Article Text

Abstract
Objectives Infections due to Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) are among the most common bacterial sexually transmitted infections worldwide, most of which are asymptomatic. Detection of infection using a variety of specimen types in symptomatic and asymptomatic subjects is important to effectively combat CT/NG infections. The performance of the cobas CT/NG v2.0 test was assessed for urogenital swabs, urine and cervical cytology samples collected in PreservCyt Solution from 5266 symptomatic and asymptomatic women (including 202 who were pregnant), and urine from 738 men.
Methods Sensitivity and specificity were estimated compared with a patient infected status determined using two US Food and Drug Administration–cleared nucleic acid amplification tests.
Results Among 6004 participants, 487 CT (8.1%) and 159 NG (2.6%) infections were identified. Sensitivity estimates for CT for women ranged from 91.2% to 97.6% depending on specimen type, and the estimate for male urine specimens was 98.4%. Specificity for CT ranged from 99.2% to 99.7%. Sensitivity estimates for NG ranged from 95.6% to 100.0% for women, and the estimate for men was 100.0%. Specificity for NG ranged from 99.3% to 100.0%.
Conclusions The cobas CT/NG v2.0 test performs well using urogenital swabs, urine and cervical samples collected in PreservCyt solution.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) infections are the most common bacterial STIs worldwide.1 Over 80% of chlamydia infections and 55% of gonorrhoea infections are asymptomatic and could go undetected in the absence of screening.2 3 Untreated chlamydia and gonorrhoea can lead to serious complications, including pelvic inflammatory disease and subsequent infertility, chronic pelvic pain and tubal pregnancy.4 Infants born to infected mothers can develop conjunctivitis and pneumonia.5 Screening recommendations for chlamydia and gonorrhoea are based on age or risk factors.6–10Effective screening strategies have been shown to reduce maternal complications, adverse events during pregnancy, newborn morbidity and transmission of infection.11
Nucleic acid amplification tests (NAATs) are highly sensitive and the preferred tests for CT and NG screening and diagnosis.6–10 For the detection of NG infections, a broad range of specimen types are acceptable;6 8 10 however, for CT detection, the preferred specimen types for NAATs are vaginal swabs for women and first catch urine from men.6 7 9 In addition to these specimen types, the Centers for Disease Control and Prevention (CDC) guidelines also recognise the use of endocervical samples.6 Accepting a range of specimen types maximises clinician and client convenience, a key strategy to increase screening coverage, and also allows detection of infection in both symptomatic and asymptomatic patients, including pregnant and non-pregnant women, an important attribute for an effective CT/NG screening test. The cobas CT/NG v2.0 test (cobas) (Roche Molecular Systems) is a partially automated CT/NG assay designed for use in clinical laboratories.12–15 The VENUS II study (vaginal, e ndocervical and urine clinical trial for CT/NG) described in this manuscript evaluated the performance (sensitivity, specificity and predictive value) of the cobas test for detection of CT and NG using female vaginal swabs, urine and cervical samples and from urine samples from men compared with other commercially available assays.
Materials and methods
Study design
The VENUS II study was a multicentre evaluation performed with the cobas specimen collection kit and the cobas CT/NG v2.0 test on the cobas 4800 system (Roche Molecular Systems, Pleasanton, California). The results were compared with the Gen-Probe Aptima Combo2 Assay (AC2) (Hologic, San Diego, California, USA) and the BD ProbeTec CT Qx and GC Qx Amplified DNA (CTQ/GCQ) assays (BD Diagnostics, Sparks, Maryland, USA). All assays were performed in accordance with the relevant package insert information at the time. The AC2 and CTQ/GCQ assays were used as reference tests to determine the patient infection status (PIS). PIS was defined as positive for each participant when both confirmatory NAATs (with different target regions for CT and NG) were positive in the endocervical and/or urine specimens. Participants were classified as uninfected when both results from the confirmatory devices were negative, or when only one assay generated positive results. Additionally, women were categorised as uninfected at the endocervix if the result was positive for both reference urine specimens only, but negative by the two reference endocervical swabs from both confirmatory devices and the AC2 liquid-based cytology (LBC). If the PIS was indeterminate due to missing or invalid results from the confirmatory devices, participants were considered non-evaluable and were excluded from analyses. The cobas 4800 system was used to perform testing at seven geographically and clinically diverse specimen collection sites, including obstetrics/gynaecology (OB/GYN) practices, family planning clinics and STI clinics.
