Article Text

Abstract
Objective To understand rates of human papillomavirus (HPV) vaccine acceptability and factors correlated with HPV vaccine acceptability.
Design Meta-analyses of cross-sectional studies.
Data sources We used a comprehensive search strategy across multiple electronic databases with no date or language restrictions to locate studies that examined rates and/or correlates of HPV vaccine acceptability. Search keywords included vaccine, acceptability and all terms for HPV.
Review methods We calculated mean HPV vaccine acceptability across studies. We conducted meta-analysis using a random effects model on studies reporting correlates of HPV vaccine acceptability. All studies were assessed for risk of bias.
Results Of 301 identified studies, 29 were included. Across 22 studies (n=8360), weighted mean HPV vaccine acceptability=50.4 (SD 21.5) (100-point scale). Among 16 studies (n=5048) included in meta-analyses, perceived HPV vaccine benefits, anticipatory regret, partner thinks one should get vaccine and healthcare provider recommendation had medium effect sizes, and the following factors had small effect sizes on HPV vaccine acceptability: perceived HPV vaccine effectiveness, need for multiple shots, fear of needles, fear of side effects, supportive/accepting social environment, perceived risk/susceptibility to HPV, perceived HPV severity, number of lifetime sexual partners, having a current sex partner, non-receipt of hepatitis B vaccine, smoking cigarettes, history of sexually transmitted infection, HPV awareness, HPV knowledge, cost, logistical barriers, being employed and non-white ethnicity.
Conclusions Public health campaigns that promote positive HPV vaccine attitudes and awareness about HPV risk in men, and interventions to promote healthcare provider recommendation of HPV vaccination for boys and mitigate obstacles due to cost and logistical barriers may support HPV vaccine acceptability for men. Future investigations employing rigorous designs, including intervention studies, are needed to support effective HPV vaccine promotion among men.
- Hpv
- Vaccination
- Men
- Meta-Analysis
- Attitudes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Human papillomavirus (HPV) is the most common sexually transmitted infection (STI), causing a substantial burden of disease in men and women.1 ,2 In the USA, half of sexually active men and women contract HPV at some point in their lives.1 The prevalence of anal HPV infection is estimated at around 15% in heterosexual men, 60% in men who have sex with men (MSM) who are HIV negative, and 95% in HIV positive MSM.3–5
Worldwide, the majority of anal and penile cancers among men are associated with HPV infection.6 ,7 The high prevalence of anal HPV among MSM is associated with 44 times higher incidence of anal cancer,7 and among HIV positive MSM approximately 60 times higher incidence of anal cancer than that of the general population.8 Heterosexual men infected with HPV, in addition to increasing their own risks of anal and penile cancers, may contribute to increasing female sexual partners’ risks of developing cervical cancer.9
HPV vaccination for men
The quadrivalent HPV vaccine (HPV4; Gardasil) was licensed in the USA for men in 2009.10 In 2011 the US Advisory Committee on Immunisation Practices approved and recommended routine use of HPV4 for boys aged 11–21 years, with approval for administration up to age 26 years, in order to prevent genital warts and anal cancer.10 HPV4 is recommended for MSM through age 26 years. HPV4 is over 90% effective in preventing a variety of types of HPV infection and genital warts in young men.11 It has also demonstrated efficacy among MSM in preventing anal epithelial neoplasias that are precursors to anal cancer.12
Nevertheless, substantial debate surrounds HPV4 vaccination programmes for men.13 Based on mathematical models suggesting that male HPV4 vaccination programmes exceed cost-effectiveness thresholds,14–16 many European countries do not include men in HPV vaccination programmes, as in the USA, Canada and Australia,10 ,17 ,18 instead focusing on achieving expanded coverage among women to promote herd immunity.19 Support for male HPV4 vaccination programmes is based on evidence of substantial clinical benefits to men,20 cost-effectiveness among MSM,21 largely excluded from mathematical models, increased cost-effectiveness for men with the addition of non-cervical outcomes to mathematical models,15 ,22 ,23 and benefits of a gender-neutral (universal) approach to vaccination.17 ,22 ,24 Furthermore, most mathematical models calling into question the cost-effectiveness of male HPV4 vaccination presume 70% or greater coverage among women,14–16 an estimate that is not supported by data from the USA (three-dose coverage in women ∼32%)10 and many European countries.19
HPV vaccine acceptability
Vaccine acceptability is a crucial factor in uptake.23 The majority of investigations of HPV vaccine acceptability have focused on women.25 A systematic review of six US studies focused on young women identified HPV vaccine acceptability ranging from 55% to 100% although meta-analysis was not conducted and results were not disaggregated by sex.26
A review of 23 quantitative and qualitative studies of HPV vaccine acceptability for men reported a range of acceptability from 33% to 78%.25 The majority of studies indicated parents and healthcare providers (HCP) were more supportive of HPV vaccination for women than men.25 Two review articles,22 ,23 one after US licensure of HPV4 for men,22 describe challenges to achieving broad coverage and the importance of understanding vaccine acceptability for men.
