Article Text

Statistics from Altmetric.com
Introduction
The European AIDS Clinical Society invited this journal and International Union against STI (IUSTI) Europe to host a joint workshop as part of the 18th European AIDS Conference (London, 27–30 October 2021). We covered four themes within four presentations and a panel discussion: trends in bacterial STIs in Europe, the relationship between STIs and HIV, emerging concepts in STIs and standards of STI care in HIV services. In preparation, a brief survey was sent to IUSTI Europe country representatives and members of the Euroguidelines in Central and Eastern Europe (ECEE) network1 to seek their views on current provision and areas for improvement.
Theme 1: trends in bacterial STIs reported to the European Centre for Disease Prevention and Control from the European Union/European Economic Area in 2019
Surveillance of STIs at the European Centre for Disease Prevention and Control
Four bacterial STIs are under surveillance within the European Union/European Economic Area (EU/EEA): chlamydia, gonorrhoea, syphilis (including congenital syphilis) and lymphogranuloma venereum (LGV). Every year, data are uploaded by EU/EEA countries to the European Surveillance System hosted by the European Centre for Disease Prevention and Control (ECDC), in accordance with case definitions for confirmed cases established by the EU2–4 and available in the ECDC Surveillance Atlas of Infectious Diseases.5 In 2019, the number of reported STIs increased by 9% for chlamydia, 55% for gonorrhoea, 25% for syphilis and 75% for LGV relative to 2015 (figure 1; box 1).

Reported cases of bacterial STIs in EU/EEA in 2015 (solid colour) vs 2019 (patterned colour).5 EEA, European Economic Area; EU, European Union; LGV, lymphogranuloma venereum.
Key points on the epidemiology of bacterial STIs reported to ECDC from EU/EEA
Reported numbers of bacterial STIs (chlamydia, gonorrhoea, syphilis, LGV) reached an all-time high in 2019.
Heterogeneity in surveillance systems (comprehensive vs sentinel surveillance, compulsory vs voluntary notification, case based vs aggregated data) and variable levels of reporting completeness must be considered when comparing data across countries. Concerted efforts are needed to harmonise a Europe-wide data collection.
Improved diagnostic capacity (especially for chlamydia and LGV) and expanded testing programmes (eg, for HIV-negative MSM) partially explain increases in STI reporting rates.
Reflecting high screening rates, chlamydia remains the most frequently reported STI; although it is most common in young women, reported cases doubled among MSM between 2015 (13 per 100 000) and 2019 (25 per 100 000).
Reported LGV cases occur predominantly among MSM living with HIV but are increasing among HIV-negative MSM (likely also because of improved case ascertainment).
Reported cases of gonorrhoea are three times more common among men than in women. Young women are a vulnerable group, with a median age at diagnosis of 22 years vs 26 years for heterosexual men and 31 years for MSM.
Syphilis continues to be a largely male-dominated epidemic. MSM account for 68% of cases with information on transmission available, and diagnoses are increasing among HIV-negative MSM. People diagnosed with syphilis tend to be older than those diagnosed with gonorrhoea or chlamydia (median age 36 years for MSM, 35 years for heterosexual men, 29 years for women).
Notifications of congenital syphilis remain low, although the overall notification rate increased from 1.1 to 1.9 cases per 100 000 live births between 2015 and 2019, with some countries reporting disproportionately high numbers.
Underdiagnosis and under-reporting of STIs are anticipated for 2020/2021 due to the COVID-19 pandemic. Factors that are expected to modify STI epidemiological trends include changes in sexual behaviour and healthcare-seeking behaviour, alongside variations in healthcare availability and mode of delivery. More research is needed to understand these effects.
ECDC, European Centre for Disease Prevention and Control; EEA, European Economic Area; EU, European Union; LGV, lymphogranuloma venereum; MSM, men who have sex with men.
Chlamydia
In 2019, 434 184 chlamydia cases were reported by 26 countries. The total notification rate (per 100 000 population) was 157, with rates ranging from <1 (Cyprus, Greece, Romania) to >500 (Denmark, Iceland, Norway). As in previous years, the UK reported ~60% of total cases (a notification rate of 389 per 100 000), which reflects the existence of a national chlamydia screening programme. The male to female ratio in total EU/EEA cases was 0.8:1; 60% of reported cases were in individuals aged 15–24 years, a group which has high incidence of chlamydia and is targeted by testing policies.6 For cases with reported modes of transmission, 82% were in heterosexual women and men and 13% in men who have sex with men (MSM).
