Article Text

Abstract
Objective Sexual minority men (SMM) of colour are disproportionately impacted by HIV and bacterial STIs (bSTIs). To better understand within-group heterogeneity and differential risk factors by race and ethnicity, we sought to examine rates of undiagnosed HIV and rectal bSTI at the intersection of racial and ethnic identity with other sociodemographic factors.
Methods We examined data from 8105 SMM conducting home-based self-testing at enrolment in a nationwide cohort study collected from November 2017 to August 2018. We conducted analyses stratified by racial and ethnic groups to examine within-group (ie, subgroup) unadjusted rates of HIV and rectal bSTI infection across a range of characteristics.
Results Rates of undiagnosed HIV were highest among Black (4.3%, n=39) and Latino (2.4%, n=38) SMM, with lower rates among those identified as multiracial (1.6%, n=15), white (1.3%, n=56) and other races (1.3%, n=6). Across the stratified analyses of HIV infection, 15 significant associations emerged showing that age, region, insurance type, sexual positioning and incarceration history had differential impacts across racial and ethnic groups. In particular, private and public insurance were protective against HIV for white but not Black and Latino SMM, and incarceration was associated with substantially higher rates of HIV infection for Black and Latino SMM relative to white SMM. We found significant co-occurrence of HIV and bSTI rates for participants who identified as Latino (OR=7.5, 95% CI 2.12 to 26.54), white (OR=3.19, 95% CI 1.14 to 8.98) and multiracial (OR=5.5, 95% CI 1.08 to 27.90), but not those who identified as Black (OR=0.82, 95% CI 0.10 to 6.56) or other races (OR=3.56 95% CI 0.31 to 40.80).
Conclusions Stratified analyses showed differential rates of HIV infection at the intersection of racial and ethnic groups with other characteristics, particularly insurance status and incarceration history, pointing to structural inequities rather than individual behaviours underlying disproportionately high rates of HIV for Black and Latino SMM.
- HIV
- HIV seroprevalence
- epidemiology
- bacterial infections
Data availability statement
Data are available for non-commercial purposes by contacting the corresponding author and establishing a data transfer and use agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sexual minority men (SMM) are disproportionately affected by HIV and other STIs.1 In 2017, SMM accounted for 70% of all new HIV diagnoses in the USA.2 In the same year, prevalence rates of two rectal bacterial STIs (bSTIs)—Neisseria gonorrhoeae (NG) and Chlamydia trachomatis (CT)—were 14.7% and 16.8%, respectively, among SMM.3 Research has demonstrated strong co-occurrence of rectal bacterial STI (bSTIs) and HIV,4 5 likely due to both the sexual practices associated with acquiring each and that rectal bSTIs biologically increase risk of HIV transmission through local immune response.6–8 The Centers for Disease Control and Prevention (CDC) recommends that SMM engaging in receptive anal sex receive annual rectal bSTI screening,9 though urogenital screening has persisted as the most common anatomical testing site.10 As a result, individuals with active rectal bSTI go untreated when a urogenital-only screening result is negative.11
Among SMM, the burden of HIV and bSTIs disproportionately impacts racial and ethnic minority subgroups, which research consistently demonstrates to not be attributable to higher behavioural risk. The lack of a behavioural explanation for disproportionate rates among SMM of colour suggests these disproportionate rates are driven by extraindividual factors, including inequities at the intersection of sexual minority and racial/ethnic statuses.12 13 Although surveillance data capture HIV and STI disparities between different racial and ethnic subgroups, they lack information on most other sociodemographic characteristics. Thus, little research has been powered to identify intersecting disparities by looking at subgroups within each racial and ethnic group that may shed light on the role of structural inequities. The CDC’s national HIV and STI surveillance data are limited to sex, age, race/ethnicity, geographical location and sex of partners,14 which are broad and make analysis of within-group differences and inequities difficult. In order to conduct such analyses, it is necessary to capture key factors that may intersect with racial and ethnic identity, such as socioeconomic factors, medical and prevention access, interaction with the carceral system, and behavioural factors like substance use. Likewise, a large sample would be needed in order to detect significant subgroup differences.15
Advances in technology have led to the emergence of large-scale cohort studies combining epidemiological and social/behavioural methods to produce large datasets with which to estimate prevalence and incidence while also having more nuanced sociodemographic and behavioural data.16 Such technology-based cohort studies provide the opportunity to better understand subgroup differences among those most affected by the domestic HIV epidemic, particularly Black and Latino SMM. The goal of the present study was to use data from an observational HIV prevention cohort study to examine within-racial/ethnic group (ie, subgroup) sociodemographic differences in rates of undiagnosed HIV and bSTI. Overall, we sought to better understand how various sociodemographic and behavioural characteristics intersect with racial and ethnic identity to influence inequities in infection.