In light of current US recommendations for HPV vaccination of men,10 we conducted quantitative syntheses (meta-analyses, weighted mean acceptability, t tests) to assess: (1) rates of HPV vaccine acceptability and (2) factors correlated with HPV vaccine acceptability among men.
Methods
Eligibility criteria
We followed preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines.27 We included original research studies using quantitative methods that examined rates of HPV vaccine acceptability and/or barriers, facilitators, attitudes, sociodemographic characteristics or other factors associated with acceptability of HPV vaccines. Studies that did not use quantitative methods, report original data, include men or examine HPV vaccine acceptability were not included in this analysis. Types of participants included men reporting on HPV vaccine acceptability. We contacted corresponding authors to provide missing and unreported data or raw data sets when studies did not report sufficient information to be included in meta-analyses.
Outcome measures
The primary outcome was HPV vaccine acceptability rates among men. The secondary outcomes were factors associated with HPV vaccine acceptability: sociodemographic characteristics, HPV vaccine attitudes, HPV vaccine awareness and knowledge, HPV risk perceptions, behavioural risk, HPV vaccine endorsements and structural factors.
Search strategy
We used a comprehensive search strategy to locate articles meeting inclusion criteria across multiple electronic databases: Cochrane Library, Cochrane Central Register of Controlled Trials, AIDSLine, CINAHIL, EMBASE, PsychInfo, Social Science Abstracts, Ovid MEDLINE, Scholars Portal, Social Sciences Citation Index, Dissertation Abstract International, ASSIA: Applied Social Sciences Index and Abstracts database, Cambridge Scientific Abstracts (CSA) Sociological Abstracts, Proquest Research Library, CSA Social Services Abstracts database and AgeLine Database. Databases were searched with no language, geographical or time restrictions; the last search date was 1 March 2013.
Data collection process
All titles and abstracts from the reference lists of articles were screened for inclusion. The full article was obtained when the first reviewer determined the article might meet inclusion criteria based on the study objectives. Two reviewers (CHL and KA or ND) then assessed each article for inclusion based on study type and outcome measures, with a third reviewer (PAN) available to arbitrate in case of disagreement.
Data extraction
We developed a data extraction form using Microsoft Excel. Two reviewers (CHL, KA or ND) extracted the following data: article information (ie, year of publication, author, journal); descriptive data (ie, sample size, country, participant demographics); methods and study design; and outcomes/key findings. Data regarding any variables examined as possible correlates of HPV vaccine acceptability was sought. We developed a list of themes related to HPV vaccine acceptability based on review of the variables explored in the included articles.
Risk of bias
We assessed risk of bias using items from the Effective Public Health Practice Project (EPHPP) ‘Quality Assessment Tool for Quantitative Studies’,28 which we modified for use with cross-sectional studies. We assessed selection bias (representativeness of sample, participation rate), data collection method (validity, reliability) and study design using a rating rubric to determine if each component had low, moderate or high risk of bias.28 Studies with no ‘high risk of bias’ ratings were considered to have an overall low risk of bias, one ‘high risk of bias’ rating moderate risk of bias, and more than one ‘high risk of bias’ rating a high overall risk of bias. No studies were excluded on the basis of risk of bias.
Data analysis
For studies that quantified HPV vaccine acceptability, we linearly transformed acceptability ratings onto a 0–100 scale. We calculated mean HPV vaccine acceptability for each study and weighted mean acceptability overall. Subgroup analyses were prespecified. For studies that reported participant sexual orientation we calculated weighted mean acceptability for gay/bisexual/MSM and heterosexual men, and used unpaired t tests to compare HPV vaccine acceptability by sexual orientation.