Gonorrhoea
In 2019, a record number of 117 881 gonorrhoea cases were reported from 27 countries. The total notification rate (per 100 000 population) was 32, with rates ranging from <1 (Bulgaria, Cyprus, Poland, Romania) to >30 (UK, Denmark, Iceland, Ireland, Malta, Norway, Sweden). The UK reported 66% of total cases and had the highest notification rate of 116 per 100 000. The male to female ratio in the total EU/EEA cases was 3.1:1. For cases with reported modes of transmission, 48% were in MSM, 24% in heterosexual women and 22% in heterosexual men; the prevalence rates of reported HIV infection in these cases were 19%, 0.6% and 1.3%.
Syphilis
In 2019, there were 35 039 syphilis diagnoses reported by 27 countries. The total notification rate (per 100 000 population) was 7.4, with rates ranging from <3 (Croatia, Estonia, Slovenia, Romania) to >10 (UK, Iceland, Ireland, Malta, Spain). The male to female ratio in the total EU/EEA cases was 8.6:1. Considering cases where HIV status was reported, 4% of heterosexual cases and 31% of MSM cases occurred in people living with HIV. While the number of cases of syphilis remained stable in MSM living with HIV during 2015–2019, there was a 44% increase in syphilis diagnoses among HIV-negative MSM. There were 72 notifications of congenital syphilis in 2019. The notification rate for the EU/EEA (1.9 cases per 100 000 live births) fell below WHO elimination target (<50 cases per 100 000 live births). The number of countries reporting cases (among those reporting data) decreased from 17 of 24 (71%) in 2010 to 13 of 25 (52%) in 2019; 6 of 23 countries that reported consistently through the years (Cyprus, Iceland, Luxembourg, Malta, Norway, Slovenia) recorded no cases during 2010–2019. However, the total notification rate increased from 1.1 in 2015 to 1.9 in 2019, and Bulgaria and Portugal reported disproportionately high numbers in 2019 (37 of 72 and 12 of 72 notifications, respectively).
Lymphogranuloma venereum
A total of 3112 LGV diagnoses were reported from 16 countries in 2019, whereas there were 103 cases reported by two countries (UK, Netherlands) in 2004. The increase likely documents an expanding LGV epidemic, but also indicates improving diagnostic capacity. Between 2004 and 2019, 99% of cases with reported modes of transmission occurred in MSM, and 73% of MSM cases with reported HIV status were in MSM living with HIV. Since 2015, in parallel with a sustained increase in the number of LGV cases among MSM living with HIV, data indicate an increase in LGV diagnoses among HIV-negative MSM.7 8 The true magnitude of the epidemic is likely to be underestimated because of the scarcity of routine screening data.
Did the COVID-19 pandemic have an impact on STI notifications?
While the EU/EEA STI surveillance data for 2020 are under validation, initial information on trends can be gathered from national reports, surveys and peer-reviewed publications, including a series of articles hosted by the STI journal9–16 (table 1). A reduction in the number of STI diagnoses coinciding with pandemic-related restrictions on social interactions was reported from many settings, although some reported stable or even increasing numbers. The EuroTEST consortium recently conducted an online survey assessing the impact of the pandemic on testing for HIV, viral hepatitis and STIs during March–August 2020 in the 53 countries of the WHO European region.17 Most respondents reported decreased testing volumes, and many described severe disruptions to testing provision, particularly in March–May 2020 versus the same period in 2019, followed by some improvement in June–August 2020. Current research aims to understand how the pandemic is impacting STI epidemiology and provision of sexual health services, and its effects on sexual behaviour and healthcare-seeking behaviour.18 Data are also needed on the opportunities offered by innovative healthcare approaches, such as provision of e-health services and implementation of self-sampling services for STI testing using postal services.
