Article Text

Statistics from Altmetric.com
Individuals globally have experienced seismic shifts in their day-to-day lives due to measures adopted by governments to tackle the COVID-19 pandemic. ‘Lockdowns’ have confined individuals to their homes, removing protective factors and access to key services. Previous public health emergencies exacerbated existing gender and intersectional inequalities1 2 and organisations warned of increased gender based violence and domestic abuse (DA).1 Such concerns have been realised with UN chief calling for action against a ‘horrifying global surge in domestic violence’.3 The UK ‘locked-down’ on 23 March 2020 and a Home Affairs Committee report described marked increases in calls to the national DA helpline,4 with escalations in violence and coercive control.4 Fourteen women and two children were reported killed by men between 23 March and 12 April, double the 3-week average.4
National guidance5 recommends routine enquiry about DA.5 Our service had successfully embedded this practice pre-COVID-19, with staff skilled at asking about DA, identifying survivors and managing disclosures safely as part of routine care. Following lockdown, Integrated Sexual Health (ISH) services throughout the UK underwent rapid service reconfiguration in order to follow social-distancing guidelines, protect patients and staff and manage COVID-19 related staff redeployment. Clinical capacity was reduced, the majority of consultations moving rapidly to remote telephone consultation. We aimed to compare the rates of DA enquiry and disclosure prelockdown and postlockdown.
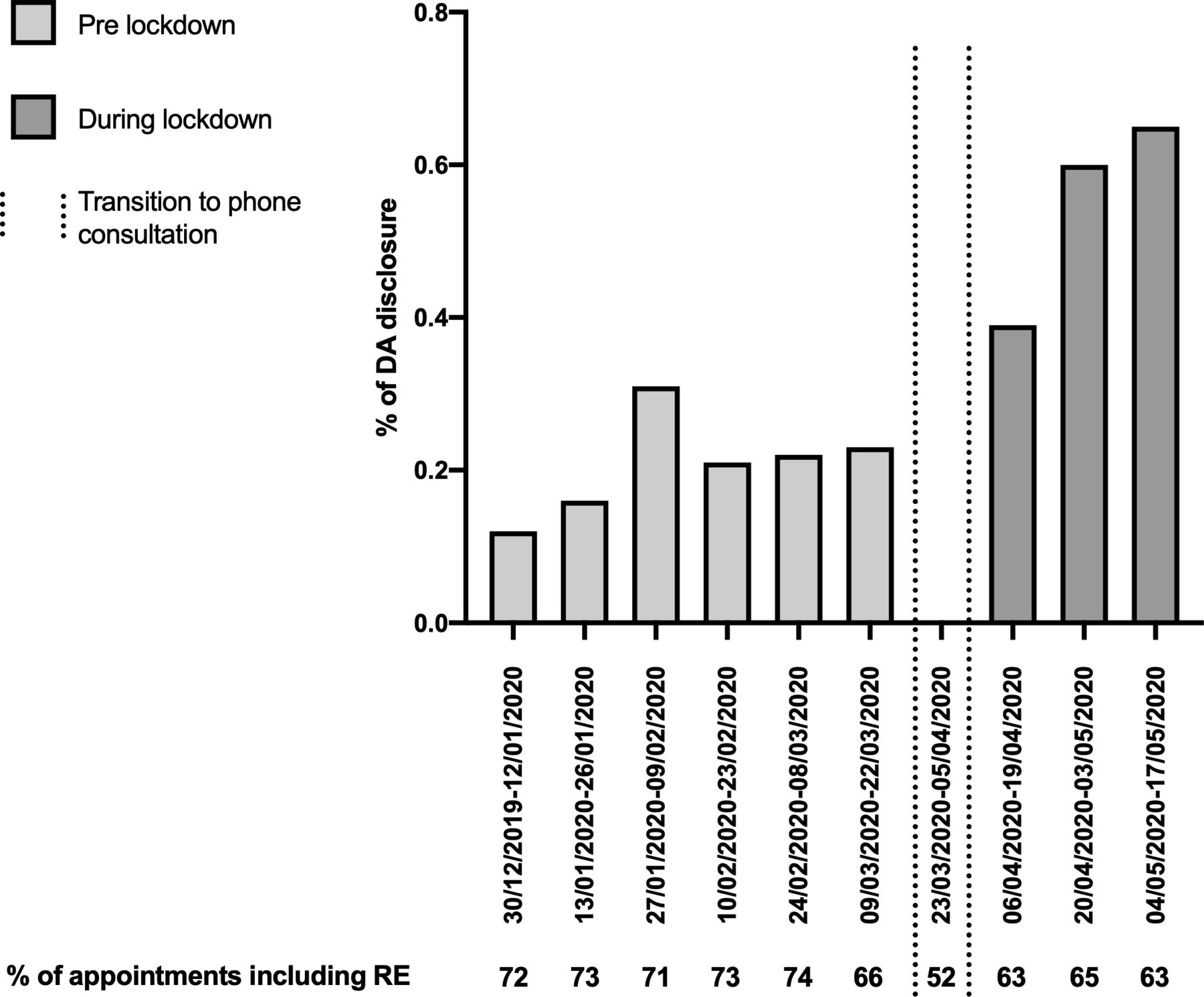
Data from evaluation of services in London and Surrey were analysed anonymously and in aggregate in Excel and STATA. This revealed a reduction in the percentage of consultations including enquiry about DA (decreasing from 66% between 09/03/20 and 22/03/20 to 52% between 23/03/2020 and 05/04/2020), accompanied by a complete absence of disclosures in the latter period (figure 1). Targeted interventions addressing this lack of disclosure included awareness-raising and ensuring service-users were routinely asked whether they were alone and could speak freely at the start of consultations. There was an increase in the proportion of consultations including routine enquiry, from 52% to 63% in the following weeks. An increase was also recorded in the percentage of DA disclosures over 6 weeks of lockdown (06/04/2020–17/05/2020), compared with the 6 weeks prior to lockdown (10/02/2020–22/03/2020), an increase from 0.22% (CI 0.14% to 0.32%) to 0.57% (CI 0.33% to 0.91%) (p=0.002, χ²) (figure 1).