Meta-analysis was conducted on studies that examined similar correlates or predictors of HPV vaccine acceptability. We used V.2 of Comprehensive Meta-Analysis Software to calculate effect sizes for each variable, with a random effects model to compensate for clinical and methodological diversity between studies. We combined coefficients across studies for each variable that was examined in order to derive a global estimate of its correlation with HPV vaccine acceptability. We calculated the Q statistic to assess homogeneity of correlations across studies (within-study variability) and the I2 index to assess the degree of heterogeneity (between-study variability).
We included all studies examining correlates of HPV vaccine acceptability that provided sufficient data (eg, correlations, ORs, χ2 statistics or t values) in the meta-analysis. As the majority of studies did not evaluate interventions, we did not conduct meta-analysis on dichotomous (intervention vs control group) data.
Results
Study selection
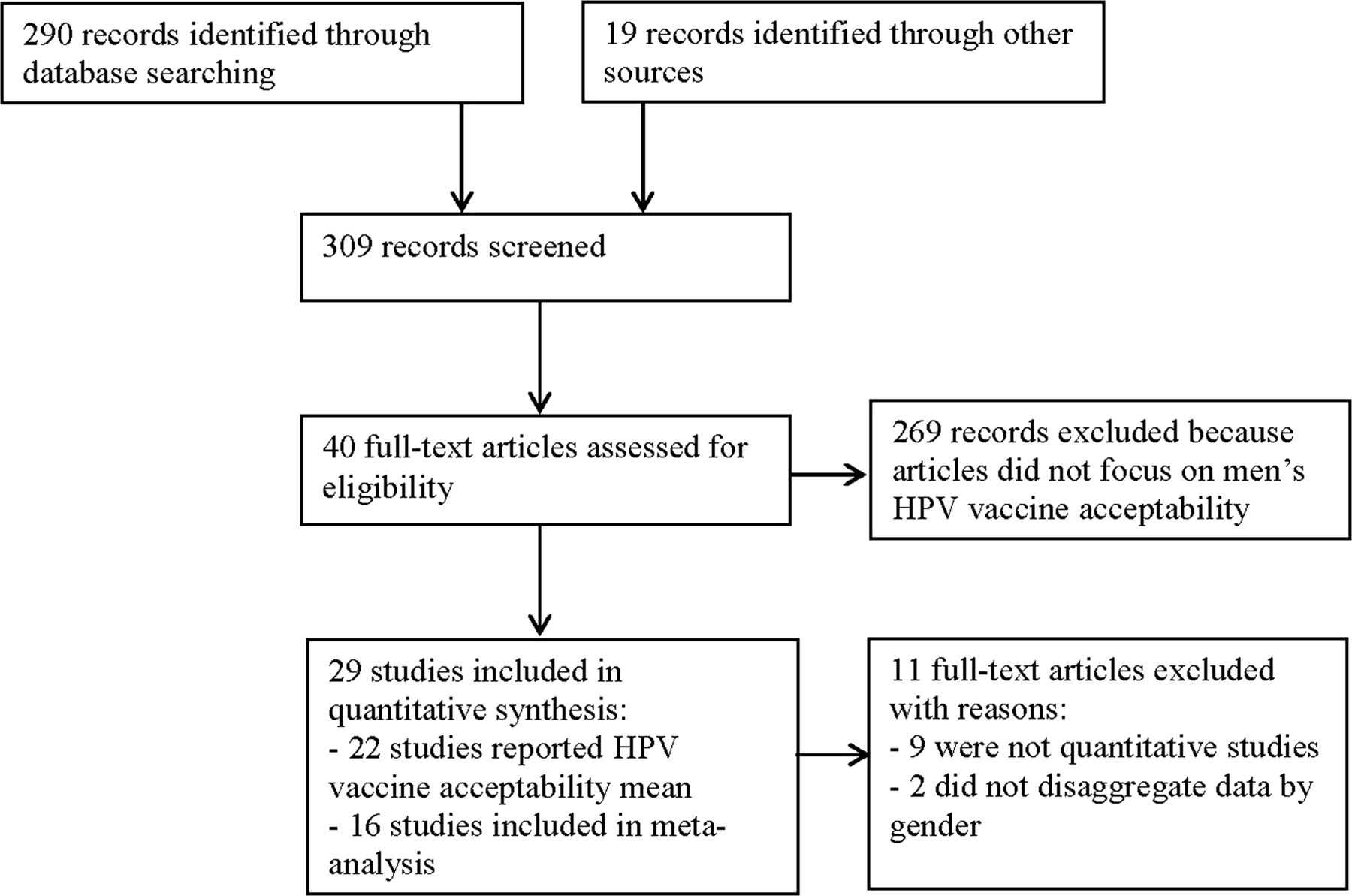
The literature search yielded 309 studies (see figure 1), with 100% agreement between reviewers (CHL, KA or ND) in selecting relevant articles. Of the 40 relevant studies, we excluded 9 because they were not quantitative and 2 because data were not disaggregated by gender. Twenty-nine remaining studies were included in this analysis.