Trends in diagnoses of syphilis and gonorrhoea (GC) during the COVID-19 pandemic in Europe from reports published in the STI journal—results from a desk review
Theme 2: the relationship between STIs and HIV
Bidirectional interactions between STIs and HIV
STIs that cause inflammation and ulceration may enhance the infectiousness of people living with HIV and increase susceptibility to infection in their partners by directly promoting HIV replication, disrupting the mucosal barrier and attracting activated lymphocytes to sites of exposure.19 20 However, data indicate that antiretroviral treatment (ART) and pre-exposure prophylaxis (PrEP) effectively prevent HIV transmission despite the presence of STIs. HIV continues to modulate the impact of STIs, most notably with human papilloma virus (HPV), which remains an important cause of disease for people living with HIV (box 2).21–24
Key points on the relationship between STIs and HIV
Effective ART and HIV PrEP have weakened the link between STIs and HIV transmission. In settings where most people living with HIV are receiving virologically suppressive ART, and where PrEP programmes are well established for those at risk of HIV exposure, HIV diagnoses can be expected to decline regardless of increasing STI diagnoses.
STI epidemiological data are incomplete for people with HIV. For populations without HIV, STI epidemiological trends serve as a key indicator of the need for HIV PrEP.
There is limited systematic reporting on HIV PrEP programmes across the EU/EEA and data on uptake and impact are incomplete.
Among PrEP users, some subpopulations are at heightened risk of STI acquisition, particularly younger MSM and people who use drugs. Promoting knowledge of HIV and STIs among young people must form an integral part of control programmes.
More data are needed on the efficacy of HIV PrEP in women with STIs and on the efficacy of long-acting injectable PrEP in men and women with STIs.
Clinicians need to be aware of potential self-sourcing of antibiotics for STI prophylaxis among a subset of MSM accessing HIV PrEP.
ART, antiretroviral treatment; EEA, European Economic Area; EU, European Union; MSM, men who have sex with men; PrEP, pre-exposure prophylaxis.
HIV PrEP and STIs
Much attention has been focused on the concept that the availability of HIV PrEP may modify behaviours and increase STI incidence among PrEP users. Data have been somewhat discordant, probably reflecting that PrEP studies tend to be biased by (1) the recruitment of participants who have more frequent STI diagnoses overall, and (2) the probability of more frequent STI screening of participants of PrEP studies than of non-PrEP users. In 2018, a systemic review showed a 24% increase in STI prevalence among PrEP users versus non-users (OR 1.24; 95% CI 0.99 to 1.54).25 In a PrEP trial in Australia in 2016–2018, overall STI incidence was 92 per 100 person-years among 2892 MSM.26 In a subset (n=1378) with pre-enrolment data, starting PrEP was associated with a small increase in STI incidence (adjusted incidence rate ratio 1.12). It has been highlighted that 76% of all STIs in the trial occurred in a fraction (25%) of the overall population19; the factors associated with STI acquisition were those related to sexual behaviour and young age.26 One important dataset comes from the PROUD Study that randomised MSM in the UK to receive PrEP either immediately or after a deferral period of 1 year: in the deferred arm, a history of syphilis or rectal chlamydia or gonorrhoea was associated with a high risk of HIV infection,27 highlighting how STI epidemiological trends can point to the need for PrEP in a population.
An online survey in Ireland aimed to determine the level of knowledge of STI and HIV transmission, testing and treatment in the MSM population.28 As many as 36% of respondents were classed as having lower levels of knowledge. Predictors of lower levels of knowledge were younger age, lack of disclosure of MSM behaviour to contacts and not having visited a national MSM-specific health promotion website. Other interesting observations emerged from an online survey of PrEP users in the UK; among over 1800 MSM, 9% reported taking self-sourced antibiotic prophylaxis for STIs, most commonly doxycycline, usually due to perceiving themselves as being at risk of exposure.29 Whereas there is evidence of the beneficial effect of doxycycline for post-exposure prophylaxis against chlamydia and syphilis,30 current guidance firmly recommends against antibiotic use for STI PrEP.31
ART and PrEP prevent HIV transmission despite STIs
The efficacy of suppressive ART in preventing HIV transmission despite the occurrence of STIs has been confirmed in several studies which recruited heterosexual or homosexual HIV-serodifferent couples, including HPTN 052 (heterosexual couples),32 PARTNER 1 (heterosexual and MSM couples),33 PARTNER 2 (MSM couples)34 and Opposites Attract (MSM couples).35 In PARTNER 2, of 782 gay couples reporting more than 76 000 episodes of condomless anal sex, 27% of 779 partners with HIV and 24% of 779 partners without HIV had an STI over a median follow-up of 2 years.34 Despite this, no episodes of within-couple HIV transmission were detected. Possible reasons include: (1) STI-induced HIV shedding during suppressive ART occurs at low copy numbers, (2) the shed virus is defective or (3) ART has direct prophylactic effects in the anogenital tract.19 In a meta-analysis of surveillance data from HIV-negative MSM attending sexual health clinics throughout England in the period predating HIV PrEP roll-out (2011–2018), HIV incidence rates decreased while rates of rectal gonorrhoea markedly increased.36 Investigators concluded that the effect likely resulted from expanded HIV testing, prompt ART initiation after diagnosis and high rates of virological suppression in people living with HIV. PrEP with tenofovir disoproxil plus emtricitabine is also efficacious in preventing HIV acquisition, despite the frequent occurrence of STIs among PrEP users.19 37 38 In the open-label observational phase of the IPERGAY Study of on-demand PrEP for example, 43% of 361 MSM had ≥1 STI (chlamydia, gonorrhoea or syphilis), yet PrEP led to a 97% relative reduction in HIV incidence over a median follow-up of 18.4 months.37
Theme 3: emerging concepts in STIs
From infection control towards disease control for chlamydia?