{kind=link}
Percentage of appointments including routine enquiry about DA and percentage of disclosures of DA during appointments by 2-week time period before and after lockdown. DA disclosures increased in 6 weeks of lockdown (06/04/2020–17/05/2020), compared with 6 weeks prior to lockdown (10/02/2020–22/03/2020). Increase from 0.22% (CI 0.14% to 0.32%) to 0.57% (CI 0.33% to 0.91%) (p=0.002, χ² test). Sensitivity analysis comparing disclosures in 8 weeks of lockdown (23/03/2020–17/05/2020), with 8 weeks prior to lockdown (27/01/2020–22/03/2020) found an increase in the proportion of disclosures 0.24% (CI 0.17 to 0.33) to 0.46% (CI 0.27% to 0.73%) which also reached statistical significance (p=0.027, χ² test). Disclosures were similar when comparing the 6 weeks prior to lockdown with the previous 6 weeks, confirming validity of assumptions as to baseline. DA, domestic abuse; RE, routine enquiry.
In summary, we report an increase in the percentage of disclosures of DA within an ISH service using mainly telemedicine during ‘lockdown’ and rapid improvements in detection following awareness-raising and training. Disclosures were managed according to local safeguarding polices. Increased disclosure was observed despite potential barriers to accessing clinic appointments and to disclosing affecting those experiencing DA, particularly those in coercive and controlling situations. Disclosure rates were high despite concerns over obstacles to disclosure via telephone consultation, including challenges in building rapport, lack of opportunity to respond to visual signs and non-verbal cues and reluctance to disclose DA over the phone due to real or perceived lack of safety to do so. Our experience provides evidence of effective routine enquiry and safeguarding via telemedicine, lending weight to calls to extend routine enquiry to other settings as part of a public health approach to DA during the ongoing pandemic and any future lockdowns.2
Footnotes
Twitter @rob_aldridge
Contributors All authors contributed substantially to the conception of the work. DW, DT and JA were responsible for the acquisition of data. DW, RWA and SJW analysed the data. SJW wrote the article and produced the figure. DW, DT, RWA and JA contributed to manuscript preparation and revision. All authors reviewed and interpreted the results, contributed to the final editing of the manuscript and agreed to be accountable to all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.