Patient populations
The study design for VENUS II included evaluation of archived clinical specimens collected during the initial VENUS study.12 14 16 Specimens from the initial VENUS study included samples from symptomatic women and symptomatic and asymptomatic men, for which residual volume was sufficient. The testing personnel were blinded to the results obtained during the original trial. Patients provided signed informed consent for their samples to be included in the study.
Additionally, VENUS II prospective enrolment focused specifically on asymptomatic women, evaluating endocervical swabs, urine specimens, vaginal swabs and cervical specimens collected in PreservCyt Solution (Hologic) tested prior to and following Pap slide preparation. Inclusion criteria for prospective enrolment required asymptomatic women to be at least 14 years of age and eligible for routine CT/NG evaluation. Exclusion criteria were (1) previous study enrolment, (2) use of antimicrobial agents active against CT or NG during the preceding 21 days, (3) use of Replens (Lil’Drug Store Products, Cedar Rapids, Iowa, USA) within the preceding 3 days, (4) history of hysterectomy or (5) contraindication to Pap test/cervical sampling. Participants reporting dysuria/pain during urination, coital pain/difficulty/bleeding, abnormal vaginal discharge or pelvic/uterine/ovarian pain were considered symptomatic and excluded from prospective enrolment. All seven study sites aimed to enrol similar numbers of participants, with a target of 75 PIS-positive patients in total.
Specimen collection
For each of the 1008 prospectively enrolled female subjects, the following were obtained in this order: a first-catch urine sample, a single clinician-collected vaginal swab, three clinician-collected endocervical swabs using each manufacturer’s sample collection device (in a randomised order) and a cervical sample suitable for LBC placed into PreservCyt Solution (Hologic Corporation, Bedford, Massachusetts) obtained with a spatula/cytobrush or broom. Urine specimens were divided into three aliquots; one aliquot was placed into each assay’s transport tube. LBC samples were aliquoted into cobas sample tubes and AC2 transport tubes prior to processing for Pap testing (prequot LBC). Following Pap processing, residual specimens were aliquoted into cobas sample tubes (postquot LBC). Specimens were collected and either tested locally or shipped to one of seven sites and tested in accordance with each manufacturer’s package insert instructions. Prospectively collected specimens were tested by all three methods, and the remnant specimens previously collected and analysed in the original VENUS study were re-analysed using only the cobas CT/NG v2.0 test.
Cobas CT/NG v2.0 test
The cobas CT/NG test uses real-time PCR technology and has previously been described in detail.15 Samples are extracted on the cobas x480 instrument; PCR amplification and detection is fully automated on the cobas z480 analyser. The cobasCT/NG v2.0 test has the same chemistry as the cobas CT/NG test, with improvements in sample processing and performance.
Statistical analysis
The US Food and Drug AdministrationDA guidance and the Clinical and Laboratory Standards Institute guidelines were used to determine statistical analyses used for the study.16 17 Demographics and baseline characteristics were summarised for evaluable participants overall. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the cobas test were calculated separately for detection of CT and NG using the PIS. The corresponding two-sided 95% score (Wilson) CIs were also reported.18 Per cent positivity was calculated as the proportion of infected participants overall.
Results
Participants
Of the 6045 participants enrolled, only 10 were excluded from the analyses because they did not meet study entry criteria or because they withdrew consent. Additionally, 31 were considered non-evaluable and were excluded from analyses because of errors in specimen handling, unknown PIS for both CT and NG, repeatedly inhibitory (IC failure) or invalid cobas results after initial testing and/or retesting. Therefore, 6004/6035 (99.5%) participants were evaluable for CT and/or NG primary analyses (5266 women and 738 men), and their complete baseline characteristics are presented in online supplementary table 1. The number of patients with each given sample type is detailed in online supplementary figure 1. A total of 2255 (37.6%) symptomatic and 3749 (62.4%) asymptomatic participants with a mean age of approximately 28 years were included in the study. Most women (94.4%) were not pregnant and (n=3683, 61.3%) were enrolled at OB/GYN and family planning rather than STI clinics.
Supplemental material
Supplemental material
Clinical performance of the cobas CT/NG v2.0 test for CT detection
Of 487 CT-infected participants, 365 (75%) were women. Symptoms were reported by 44.4% of infected and 37.0% of uninfected women. Most (70.4%) infected women had positive results from all three tests across all sample types. Only 19 (5% of infected) women tested positive by both NAATs at one anatomic site (10 urine only; 9 endocervical only).