{kind=link}
Flow diagram of articles selection progress for human papillomavirus vaccine acceptability among men review.
Study characteristics
Two reviewers (CHL, KA or ND) determined whether the same sample and study were used more than once. The 29 articles9 ,24 ,29–55 reflect 24 original studies,9 ,29 ,30 ,34–47 49–55 all published in English. Half (n=12) of the studies were conducted in the USA, three in Australia, two in Sweden (n=2), and one each in Canada, Germany, the Netherlands, New Zealand, Philippines, Singapore and South Korea. Ninety-one per cent (n=21) of the study samples were adult men; two studies were conducted among adolescent boys aged 14–19 years.29 ,43 Study characteristics and mean HPV vaccine acceptability are outlined in table 1.
Studies addressing human papillomavirus (HPV) vaccine acceptability, study characteristics and risk of bias, ordered by mean vaccine acceptability (n=29)*
The majority of studies (n=20; 83%) had high risk of bias,29 ,34–41 43–47 ,49 ,50 ,52–55 three (13%) moderate risk of bias9 ,30 ,51 and one (2%) low risk of bias.42 All studies were cross-sectional in design except for two cohort studies.42 ,44 Eight studies (33%) used random sampling9 ,30 ,37 ,47 ,49–52 ,54; 16 studies used non-random sampling techniques.
Twenty-nine studies quantified HPV vaccine acceptability among men (see table 1). We included 22 studies (n=8360)9 ,24 ,29 ,30 ,34–47 ,49 ,51 ,53–55 in the calculation of mean HPV vaccine acceptability because in several cases9 ,24 ,30–33 ,41 ,48 ,51 different studies were based on the same sample. In one study we treated two samples separately as the authors reported separate means and correlates for men enrolled in a clinical study and college students.30 ,31 Among these 22 investigations, mean HPV vaccine acceptability ranged from 8.2 to 94.0 with overall mean acceptability of 56.6 (SD 21.3) (weighted mean=50.4, SD 21.5).
In the nine studies that reported HPV vaccine acceptability and sexual orientation, weighted mean acceptability was 58.44 (SD 16.76) among gay/bisexual/MSM (n=986) and 50.98 (SD 19.67) among heterosexuals (n=1713),9 ,35 ,41 ,42 ,44 ,51 ,53–55 although not statistically significant (t (2699)=0.24, p=0.81).
Meta-analytic results: correlates of HPV vaccine acceptability among men
Sufficient data were provided to examine the association between HPV vaccine acceptability and factors in seven categories: sociodemographics, HPV knowledge, HPV risk perceptions, HPV vaccine attitudes, endorsement from others, behavioural risk indicators and structural barriers. Table 2 reports weighted mean correlational effect sizes measuring the association of each factor with HPV vaccine acceptability and 95% CIs, as well as the Q test of homogeneity and I2 index of between-study variability. I2 values of 25% represent low, 50% medium and 75% high heterogeneity.56 Sixteen studies (n=5048) were included in the meta-analysis.9 ,24 ,30 ,34–37 ,40 ,42 ,44–56
We used a random effects model in the meta-analysis to account for between-study variability. As the small number of studies examining many factors precluded subanalyses of moderator variables or meta-regression, we examined individual results to identify potential reasons for between-study variability. Substantive (ie, participant characteristics) and methodological (ie, sample size) differences may have impacted between-study variability.