Methods
The present study uses baseline data from UNITE (Understanding New Infections through Targeted Epidemiology), a nationwide cohort study prospectively following SMM to better understand risk of HIV seroconversion.17 UNITE involved routine surveys and annual HIV testing and was available in Spanish and English to SMM aged 16 and over. All procedures were reviewed and approved by the institutional review board of the City University of New York.
Participants and procedures
Participants were 8105 SMM recruited between November 2017 and September 2018 using online strategies across a range of venues, including geosocial networking apps, social media sites, website referrals and email blasts. Participants completed a brief screening survey to determine eligibility: (1) were 16 years of age or older; (2) identified as HIV-negative or unknown status; (3) identified their gender as male; (4) identified with a sexual minority identity (ie, gay, queer or bisexual); (5) lived in one of the 50 US states, DC, or Puerto Rico; (6) were recruited from or reported using geosocial networking apps to meet partners; and (7) reported risk of HIV as previously described in detail.17 18
After providing contact information, eligible participants were emailed a link to the enrolment survey. The survey began with watching a 5 min video detailing key information about the study and completing informed consent or assent, followed by completing a survey containing a range of measures about sociodemographic characteristics, psychosocial well-being, and HIV and STI prevention. Participants were then mailed their at-home testing kit. In addition to receiving an oral fluid-based HIV test kit, half of the sample was randomly assigned to also receive a rectal swab-based bSTI test kit as well. The OraSure HIV-1 Oral Specimen Collection Device19 was used to gather oral samples, and the Hologic Aptima swab specimen collection kit20 was used with rectal samples for NG/CT testing. To complete testing, participants were sent a link to a survey that contained an instructional video on how to perform the oral fluid collection and, when relevant, the rectal swab. Participants placed samples into a self-addressed return envelope to our laboratory partner, the Alameda County Public Health Laboratory, where they were batch processed and results were returned to our study team via a secure portal. On receipt of the sample for HIV testing by the lab, the participants were compensated with a $25 Amazon e-gift card.
The final sample of enrolled participants (n=7957) excludes participants with a positive result at baseline, though the present analyses include 148 participants who received a positive HIV test result at baseline (N=8105). Moreover, bSTI tests were randomly sent to half of the participants as noted earlier, and thus the analytical sample for those analyses was a subset of the larger sample (n=3279).
Variables and measurement
Demographics
Participants reported sociodemographic information including age, race and ethnicity, sexual identity, geographical location, insurance, education and relationship status.
Incarceration history
A single item with a dichotomous yes/no response scale assessed incarceration history: ‘Have you ever been incarcerated (prison, jail or juvenile detention)?’
Preferred sexual position
Participants reported preferred sexual position by responding to the question ‘Which sexual position would you say you identify most as?’ Response options were ‘top’, ‘versatile/top’, ‘versatile’, ‘versatile/bottom’ and ‘Bottom’.
Recent HIV test
Participants reported their most recent HIV test by responding to the question ‘When was the last time you had an HIV test?’ Response options were ‘within the last month’, ‘about 1–3 months ago’, ‘about 3–6 months ago’, ‘about 6–12 months ago’, ‘about 1–2 years ago’, ‘more than 2 years ago’ and ‘I’ve never been tested’.”
Statistical methods
Descriptive statistics were estimated using SPSS V.24. Contingency table analyses were conducted using a likelihood-ratio test (ie, G 2), stratified by racial and ethnic groups, to examine within-racial/ethnic group differences in HIV and rectal bSTI rates by a range of sociodemographic and behavioural characteristics (ie, age, region, education, insurance status, sexual identity, relationship status, metropolitan area, HIV testing history, sexual position and incarceration history). Participants in the ‘other’ race category were those who identified as Asian, Native American or Alaskan Native, Native Hawaiian or Pacific Islander due to insufficient sample sizes of each group. Across analyses, we followed standard practice and suppressed the inclusion of certain group categories in analyses when the overall number of infections in that group was below 16.21 Completion of the full survey and HIV testing were required for enrolment, as such participants were not missing data on key variables of interest.