Sensitivity, specificity and predictive values of the cobas test for CT was defined by PIS for gender, sample type and symptom status. For women, overall sensitivity was highest for self-collected and clinician-collected vaginal swabs (97.6% and 97.3%, respectively). Sensitivity estimates were 93.8%, 93.6%, 92.5% and 91.8% for endocervical swabs, urine specimens and LBC prequot and postquot, respectively (table 1). For men, sensitivity was 98.4% (95% CI 98.1% to 99.7%), all but two of the 122 CT-infected men, urine specimens tested positive with the cobas test (online supplementary table 12b). Specificity for CT ranged from 98.8% to 99.8% in both female and male specimens. Similar calculations were performed to estimate the performance of the two comparator assays and the data are shown in online supplementary tables s2a and b. Calculated hypothetical PPVs calculated from performance in the current study indicate CT PPV of 69% at 1% prevalence of CT disease up to a PPV of 98.2% in a population with 20% prevalence (figure 1A).

Hypothetical PPV based on varying population prevalence for (A) cobas Chlamydia trachomatis results and (B) cobas Neisseria gonorrhoeae results. CT, C. trachomatis; NG, N. gonorrhoeae; PPV, positive predictive value.
Clinical performance for Chlamydia trachomatis detection by sample type and symptom status compared with patient infection status
Clinical performance for Neisseria gonorrhoeae detection by sample type and symptom status compared with patient infection status
Clinical performance of the cobas CT/NG v2.0 test for NG detection
Of 159 NG-infected participants, 92 (58%) were women (table 2). Symptoms were reported in 46.7% of infected and 37.4% of uninfected women. Most (71.7%) infected women had positive results from all three tests across different sample types. Four female participants with matched urine and swab specimens tested positive by both NAATs only at the endocervical site, but results were negative for urine. For all 67 NG-infected men, urine specimens tested positive with cobas. Of the 738 men, 37.7% were symptomatic and 62.3% were asymptomatic. According to the PIS algorithm, the NG positivity rate was 1.7%, 9.1% and 2.6% in women, men and the entire study population, respectively.
Sensitivity, specificity and predictive values of cobas for NG was defined by PIS for gender, sample type and symptom status. For women, sensitivity was 100.0% for clinician-collected vaginal swabs and 96.7%, 96.6%, 95.6%, 96.7% and 95.6% for self-collected vaginal swabs, endocervical swabs, urine specimens and LBC pre-quot and post-quot specimens, respectively. Sensitivity was 100.0% for male urine specimens. As with CT, sensitivity did not differ by symptom status and specificity for NG ranged from 99.1% to 100.0% in both women and men. NG results from the cobas assay in symptomatic and asymptomatic participants and the two comparator assays are presented in more detail in online supplementary table 3a and b.