Starting from the 1970s, successive breakthroughs in diagnostics helped identify Chlamydia trachomatis as an STI. Subsequent work established that most infections are mild or asymptomatic, although in a small proportion of cases they can lead to pelvic inflammatory disease (PID) and infertility.39 The potential for significant disease and sequelae led some countries to implement extensive screening programmes as part of a ‘test and treat’ approach. Recently, the cost-effectiveness of asymptomatic screening for chlamydia has been called into question,40 reflecting several considerations: (1) PID-related hospital admissions have been declining both in countries with extensive screening programmes, such as the UK and the Netherlands, and in countries that have not adopted such programmes, such as Ireland and Belgium, causing uncertainty about the true population attributable fraction of PID that may be related to chlamydia41; (2) ‘test and treat’ does not seem to translate into reduced chlamydia transmission at the population level; (3) antibiotic treatment of asymptomatic infections may contribute to the spread of antimicrobial resistance; (4) among men, and especially among MSM, chlamydia infection of extragenital and probably genital sites causes low or even negligible morbidity; and (5) at the individual level, the potential benefits of asymptomatic testing need balancing against a potentially negative psychosocial impact, for example, on relationships (box 3).
Key points on emerging concepts in STIs
Through the years, diagnostic innovations have been instrumental in the recognition of new STI aetiologies (eg, chlamydia and LGV). However, in routine practice, use of assays that test for agents lacking a clear role in pathogenesis should be discouraged. Some multiplex assays, in addition to recognised STIs, also report on ‘potential pathogens’ (eg, Mycoplasma hominis, Ureaplasma urolythicum or Prevotella spp). This can create a clinical dilemma as to whether one should ignore a positive result or offer treatment without proven need or benefit.
Screening practices should consider potential downsides of asymptomatic diagnoses, including antibiotic overuse and psychosocial impact. For chlamydia, while scientific debate is reconsidering the net benefits of mass screening programmes, the optimal screening strategies for low-risk populations remain to be defined.
Based on high-genome homology, the current LGV epidemic among MSM is considered a clonal outbreak that spread throughout the world via a highly intertwined, international network of MSM living in and travelling between large urban centres.
The high burden of HPV infection and HPV-related anal cancer among MSM living with HIV highlights the importance of preventing both HIV and HPV acquisition in MSM, including through gender-neutral HPV vaccination. Emerging data also indicate the benefit of detecting and treating anal cancer precursor lesions, pointing to a role for regular high-resolution anoscopy for MSM living with HIV, although this is not yet universally available in many European settings.
HPV, human papilloma virus; LGV, lymphogranuloma venereum; MSM, men who have sex with men.
How is LGV spreading among MSM?
C. trachomatis genovar L – the cause of LGV – is an invasive organism that can cross the mucosal layer and spread to loco-regional lymph nodes, causing severe inflammation. About 75% of infections are symptomatic, presenting with anal and rectal symptoms.42 43 Before 2000, LGV was seen in Europe mainly in heterosexual contacts of people from countries in the equator. Outbreaks affecting MSM in large urban centres followed, initially among people living with HIV but now increasingly among HIV-negative MSM.7 8 Using stored samples, the first evidence of transmission among MSM was traced to the early 1980s in San Francisco. Genome analyses show that the strains causing LGV among MSM in Europe (UK, Netherlands, Spain) are highly similar to those found in major cities in Australia and North America, pointing to a clonal origin of the epidemic.44
When to screen for Mycoplasma genitalium?