Results
A study flow diagram is presented in figure 1 and descriptive sample characteristics by racial and ethnic identity are displayed in table 1. The analytical sample included 8105 SMM who completed the survey and HIV testing, of whom 7957 received a negative result and were fully enrolled in the cohort for longitudinal follow-up; of those, 3279 were selected for and completed rectal bSTI testing. The sample was diverse, with more than half identifying as men of colour, one-fifth having no insurance, slightly more than one-third being from the Southern USA and 1 in 10 having a history of incarceration.

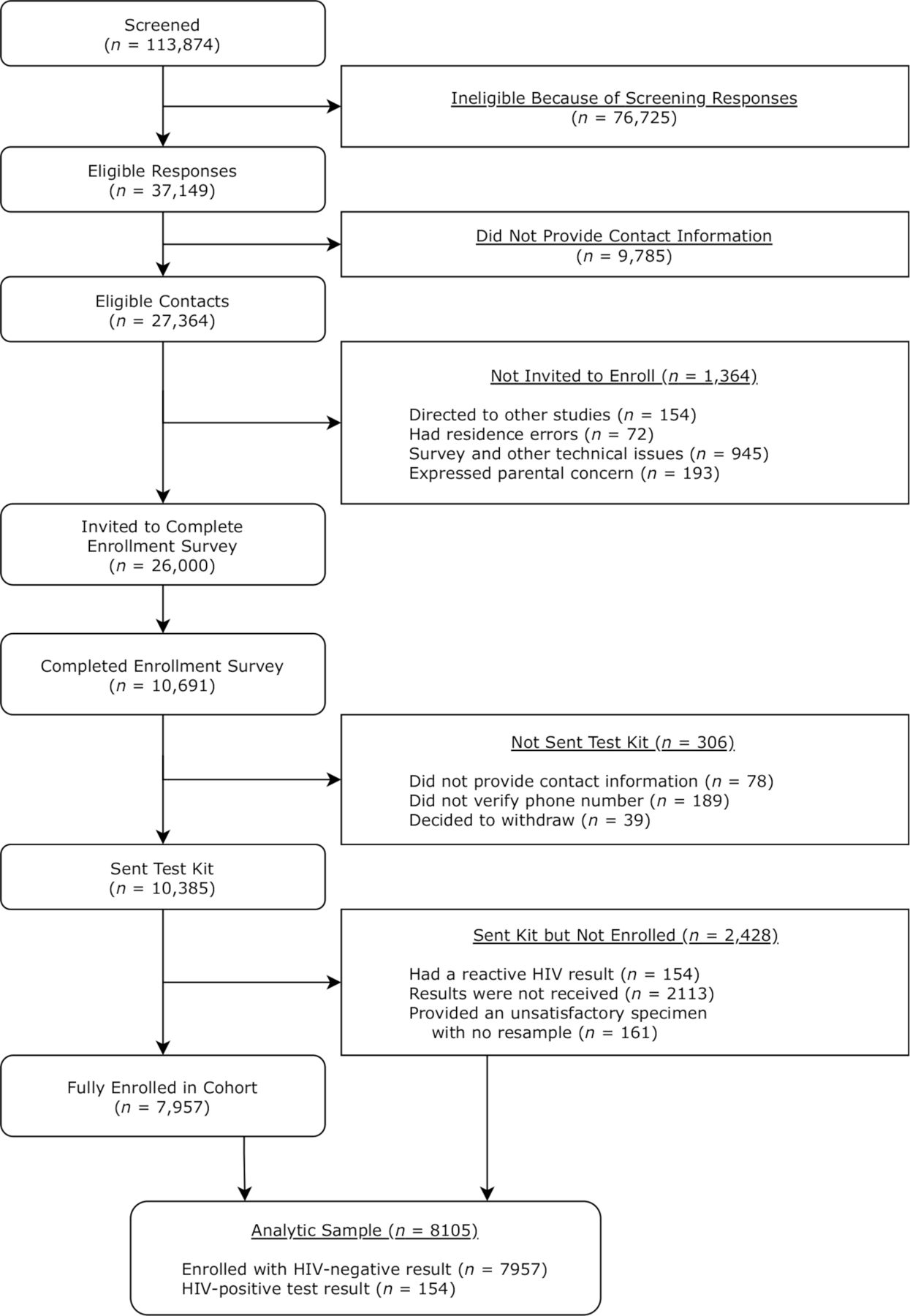{kind=link}
Number of participants who completed each step required for enrolment in UNITE (Understanding New Infections through Targeted Epidemiology), including home-based sampling for lab-based HIV and rectal bacterial STI testing.