Head-to-head comparison
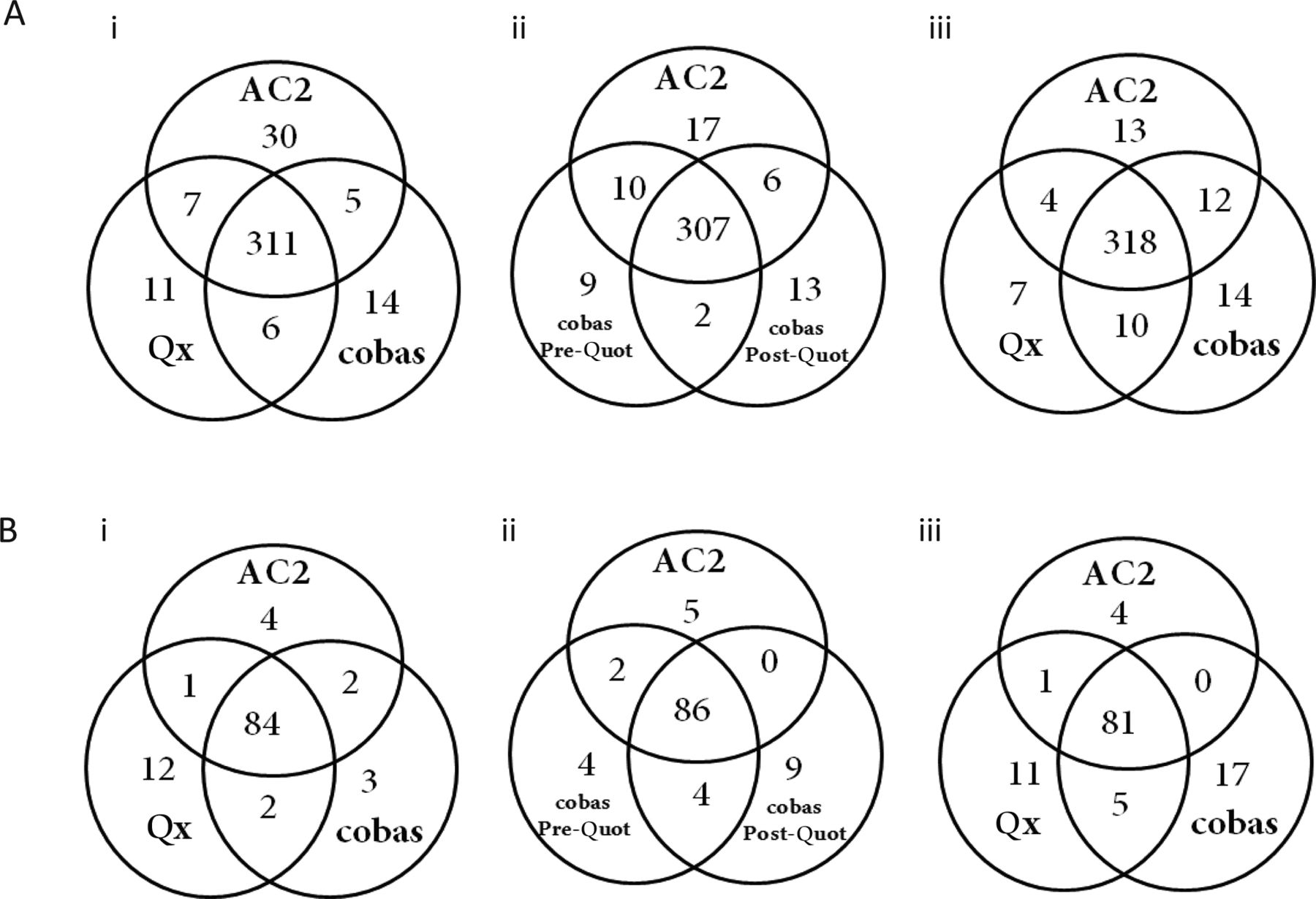
To remove the variation in positives created by potentially site-specific infections, additional analyses were performed to compare the head-to-head performance of (1) ccobasobas with the AC2 and CTQ/GCQ assays in endocervical swab and urine specimens and (2) cobas LBC pre-quot and post-quot result with AC2 results. Venn diagrams comparing all positive results, regardless of the final definition of infection status, for CT are shown in figure 2A. Using endocervical swabs for CT, 85.7% (329/384) were positive by two or more assays while single assay positives were identified by 3.6% (14/384), 2.9% (11/384) and 7.8% (30/384) by cobas, CTQ and AC2 assays, respectively. Endocervical swab sample results for CT were not significantly different when comparing cobas to Qx samples (kappa=0.9410), cobas to AC2 samples (kappa=0.9113) and Qx to AC2 samples (kappa=0.9189) (figure 2Ai). Using female urine specimens, the CT results were positive by two or more assays in 91.0% of samples with any positive result and single positives were obtained by the cobas, CTQ and AC2 assays for 3.7, 1.9 and 3.4% of samples, respectively. Urine sample results for CT were not significantly different when comparing cobas to Qx samples (kappa=0.9427), cobas to AC2 samples (kappa=0.9372) and Qx to AC2 samples (kappa=0.9344) (figure 2Aiii). LBC sample results for CT were not significantly different when comparing cobas pre-quot to cobas post-quot samples (kappa=0.9738), cobas pre-quot to AC2 pre-quot samples (kappa=0.9453) and cobas post-quot to AC2 pre-quot samples (kappa=0.9325) (figure 2Aii).

{kind=link}
{kind=link}
(A) Venn diagrams comparing Chlamydia trachomatis Chlamydia trachomatis (CT) and (B) Neisseria Neisseria gonorrhoeae (NG) percent positive results across three assays in (i) endocervical swabs, two assays in (ii) liquid-based cytology specimens and three assays in (iii) urine specimens obtained from female participants. For CT, a total of 5092 (endocervical swabs), 4824 (liquid-based cytology) and 5100 (urines) participants had all three valid results from cobas CT/NG v2.0 test, AC2 and Qx assays. For NG, a total of 4824 (endocervical swabs), 4819 (liquid-based cytology) and 5102 (urines) participants had all three valid results from cobas CT/NG v2.0 test, AC2 and Qx assays.
