # 110,659). For this manuscript, the funder participated in study design and manuscript review but had no role in data analysis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.