Article Text

Abstract
Objectives Individuals with genital warts may be particularly susceptible to human papillomavirus since they have failed to clear the virus. Consequently, women with genital warts could be at increased risk of cervical dysplasia. In this cohort study we aimed to compare the incidence of cervical intraepithelial neoplasia grade 2 or worse (CIN2+) in women with a diagnosis of genital warts with that of the general female population without genital warts.
Methods Using the Danish nationwide population-based health data registers, we identified women between 15 and 45 years and followed them for diagnoses of CIN2+ from 1995 to 2006. Genital wart diagnoses were recorded from birth, and Cox regression with attained age as underlying scale was used to estimate age-dependent HRs for the risk of CIN2+ with genital warts as a time-varying exposure.
Results Among 918 609 women without genital warts and 32 218 women with genital warts, 30 209 and 1533 women, respectively, had a subsequent diagnosis of CIN2+. A significantly higher risk of CIN2+ was found among women with genital warts relative to those without (HR, 2.43; 95% CI 2.30 to 2.56). Treatment-resistant genital warts posed a significantly higher risk of CIN2+ than did transient genital warts (HR, 1.20; 95% CI 1.01 to 1.43). The risks remained elevated more than 4 years after the genital wart diagnosis.
Conclusion Clinicians should ensure that women with genital warts are screened for cervical cancer after the genital wart diagnosis and that they continue to be screened on time.
- genital warts
- cervical cytology
- hpv
- epidemiology (general)
- anogenital cancer
Statistics from Altmetric.com
Key messages
Genital warts are markers of subsequent long-term elevated risk of cervical intraepithelial neoplasia grade 2 or worse.
The risk is particularly high within 1 year after the genital wart diagnosis, among women <23 years and if the warts are hard to treat.
A diagnosis of genital warts is a good reason to ensure that women are screened on time.
Background
Cervical cancer is a major public health concern worldwide. It is preceded by a long phase of precancerous lesions, collectively referred to as cervical intraepithelial neoplasia (CIN) categorised into grades 1, 2 and 3 with increasing severity. Without treatment more than 20% of CIN2/3 will progress to carcinoma in situ or cancer,1 but through detection and treatment of cervical precursor lesions, cervical cancer screening programmes have substantially decreased the incidence and mortality of cervical cancer. In Denmark women aged 23–49 years are invited for cervical screening free of charge every third year, and after that they are invited every fifth year until the age of 64 years. Closer gynaecological surveillance is recommended only in the presence of cellular abnormalities.
Like CIN and cervical cancer, genital warts (GWs) are caused by human papillomavirus (HPV), which is transmitted through sexual contact. While the majority of all women become infected with HPV at some point during their lifetime, only a minority ultimately go on to developing clinical disease. This suggests that additional risk factors are involved in the pathogenesis of cervical precancerous lesions and cervical cancer. Previously, we have demonstrated an association between GWs and increased risk of cervical cancer.2 However, since screening could considerably affect the incidence of cervical cancer, studies of precancerous lesions may provide a more exact estimate of the actual association. So far, knowledge on the associations between GWs and cervical precancers has predominantly originated from case–control studies,3–10 and only rarely from cohort studies.11 These studies have been limited by small sample sizes, selected groups of women and/or lack of generalisability to the general population.
Since individuals with GWs have failed to clear the virus, they may be particularly susceptible to HPV. We hypothesised that this susceptibility is associated with increased risk of cervical dysplasia and cancer, and aimed to compare the incidence of CIN2 or worse (CIN2+) in women with GWs with that of the general Danish female population without GWs. To further test our hypothesis, we also compared the incidence of CIN2+ in women with treatment-resistant GWs with that of women with transient GWs. If GWs prove to be markers of increased risk of CIN2+, it may be reasonable to recommend closer gynaecological surveillance following a GW diagnosis.
Materials and methods
Since 1968, all citizens in Denmark have been assigned a unique 10-digit personal identification number (PIN) which contains information on date of birth and gender.12 The PINs are registered in the Civil Registration System, which also contains information on death and emigration of the citizens, and it is updated on a daily basis.12 The PIN is an integral part of the Danish society and is used in all health registers, enabling accurate linkage between them.