We identified factors associated with HPV vaccine acceptability across seven domains.
HPV vaccine attitudes: acceptability was positively correlated with perceived HPV vaccine benefits (r=0.51, p<0.001), anticipatory regret (r=0.27, p<0.001), perceived HPV vaccine effectiveness (r=0.19, p<0.001); and negatively correlated with fear of needles (r=−0.11, p<0.05) and fear of side effects (r=−0.09, p<0.01).
HPV vaccine endorsement: acceptability was positively correlated with HCP recommendation (r=0.42, p<0.01), supportive/accepting social environment for HPV vaccines (r=0.18, p<0.001) and negatively correlated with partner thinks one should get the vaccine (r=−0.41, p<0.001).
HPV risk perceptions: perceived risk or perceived susceptibility to HPV infection (r=0.25, p<0.001) and perceived HPV severity (r=0.09, p<0.001) were positively associated with acceptability.
Behavioural risk indicators: number of lifetime sexual partners (r=0.18, p<0.01), having a current sex partner (r=0.17, p<0.05), smoking cigarettes (r=0.12, p<0.05) and history of STI (r=0.10, p<0.05) were positively correlated with HPV vaccine acceptability. Non-receipt of hepatitis B vaccine was negatively correlated with acceptability (r=−0.16, p<0.001).
HPV awareness (ie, having heard about HPV) (r=0.17, p<0.01) and HPV knowledge (ie, correctly answering questions about HPV) (r=0.09, p<0.05) were positively associated with acceptability.
Structural barriers: vaccine cost (r=−0.17, p<0.001), logistical barriers (eg, hassle, time, transportation) (r=−0.16, p<0.05) and need for multiple shots/doses (r=−16, p<0.01) were negatively correlated with HPV vaccine acceptability.
Sociodemographic characteristics: being employed (r=0.13, p<0.05) and non-white (vs white) ethnicity (r=0.09, p<0.05) were positively associated with HPV vaccine acceptability. Educational level, included in the majority of studies examined, approached significance (r=0.08, p=0.05).
Perceived HPV vaccine benefits, anticipatory regret, HCP recommendation and partner thinks one should get vaccine had medium effect sizes on HPV vaccine acceptability (see table 2), based on Cohen's classification.57 The remaining correlates had low effect sizes.
Discussion
This meta-analysis reveals a moderate level of HPV vaccine acceptability among men (50.4 on a 100-point scale) across 22 studies totalling 8360 participants, with a wide range of acceptability (8.2–94.0) across studies. In contrast, acceptability was considerably higher (55.0–100.0) in a review of US studies focused on young women,26 although mean acceptability was not reported.
Meta-analysis results across 16 studies (n=5048) indicate the influence of positive HPV vaccine attitudes, HCP recommendation, perceived HPV risk and HPV awareness and knowledge on HPV vaccine acceptability for men. Health promotion messaging that fosters positive attitudes about HPV vaccination benefits for men, accurate HPV risk perceptions, and that enhances awareness and knowledge regarding HPV may increase the acceptability of HPV vaccination for men.
We found no significant difference in HPV vaccine acceptability between gay, bisexual and other MSM, who would benefit most from HPV4 vaccination,7 ,8 and heterosexual men. Results from the meta-analysis suggest that in addition to promoting HPV4 vaccination for all boys and young men,23 ,25 ,48 ,51 targeted messaging for young MSM to support perceived HPV vaccine benefits and effectiveness, and accurate perceptions of HPV risk may increase acceptability.
HCP recommendation, the correlate with the second highest impact on HPV vaccine acceptability after perceived HPV vaccine benefits, has been identified as an important factor in HPV vaccine acceptability for girls,26 and patient acceptance of hepatitis B vaccines.58 HCP-identified barriers to hepatitis B vaccination—lack of government reimbursement, patient non-disclosure of risk and inadequate time to assess risk59—suggest that in addition to promoting HCP recommendation of HPV4 vaccination for boys, it is important to assess systemic and structural barriers that may impede HCP recommendation.