Characteristics of the study sample (N=8105)
Overall rates of undiagnosed HIV were highest among Black participants (4.3%, n=39), followed by Latino (2.4%, n=38) and multiracial (1.6%, n=15), with the lowest rates among those who identified as white (1.3%, n=56) or with another race (1.3%, n=6). Table 2 displays sociodemographic differences in rates of undiagnosed HIV infection within (ie, stratified by) each racial and ethnic group. In total, 15 significant demographic associations emerged across the stratified analyses, 4 among Black, 3 among Latino, 4 among white, 3 among multiracial and 1 among participant of another race/ethnicity. Significant disparities in HIV infection by age emerged only among Latino participants, showing a substantially lower rate among the 16–24 age range and higher rates among the 35–49 and 50+ age ranges compared with the overall trend. There were geographical differences only among Black participants, showing the rates of undiagnosed HIV were more heavily concentrated in the Northeast and South. For insurance status, differences among white participants suggested significant protective effects of both private and public insurance, which was lacking among other groups, and differences among multiracial participants actually showed an elevated rate of diagnosis among those with public insurance that was greater than that among uninsured multiracial participants. The recency of HIV testing was associated with infection rates among all racial/ethnic groups—rates were highest among the group who had tested more than 1 year ago, though this effect was substantially more pronounced among Black participants and least pronounced among white participants. The typically protective role of insertive ‘top’ sexual position identity was significant only among white participants. Pre-exposure prophylaxis use was associated only among participants who identified as Black, though the pattern largely mirrored that of other groups and was likely driven by the larger rate of infections among the group overall. Finally, a history of incarceration was associated with a greater rate of infection among Black, Latino and white participants, but was much more pronounced among Black and Latino men.
Subgroup unadjusted prevalence estimates for undiagnosed HIV infection at study entry (N=8105)
Overall rates of undiagnosed rectal STIs were highest among multiracial (15.9%, n=63) participants, followed by those who identified with another racial/ethnic background (12.6%, n=25) and Latino (12.4%, n=77), and lowest among those who identified as white (10.2%, n=172) or Black (9.9%, n=38). Table 3 displays sociodemographic and behavioural differences in rates of rectal bSTI infection within (ie, stratified by) each racial and ethnic group. In total, 12 significant demographic associations emerged within the stratified analyses, 2 among Black, 4 among Latino, 5 among white and 1 among multiracial participants, with none among participants of another race/ethnicity. Rectal bSTI rates differed by age among Black, Latino and white participants—across all three groups, the 16–24 age range had the highest rate of infections, with a more pronounced rate among Black and Latino SMM of this age range. There were significant differences in rates by geographical region and insurance status among only white participants, showing a markedly lower rate in the Northeast and a lower rate among those with public and private insurance than with none. Rates differed by whether participants lived in a major metropolitan area among only Latino participants, showing a reversed trend compared with other groups with lower rates among those from such areas. Recent HIV testing was associated only among multiracial participants, showing substantially higher rates of rectal bSTIs among those who had last tested more than a year ago or had never tested. Finally, sexual position was significantly associated with rates among Black, Latino and white participants, showing substantially lower rates of rectal bSTIs among top-identified participants.
Subgroup prevalence estimates for undiagnosed rectal bSTI infection at study entry (N=3279)
Finally, we conducted an exploratory analysis examining the co-occurrence of undiagnosed HIV and rectal bSTI stratified by racial/ethnic group and found they were positively associated for participants who identified as Latino (OR=7.5, 95% CI 2.12 to 26.54), white (OR=3.19, 95% CI 1.14 to 8.98) and multiracial (OR=5.5, 95% CI 1.08 to 27.90), but there was no evidence of co-occurrence for participants who identified as Black (OR=0.82, 95% CI 0.10 to 6.56) or other races (OR=3.56, 95% CI 0.31 to 40.80).