From the Danish Civil Registration System,12 we identified all women in Denmark 15–45 years of age during January 1995–October 2006. Information on a diagnosis of GWs was obtained from the Danish National Patient Register and through redemptions of a prescription for podophyllotoxin in the Danish National Prescription Registry. Women were considered without GWs until the first diagnosis of GWs in the National Patient Register or first prescription of podophyllotoxin in the Prescription Registry, whatever came first. The National Patient Register contains information on all diagnoses made in public and private hospitals in Denmark—inpatient admissions since 1978 and outpatient admissions since 1995—while the Prescription Registry holds information on all redeemed prescriptions since 1995. Because the notification of GWs is not compulsory in Denmark, we used prescriptions of podophyllotoxin as an indicator of GWs to capture cases that were diagnosed outside the hospitals by general practitioners and practising medical specialists. Podophyllotoxin is used exclusively to treat GWs and is the first-line treatment against GWs in Denmark. All cases of GWs diagnosed at hospitals are registered in the National Patient Register.
The Danish Pathology Data Bank covers all pathology data from the entire country. From this registry we retrieved information about cervical cytological and histological examinations. Women with and without GWs were linked to the Danish Pathology Data Bank and followed for occurrence of CIN2+. HPV vaccination status was not taken into account because in Denmark the first HPV vaccine was licensed in October 2006, the end of our study period.
Statistical analyses
We included only women with cervical cytology and/or histology examination data during follow-up in our cohort in order to take into account potential selection bias due to screening. To include only CIN2+ lesions which developed after GWs, as CIN2+ theoretically could have been present some time before diagnosis, we used a conservative estimate on when the outcome occurred; person-time was counted until the last normal (defined as ≤CIN1) cervical examination, and for women with subsequent CIN2+ the date of the CIN2+ diagnosis was defined as the date of the last normal cervical examination prior to CIN2+. The median time from the last normal cervical examination (≤CIN1) to CIN2+ for women with GWs was 43 days. The women were followed until October 2006, emigration, death, 45th birthday, CIN2+ or last normal examination, whichever came first. We excluded women with GWs, conisation or CIN2+ before their 15th birthday or 1 January 1995.
We also analysed the data using the entire cohort as our study population. In this sensitivity analysis, we assumed that women without cervical cytology and/or histology examination data during follow-up did not have CIN2+. Since the results of this analysis were similar to our primary analysis, we only present the results of the primary analysis.
Cox regression with attained age as underlying scale was used to estimate age-dependent HRs and corresponding 95% CIs describing differences in the risk of CIN2+ between women with and without GWs, with GWs as a time-varying exposure. To estimate the risk of CIN2+ according to time since first GW diagnosis, time since GWs was included as a second scale in the Cox model with the levels 0–1 years, 1–2 years, 2–3 years and >4 years. Because sexual risk behaviour may differ between women who are screened opportunistically and women attending organised screening for cervical cancer, we stratified according to attained age (<23 years and ≥23 years). Each woman contributed person-time to each combination of exposure (no GWs, GWs), time since GWs and age group according to the time spent in each of these.
We further considered the risk of subsequent CIN2+ among women with treatment-resistant GWs and transient GWs. Treatment-resistant GW cases were defined as episodes of GWs lasting at least 90 days from onset to the end of the last episode beginning within the first year after initial diagnosis. For this analysis a prescription of podophyllotoxin was considered to represent 1 month of treatment. Because the first year after initial GW diagnosis was used to define treatment-resistant cases, follow-up started 1 year after initial GW onset in this analysis (earliest at age 16 years), and women with a diagnosis of CIN2+ within the first year after GWs were excluded, as were women who had less than 1 year of follow-up after the initial GW episode, because they did not contribute risk time. In addition to analysing the relative risks of CIN2+ (high-grade dysplasias (CIN2/3) and cancer), all analyses were conducted with CIN3+, and CIN2/3 alone as outcomes, but since the results were similar we primarily present the results with CIN2+.
Statistical analyses were performed using R Statistical Software V.3.2.2.
Results
During our study period of more than 20 years (January 1995–October 2006), a total of 1 140 199 women between the ages of 15 and 45 years were identified (figure 1). We excluded 9 women with GWs, 5759 women with conisation and 4717 women with CIN2+ before 1 January 1995 or their 15th birthday. After further exclusion of 209.313 women without a cervical examination during follow-up and 1.436 women without a cervical examination between the start of follow-up and CIN2+, our final study population comprised 918 609 women.

Flow chart. CIN2+, cervical intraepithelial neoplasia grade 2 or worse; GWs, genital warts.