Mycoplasma genitalium is sexually transmitted and is associated with urethritis in men. An association with other urogenital manifestations, including cervicitis and PID in women, is proposed, but understanding of the natural history of the infection is incomplete.45 Most people are asymptomatic and widespread asymptomatic screening is not recommended.46 In addition, M. genitalium is highly prone to antimicrobial resistance, limiting therapeutic options for symptomatic infections and raising concerns about the emergence of untreatable strains. Diagnosis requires access to molecular assays and a characterisation of resistance. IUSTI is developing guidelines indicating that testing should be primarily directed to people with specific syndromes.46
How can anal cancer be prevented in MSM?
In a meta-analysis of data from 29 900 men, prevalence of anal HPV16 and other high-risk HPV types was highest in MSM living with HIV, lower in heterosexual men living with HIV and in HIV-negative MSM, and lowest in HIV-negative heterosexual men.22 HIV infection and HIV-related immunosuppression were also significant predictors of anal high-grade squamous intraepithelial lesions (HSILs). These data are consistent with a previous meta-analysis showing a strikingly increased risk of anal cancer among MSM, which was associated with HIV infection as well as older age.23 MSM living with HIV have nearly 100-fold higher risk of anal cancer relative to HIV-negative MSM, and the risk is increased with low nadir CD4 cell count, alcohol use and smoking, whereas virologically suppressive ART has a partially protective effect.24 Results were recently announced from the phase 3 ANCHOR Study, which randomised just over 4000 people living with HIV who had anal HSIL to either immediate treatment of the lesions or observation.47 The study was terminated early due to the observation that immediate treatment significantly reduced the incidence of anal cancer. The data indicate a role for screening (by high-resolution anoscopy) MSM living with HIV as a key strategy to prevent anal cancer.
Theme 4: standards of STI care in people living with HIV
A survey of standards of STI care indicates considerable variation and room for improvement
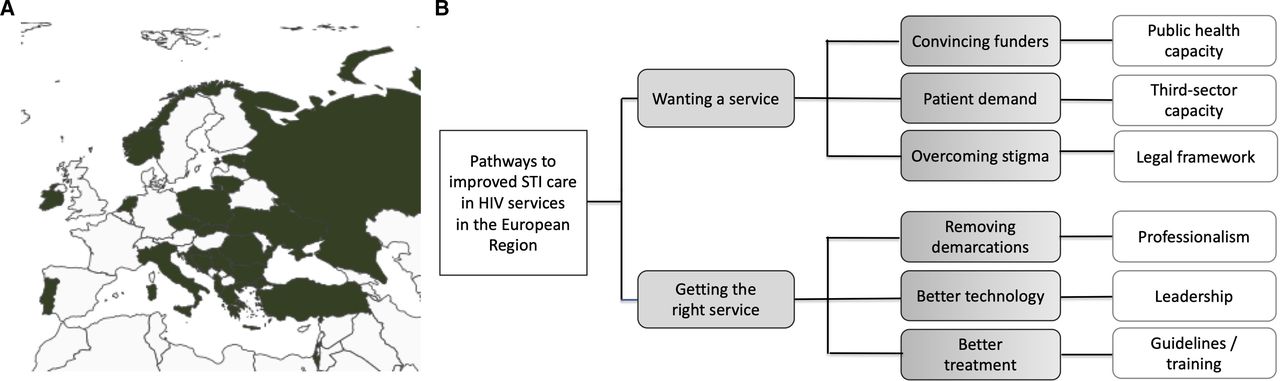
When managing STIs within HIV services, it is important that practitioners are familiar with practice guidelines. However, familiarity with practice guidelines is not sufficient for situations in which individuals are unable to access a service or appropriate diagnostic test. These matters pertain to service standards, which consider areas such as overall service quality, values, governance and rights (figure 2). Standards for STI services began to be defined in the UK by the mid-2000s, first in Scotland in 2008 followed by England in 2010 and have undergone revision in the intervening years.48 Our survey gathered the opinions of country representatives of IUSTI Europe and country leads from the ECEE network1 on standards of STI services for people living with HIV across the European region. Responses were collected via an email link to a survey form. Twenty-two representatives from 21 countries responded (figure 3). Participants were first asked to give a single overall score, between 1 (poor) and 5 (excellent), to represent their opinion of the quality of STI care in their country’s HIV services. The median score was 3 with a range of 1–5, suggesting considerable variation (Box 4). The reported concerns could be grouped into four main areas:
Strong professional demarcations along traditional specialty lines that were not always helpful to patient care. The specific expertise required to treat some STIs was not always accessed, although there were good examples of collaborative working in other areas.