The impact of HPV risk perceptions, awareness and knowledge on HPV vaccine acceptability is notable given evidence of low levels of HPV knowledge and awareness among men.32 ,50 ,60 Mechanisms to foster accurate HPV risk perceptions and awareness might involve addressing the prevalence of HPV infection and its association with cancers among men, highlighting cancer prevention as a benefit of HPV vaccination for boys48 and challenging false beliefs that HPV vaccines are not relevant for men.25
Notably, out-of-pocket cost, as reported in earlier reviews,22 ,23 ,25 logistical barriers and the need for a series of injections were negatively associated with acceptability. In meta-analysis these structural barriers had a greater impact than HPV vaccine knowledge (the most often studied correlate) and effect sizes equal to behavioural risk factors. In addition to tailored educational interventions government financing of HPV4 vaccination, and interventions to reduce barriers in access to vaccination may significantly increase HPV4 vaccine acceptance among men.
Finally, further research is needed to explore the negative association between partner thinks one should get the HPV vaccine and HPV vaccine acceptability, based on only two studies.24 ,44 Partner endorsement might implicate stigma and the association of HPV as a women's disease.25
Limitations to this meta-analysis include the absence of intervention studies, the relatively small number of studies and exclusion of unpublished studies, with few studies from each of several countries outside the USA. The lack of intervention studies precludes using RevMan 5 for meta-analyses; and some correlates of HPV vaccine acceptability are based on few studies. The limited number of studies in each setting precludes subanalysis by country. Additional studies overall and within each setting will help to identify possible differences in acceptability, including by healthcare systems and culture. Two studies of parental acceptance of HPV vaccines for male adolescents were included in the calculation of mean acceptability though not included in meta-analysis; given different challenges to uptake for adolescents and adults, meta-analysis of parental acceptance of HPV vaccination for boys is indicated.
Another limitation is due to the high risk of bias among the majority of studies included in the meta-analysis; this is indicative of weak study designs (ie, cross-sectional, non-random sampling) and suggests caution in generalising the results. However we used a random effects model that takes into account between-study and within-study variability, which suggests that the effect sizes approximate an appropriate mean of a distribution of effects. This meta-analysis provides a quantitative synthesis of the literature, indicating correlates of HPV vaccine acceptability and the magnitude and direction of these associations among a large sample of men across different studies.
Finally, as most of the studies reviewed were conducted before the US Advisory Committee on Immunisation Practices recommended routine HPV4 vaccination of men, levels and correlates of HPV vaccine acceptability may shift with additional post-2011 studies. However, low HPV vaccine coverage among young women in the USA and Europe since licensure in 200610 ,18 suggests the importance of synthesising available evidence on acceptability to guide evolving policy recommendations.
This meta-analysis suggests the importance of future investigations using more rigorous designs, including intervention research, to address factors that promote HPV vaccine acceptability among men. Generally lower levels of support for HPV vaccination among HCP and parents for young boys versus young girls11 ,25 and the particular need for HPV4 vaccination in gay/bisexual/MSM, indicate the importance of routinely disaggregating data by sex and sexual orientation in future investigations of HPV vaccine acceptability.
Overall, the moderate level of vaccine acceptability among men in the case of HPV, the most common STI, supports the need for evidence-informed interventions to address widespread gaps between HPV vaccine recommendations and actual use.
Key messages
-
A moderate level of human papillomavirus (HPV) vaccine acceptability (50.4 on a 100-point scale) was reported among 8360 men across 22 studies.
-
Perceived HPV vaccine benefits and healthcare provider recommendation were the two most influential correlates of HPV vaccine acceptability among men.
-
HPV vaccine cost and logistical barriers may pose significant obstacles to uptake.
-
HPV vaccination campaigns targeting men should promote awareness of HPV, HPV-associated cancer risks and HPV vaccine efficacy, and healthcare providers’ recommendation of HPV vaccination for boys.
Acknowledgments
The authors thank two anonymous reviewers for their helpful comments.
References
Footnotes
-
Handling editor Jackie A Cassell.
-
Contributors PAN conceptualised the study, contributed to data analysis and led writing of the manuscript. CHL, KA and ND reviewed titles and abstracts for inclusion in the review, read the articles and reviewed the manuscript. CHL conducted meta-analysis and drafted the methods and results.
-
Funding This research was funded in part by grants from the Canadian Institutes of Health Research (funding reference number THA-118570) through the Canadian HIV Vaccine Initiative, and the Canada Research Chairs program (950-204522).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.