The study population of 918 609 women was followed for a median of 11.75 years, during which 32 218 (3.5%) had GWs. Seventy-two per cent of the women with GWs were identified through a prescription of podophyllotoxin, 15% through a hospital diagnosis of GWs and 13% from both sources. A flow chart of the study population with crude incidence rates of GWs and CIN2+ is presented in figure 2. Incidence of CIN2+ was 358 per 100 000 person years among women without GWs, while it was 926 per 100 000 person years among women with GWs.

Crude incidence of cervical intraepithelial neoplasia grade 2 or worse (CIN2+) among women with (+) and without (−) genital warts. Incidence rates are presented per 100 000 person years.
Among women with GWs who were subsequently diagnosed with CIN2+, 20% of CIN2+ cases appeared during the first year following GWs, 14% experienced CIN2+ 1–2 years after GWs, 13% 2–3 years after GWs, 12% 3–4 years after GWs and 40% more than 4 years after the GW diagnosis. Women younger than 23 years contributed 48% of the total person-time.
Risk of CIN2+ after GWs
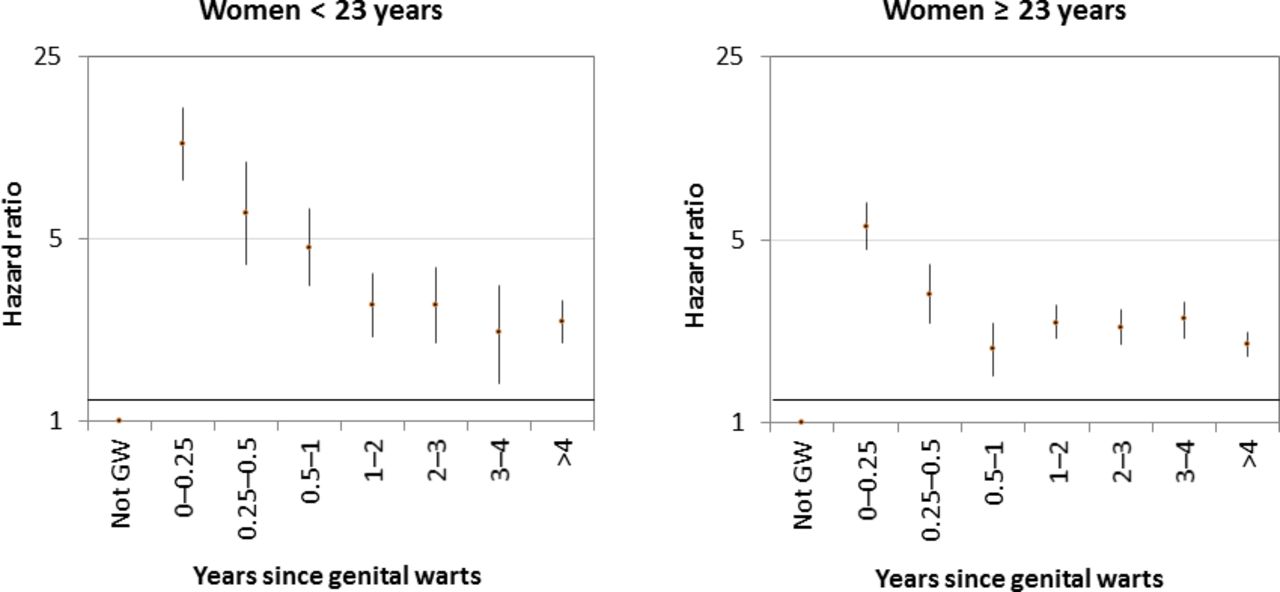
In the first part of our analyses, we found that the risk of CIN2+ was significantly elevated among women with a diagnosis of GWs relative to those without (HR, 2.43; 95% CI 2.30 to 2.56). The HRs were significantly (p<0.01) higher for women younger than 23 years (HR, 3.08; 95% CI 2.74 to 3.45) than in women 23 years and older (HR, 2.30; 95% CI 2.16 to 2.44), but the trends of CIN2+ risk according to time since GWs were similar for the two age groups (figure 3); the highest HRs were found within the first year of GW diagnosis, and although they declined with increasing follow-up women with GWs were consistently at statistically significantly increased risk of CIN2+ compared with women without GWs throughout more than 4 years of follow-up.

Relative risk of cervical intraepithelial neoplasia grade 2 or worse (CIN2+) according to time since genital warts (GWs) for women with versus without GWs. The horizontal line corresponding to an HR of 1 indicates no differences in risk of CIN2+ between women with and without GWs.