Problems accessing modern testing technology both for symptomatic diagnostics and for asymptomatic screening.
Commissioning of HIV services was often carried out without co-commissioning STI treatment and prevention and reproductive health services, leading to complex referral pathways rather than integration within HIV services. A further reported problem was a separate focus on specific STIs or some blood-borne viruses, which were sometimes described as separately funded through third-sector or non-governmental agencies, leading to pathway fragmentation. Some countries reported comprehensive expert and high-quality STI care within HIV services, indicating this can be achieved.
Ongoing challenges of stigma and broader concerns around values and legal systems in some countries. Some respondents described barriers to the implementation of self-sampling, self-testing, postal submission of tests or sending of medication, preventing remote management. Other countries clearly exploited the capabilities of digital transformation to mitigate the impact of the COVID-19 pandemic.17 The recently published findings of the INTEGRATE work programme in the EU highlighted the legal challenges surrounding partner notification,49 with under 30% of jurisdictions responding having guidelines for partner notifications for a range of STIs including HIV.

Examples of statements about standards for the management of STIs.48

{kind=link}
{kind=link}
{kind=link}
Survey on standards of STI care for people living with HIV. (A) Country representatives that responded to the survey (represented in dark)a; (B) a driver diagram to improve STI care in HIV services developed from the survey. a The designations employed and the presentation of the map do not imply the expression of any opinion whatsoever on the part of the WHO Secretariat concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers and boundaries.
Key points on standards of STI care in people living with HIV
Standard of care for STIs focuses on quality, person-centredness, workforce competence and accessibility.
In a survey of 21 countries across the European region, we identified the following areas for improvement: collaborative working practices across specialties, integration of STI care within HIV services, access to modern diagnostics, antibiotic stewardship, addressing barriers related to stigma, values and legal systems, recognising the needs of vulnerable populations, regulation of commercial providers and planning capabilities.
What does good look like?
The findings from the survey leave us with much to think about. Respondents felt that standards of STI care in HIV clinics in Europe should be developed along clear priorities, indicating two broad aims: recognising the need for an STI service and establishing the provision of the right STI service (figure 3), finding ways to integrate STI care into routine HIV care. Funders in some areas may need convincing that there is a problem requiring public health capacity, and need, at the bare minimum, awareness of the epidemiology and mechanisms to plan and commission services. There are opportunities to harness the impact of the third sector (non-governmental organisations, charities, etc), which has been so influential in campaigns for ART provision and more recently HIV PrEP. There may be significant legal and stigma barriers in some jurisdictions but there is also a good track record in HIV of success in overcoming these barriers. The second main aim is to focus on improving the quality of the services that are on offer. Professionals need to find ways to reduce the demarcation between them. Leadership and cooperation are needed to drive service transformation, embed modern diagnostics, and make sure that guidelines for STI care are adopted and the workforce is appropriately trained. From a patient perspective, a set of rights should apply to anyone living with HIV in Europe, including being able to talk about STI concerns with HIV care providers, getting access to accurate tests for STIs, having free screening for cervical and anal cancer, and having treatment for STIs free of charge with minimal inconvenience.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We are grateful to all the country representatives that responded to the survey: Antonija Verhaz, Antonious Papadopoulos, Arjan Harxhi, Bondarenko Glib, Carmen Lisboa, Cristiana Oprea, David Jilich, Deniz Gökengin, Derek Freedman, Gordana Dragovic Lukic, Henry de Vries, Ivailo Alexiev, Josip Begovac, Justyna Kowalska, Kerstin Aimla, Ľubomír Soják, Marco Cusini, Mariana Mardarescu, Oleg Yurin, Raimonda Matulionyte, Tsyrulnikov Israel, Usha Hartgill.
References
Footnotes
Handling editor Jason J Ong
Twitter @Prof Anna Maria Geretti@GerettiAnna, @teowinterandy
Correction notice This article has been amended since it was first published. Table 1 has been amended to include arrows in row 5, column 5
Contributors AMG drafted the manuscript from the material presented at the workshop. All authors provided critical input to the writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests AMG is Editor-in-Chief of the journal Sexually Transmitted Infections.
Provenance and peer review Not commissioned; externally peer reviewed.