Comparison of all positive results for NG, regardless of the final definition of infection status, is depicted in figure 2B. Using endocervical swabs for NG, 82.4% (89/108) were positive by two or more assays while single assay positives were identified by 2.7% (3/108), 11.1% (12/108) and 3.7% (4/108) by cobas, GCQ and AC2 assays, respectively. Endocervical swab sample results for NG were not significantly different when comparing cobas with Qx samples (kappa=0.9035), cobas to AC2 samples (kappa=0.9441) and Qx to AC2 samples (kappa=0.8927) (figure 2Bi). From female urine specimens, NG-positive results were obtained from two or more assays in 73.0% (87/119). Single positives were obtained by cobas, GCQ and AC2 assays for 14.3% (17/119), 9.2% (11/119) and 3.4% (4/119) of samples, respectively. Urine sample results for NG were not significantly different when comparing cobas with Qx samples (kappa=0.8528), cobas to AC2 samples (kappa=0.8545) and Qx to AC2 samples (kappa=0.8893) (figure 2Biii). LBC sample results for NG were not significantly different when comparing cobas pre-quot with post-quot samples (kappa=0.9215), cobas pre-quot with AC2 pre-quot samples (kappa=0.9298) and cobas post-quot with AC2 pre-quot samples (kappa=0.8937) (figure 2Bii).
CT and NG prevalence
Overall, the CT prevalence (by PIS) was 6.9% (365/5265) in women, 16.5% (122/738) in men and 8.1% (487/6004) in the entire study population. Hypothetical PPVs calculated with performance from the current study indicate NG PPVs range from 82% to 99.1% in a population with disease prevalence from 1% to 20% (figure 1B).
CT and NG prevalence in pregnant women
The frequency of CT and NG infection in pregnant women enrolled in this large study population was 8.4% (17/202) and 1.5% (3/202) for CT and NG, respectively. Sensitivity of ccobasobas for CT in this subpopulation was 87.5% (14/16, 95% CI 64.0% to 96.5%) for endocervical swabs, 94.1% (16/17, 95% CI 73.0% to 99.0%) for urine specimens, 87.5% (7/8, 95% CI 52.9% to 97.8%) for both self-collected and clinician-collected vaginal swabs, 81.3% (13/16, 95% CI 57.0% to 93.4%) and 88.2% (15/17, 95% CI 64.0% to 96.5%) for pre-ThinPrep and post-ThinPrep processing PreservCyt specimens, respectively. The sample size is small and no differences in sample type performance effects were observed (all p values from Fisher exact tests >0.10). Specificity was consistently ≥97.6% across all sample types (lowest 95% CI 91.5% to 99.3%). Sensitivity of cobas for detection of NG in pregnant women was 100.0% for all sample types (n=1, 2 or 3 NG-positives/sample type). Specificity was 100.0% across all sample types for pregnant women, except for PreservCyt specimens (post-ThinPrep processing), which was 99.5% (185/186, 95% CI 97.0% to 99.9%).
Discussion
According to CDC 2014 recommendations, optimal specimen types for detecting genital CT and NG infections are vaginal swabs in women and first-catch urine in men6; recent studies support these conclusions.12 14 In the present study, sensitivity, specificity, PPV and NPV of cobas in all sample types were high (>90%). Importantly, we did not observe statistical differences in performance of this assay among participants with and without symptoms. These data demonstrate that the cobas CT/NG v2.0 test can be used reliably in asymptomatic populations and in diagnostic testing of symptomatic patients; a test with such dual purposes is recommended.6–10 There is no rationale against using vaginal swab samples in women, even in the presence of symptoms, since they perform as well as endocervical swabs and are easier to obtain. Self-obtained vaginal swabs could allow sample collection before visiting a clinician, enabling clinicians to evaluate patients independently of sample collection. This process change may improve adherence to screening recommendations by speeding up the clinical process and creating a normative environment for sample collection.
The cobas test also allows for testing of cervical samples using swabs or samples collected in PreservCyt solution commonly performed for cervical cancer screening via molecular tests or Pap smears.14 Interestingly, both pre-quot and post-quot samples provided high sensitivity and specificity, suggesting no contamination in the Pap processing (Lewinski et al, manuscript in preparation). The addition of pre-quot and post-quot sample suitability as shown in the present study adds to the flexibility in choosing from a large variety of sample types for testing, potentially further increasing the success of screening programmes.