Women with GWs attended cervical cancer screening slightly more often than women without GWs (relative risk<23 years: 1.69, 95% CI 1.67 to 1.73; RR≥23 years: 1.34, 95% CI 1.33 to 1.35).
When we repeated the analyses for the total female population, that is, without requiring a cervical cytology and/or histology examination (sensitivity analysis), we found similar results for the two populations in almost all analyses. Only the relative risk of CIN2+ less than 1 year after GW diagnosis for women with GWs versus without GWs was substantially lower for the screened population compared with the total population (data not shown).
Risk of CIN2+ after treatment-resistant GWs
The second part of our analyses was based exclusively on women with GWs. After exclusion of 313 women with CIN2+ within 1 year of GW diagnosis and 3689 women with less than 1 year follow-up after GWs, the remaining 27 860 women constituted our study population. Of those, 10% were categorised as having treatment-resistant GWs, according to our predefined criteria. In figure 4, a flow chart of this study population shows the crude incidence rates of CIN2+ among women with transient and treatment-resistant GWs, respectively. In the Cox analysis where age was taken into account, a significantly higher risk of CIN2+ was found among women with treatment-resistant GWs relative to those with transient GWs (HR, 1.20; 95% CI 1.01 to 1.43). The elevated relative risk did not vary significantly according to time since GWs (p=0.92).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Crude incidence of cervical intraepithelial neoplasia grade 2 or worse (CIN2+) among women with transient and treatment-resistant genital warts. +Genital warts: transient genital warts; ++genital warts: treatment-resistant genital warts. CIN2+ incidence rates are presented per 100 000 person years.
Finally, repeating the analyses with CIN3+ as outcome produced virtually identical results; for example, HR was 2.27 (95% CI 2.13 to 2.42) for women with GWs versus women without GWs. Similarly, the analyses using CIN2/3 as outcome did not change the results; for example, the HRs were 2.46 (95% CI 2.33 to 2.59) for women with GWs versus women without GWs and 1.20 (95% CI 1.00 to 1.43) for women with treatment-resistant GWs versus women with transient GWs.
Discussion
In this nationwide study of more than one million women from the general population, a diagnosis of GWs was significantly associated with a long-term increased risk of CIN2+. The risk was highest 1 year after the GW diagnosis but continued to be statistically significantly increased up to 4 years and longer since the GW episode, and women with treatment-resistant GWs presented a higher relative risk of CIN2+ than did women with transient GWs. It should be noted that our study period ended before HPV vaccination was introduced into the Danish children’s vaccination programme. Our results will therefore be modified with an HPV vaccination programme in place.
In line with our findings, a smaller cohort study from Brazil (n=846)11 reported that women with GWs had a fourfold increased risk of cervical squamous intraepithelial lesions up to 2 years after the GW diagnosis. Our findings also agree with the majority of case–control studies.3 5 6 8–10 With an OR of 3.9 (95% CI 2.5 to 7.7), a large case–control study from Beijing5 found GWs to be one of the most important risk determinants of high-grade squamous intraepithelial lesions. In addition, a Danish interview-based case–control study (n=8373)10 found that women with a history of GWs were significantly more likely to report ever having had an abnormal Pap smear compared with women with no history of GWs (OR=1.9; 95% CI 1.6 to 2.3). The potential link between GWs and CIN2+ is further supported by our findings in the present study of increased CIN2+ risk according to increased severity of the warts. Only a few, smaller case–control studies did not confirm our results.4 7
Our findings may be explained by biological and/or behavioural factors. One biological explanation is host genetic variability. The small proportion of women with HPV infection who progress to develop the disease may do so because they carry specific genetic variations that alter the immune response to HPV, making them particularly susceptible to the infection. This hypothesis is supported by twin studies13 and by reports demonstrating heritability of CIN and cervical cancer in first-degree relatives.14–17 Many different genetic variations have been associated with cervical cancer,18 but the exact genes involved in susceptibility to cervical cancer and the potential interaction between them are still largely unknown.
Another biological hypothesis that could explain part of the elevated risk of CIN2+ in women with GWs is if local immunosuppression of cells in and around the GW lesions results in higher sensitivity of these cells to new HPV infections.19 20 Particularly the excess risk shortly after the GW diagnosis might to some degree be associated with local immunosuppression, but whether it also affects the long-term increased risk is more uncertain.