Testing of pregnant women for CT and NG is recommended in the first trimester,5 and in this study, the rates of infection for CT and NG were comparable between pregnant and non-pregnant women. Rates of infection in pregnant women (8.4% for CT and 1.4% for NG) observed in this study clearly support the CDC recommendations for prenatal screening.6 In pregnant women with CT infections, cobas sensitivity estimates were not as high as percentages in women overall, but the number of these participants (n=17) was small. Specificity in CT infections and sensitivity and specificity percentages in NG infections across sample types were comparable with those in women overall.
In light of the small changes to sample processing between the cobas CT/NG v2.0 test and the previous version test, the re-analysis of specimens from VENUS showed that the cobas CT/NG v2.0 test performs as well as the previous version test across the sample types in this study.12 14
Availability of new assays such as the cobas CT/NG v2.0 test provides laboratories with a comprehensive approach to genital tract CT and NG infection testing. The cobas assay exhibited high sensitivity, specificity, PPV and NPV for the detection of CT and NG in endocervical swabs, urine specimens, vaginal swabs and cervical specimens collected in PreservCyt Solution from asymptomatic and symptomatic women and in urine specimens in men.
Key messages
The cobas CT/NG v2.0 test was sensitive and specific for the detection of Neisseria gonorrhoeae and Chlamydia trachomatis infection.
The cobas CT/NG v2.0 test performed well across the following sample types: urogenital swabs, urine and cervical cytology samples.
In this study, vaginal swabs, which can be self-obtained, performed as well as endocervical swabs, enabling testing to occur independently of clinician sample collection.
Acknowledgments
We are grateful to John Duncan and Dr Shaowu Tang for expert statistical support.
References
Footnotes
Handling editor Catherine A Ison
Contributors All authors collaborated in the writing of the manuscript. ML and OL were also involved in the design and management of the study. The study was performed by MBN, SY, SNT, RAL, BAB, CE, EWH III and BVDP. Statistical analyses were performed by John Duncan and Shaowu Tang. All authors contributed to the analysis and interpretation of results.
Funding This study was funded by Roche Molecular Systems, Pleasanton, CA.
Competing interests BVDP discloses consulting honoraria or research funding received from Atlas Genetics, BD Diagnostics, Beckman Coulter, Cepheid, Rheonix and Roche Molecular Systems. EWH III has received research support from Roche Molecular Systems, BD Diagnostics, Hologic Gen-Probe Inc., Siemens and Cepheid. SNT discloses research support from Roche Molecular Systems, BD Diagnostics, Hologic Gen-Probe Inc. and Cepheid. BAB discloses being former employee and officer of Laboratory Corporation, Holdings (LabCorp) and advisory board service and contracts for laboratory work for Roche Diagnostics for which LabCorp was compensated and advisory board service for Roche Molecular Systems for which LabCorp was compensated. She has current consulting contracts with LabCorp, Qiagen, Inc. and Meridian Biosciences, Inc. JO, ML and OL are employees of Roche Molecular Diagnostics. No other authors disclose conflicts of interest.
Patient consent Obtained
Ethics approval All procedures in the VENUS II study, including use of the cobas v2.0 assay, were approved by different Institutional Review Boards (IRBs) depending on the testing or collection site: CGIRB (IRB00001313), Indiana University—Office of Research Administration (IRB00004961, IRB00000222), Independent IRB (IRB00003563), LSU Health Sciences Center—New Orleans IRB (IRB00000177, IRB00000179), University of New Mexico Health Sciences Center, Human Research Review Committee (Committee 1 IRB00000591, Committee 2 IRB00000592, Committee 3 IRB00001775, Committee 4 IRB00001776), Western IRB (IRB00000533), Copernicus Group IRB (IRB00001313), New England IRB (IRB00000755), Los Angeles County Public Health IRB (IRB00000864), Johns Hopkins Medicine IRB (IRB000735558), Maryland Department of Health IRB (IRB00000785) and Office of Human Research Ethics IRB University of North Carolina (Committee 1 IRB00000538, Committee 2 IRB00000539, Committee 3 IRB00001648, Committee 4 IRB00001649).
Provenance and peer review Not commissioned; externally peer reviewed.