The risk estimates shortly after the GW diagnosis were substantially higher than the long-term risk. This difference could indicate that the timing of the CIN2+ and GW diagnoses coincided, potentially because of concurrent infection with high-risk, oncogenic HPV types. Although GWs are caused by low-risk HPV types and are not precancerous, both high-risk and low-risk types may exist in GWs.21 It usually takes a few years for CIN2+ to develop after initial infection with high-risk HPV types22 23; thus, the elevated risk of precancerous lesions identified in this study shortly after GWs could potentially be explained by coinfection with high-risk HPV types at time of GW diagnosis. However, defining the date of CIN2+ as the date of the last ‘normal’ (≤CIN1) cervical examination may have reduced the likelihood of coinfection as an explanation for our results.
Behavioural confounding could also contribute to some of the differences in the risk of CIN2+ observed between women with and without GWs. The number of sexual partners is one of the most important risk factors identified for cervical cancer and precancer.24 Other lifestyle factors like smoking, hormonal contraceptives and previous exposure to other STDs (eg, Chlamydia t rachomatis, Trichomonas vaginalis) have also been associated with the development of cervical abnormalities.5 25 26 If women with GWs have a higher prevalence of these behavioural risk factors than women without GWs, it could explain part of the observed excess risk among women with GWs. Also, the differences in risk of CIN2+ between women with GWs who have and have not yet entered the cervical cancer screening programme (younger and older than 23 years) might be explained by behavioural confounding, although biological differences cannot be excluded. On the other hand, we know that studies which were able to adjust for some of these factors5 15 show similar results as us, suggesting that behavioural confounding may not be the only explanation.
This study stands out from previous studies on associations between GWs and high-grade cervical lesions/dysplasia in several ways. In contrast to most other previous studies, this is a cohort study, and to our knowledge it is by far the largest cohort study to date. The high number of participants enabled us for the first time to demonstrate differences between women with GWs according to severity of the GW episode. The study has a particularly long follow-up period (median of almost 12 years), and because of the completeness of the Danish registries we had virtually no loss to follow-up. Finally, the results of this population-based and nationwide study are generalisable to the entire population.
The study also had limitations that should be acknowledged. Minor misclassification of GWs may exist because we were not able to detect GW episodes in individuals treated outside the hospitals with treatments other than podophyllotoxin. However, during our study period, podophyllotoxin has been the first-line treatment against GWs in Denmark, so we expect the vast majority of women with GWs in this study to be identified by their first diagnosis. Some misclassification of treatment-resistant GWs may have occurred since some patients with treatment-resistant GWs after a while will receive other treatments, for example, imiquimod. However, in clinical practice patients are most often treated with podophyllotoxin for several months before changing to another treatment modality, and if treatment is initially successful but the warts recur podophyllotoxin will again be the treatment of choice. Another potential limitation was the lack of information about HPV status, HPV types, educational level and lifestyle factors (eg, sexual behaviour, smoking and so on) that could increase the risk of CIN2+. Finally, surveillance bias could not be completely avoided, since women with GWs did attend cervical cancer screening more often than women without GWs, which would increase the chance of detecting precancerous lesions. However, because we excluded women without a cervical examination and defined the date of the CIN2+ diagnosis as the date of the last normal cervical examination prior to CIN2+, we believe to have minimised the risk of surveillance bias.
In conclusion, GWs seem to be predictors of a continuously elevated risk of CIN2+ more than 4 years after the GW diagnosis. For the clinician it is not crucial whether biological or behavioural mechanisms are the true explanation for these results. Based on our findings, a diagnosis of GWs may be a good reason to ensure that the woman is screened on time. In addition, it may be warranted to vaccinate women with GWs against HPV to reduce the risk of a subsequent infection,27 since women developing GWs (particularly women with treatment-resistant GWs) seem to be more vulnerable to HPV-related diseases than others.
References
Footnotes
Handling editor Francesca Ceccherini Silberstein
Contributors The authors agree to be accountable for all aspects of this work. All authors have contributed substantially to the design of the work, acquisition, analysis and interpretation of data, and they have either drafted (MB) or critically revised the work (SKK, CD). All have approved the final version.
Funding This work was supported by funding from the Mermaid-2 project. The sponsor of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report. The corresponding author had full access to all the data and had final responsibility for the decision to submit for publication.
Competing interests SKK has received speaker’s fee from Sanofi Pasteur, MSD and Merck, scientific advisory board fee from Merck, and research grant through her institution from Merck.
Patient consent for publication Not required.
Ethics approval The study was approved by the Danish Data Protection Agency (reference number 2014-41-2917).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.