Discussion
In this paper, we analysed data from a large and diverse nationwide HIV prevention cohort of SMM to provide insights into HIV and rectal bSTI within racial and ethnic groups, examining rates of undiagnosed infections at the intersection of race and ethnicity with other specific sociodemographic, structural and access-related characteristics. Public health surveillance data highlight that the intersection of transmission risk category (ie, SMM) and race and ethnicity show evidence for the largest disparities, but have been unable to examine rates within subgroups among SMM stratified by race/ethnicity, with the notable exception of age group differences. In this study, we observed overall differences in rates by race and ethnicity, but were also sufficiently powered to examine the intersection of race and ethnicity with other key characteristics and found unique patterns among racial and ethnic groups. In addition to corroborating well-documented disparities by factors such as age and HIV testing frequency, subgroup-specific rates at the intersection of racial and ethnic identities with factors like insurance status and incarceration history provide evidence that pronounced racial and ethnic disparities often occur among SMM of colour experiencing social and structural inequities.
We identified only a single factor that was uniformly associated with rates of undiagnosed HIV infection across racial and ethnic groups of SMM—recency of HIV testing. Although the patterns were similar across racial and ethnic identities, they were substantially more pronounced among Black SMM, a finding that would be masked in typical searches for independent predictors. In particular, those who had tested at least once in their lives but more than 1 year ago had significantly elevated rates of undiagnosed HIV, with the highest rates among men who identified as Black (11.2%) or another race (ie, Asian, Native American or Alaskan Native, Native Hawaiian or Pacific Islander who had to be grouped due to sample sizes, 8.3%), moderately high among Latino (5.1%) and multiracial (4.6%) men, and lowest among white men (2.7%).
Other findings were similarly noteworthy due to their inconsistent patterns among racial and ethnic subgroups. In particular, insurance status was associated with undiagnosed HIV infection for participants who identified as white but not others. Results by insurance status suggested rates of undiagnosed HIV infection were highest among those with public insurance, even compared with those with no insurance, for all racial/ethnic groups except white men, for whom it was more protective than no insurance; the lack of significant association between insurance status and rates of infection for all other racial and ethnic groups also suggests no protective effect of private insurance, a phenomenon that emerged only among white men. Relatedly, we found differences in undiagnosed HIV rates by lifetime incarceration history among Black, Latino and white participants, though these were substantially elevated for Black (8.1%) and Latino (7.1%) as compared with white (2.9%) participants. These findings regarding disparate impact of insurance and incarceration by racial and ethnic group suggest that higher rates of HIV infection are inequities resulting from structural rather than individual factors, namely, inequitable access and systemic racism within these systems.22–25
Compared with undiagnosed HIV, there were distinct patterns for fewer disparities in rates of bSTI diagnoses. Rates were consistently highest among the youngest SMM, which was the inverse of the HIV findings, and identifying one’s sexual position as ‘bottom’ (ie, receptive) was more strongly associated with rates of bSTI diagnosis across racial/ethnic subgroups than it was for HIV. Despite a shared behavioural transmission pathway, these findings highlight discrepancies in the factors associated with HIV and bSTI diagnosis. In fact, exploratory analyses demonstrated that undiagnosed HIV and bSTI co-occurred, as would be expected, for Latino, white and multiracial participants, but not for those who identified as Black or another race. These findings underscore the importance of not only investigating rates of infection at the intersection of race/ethnicity and other sociodemographic factors but also testing models of risk separately for these groups to better understand the racial/ethnic disparities in HIV and bSTI infection for SMM. At the same time, the chronic nature of HIV versus the ability to recover from bSTIs both with and without treatment further complicates their comparison, particularly when looking at age differences where rates of HIV are cumulative and bSTIs are not.
Limitations
This study had numerous strengths, including its use of at-home testing with lab-confirmed results, a diverse sample across the USA, and a large enough sample to examine stratified rates of HIV and rectal bSTI infections, though it was not without limitations. In working to represent the groups most affected by the HIV epidemic among SMM, we had limited sample sizes for several racial/ethnic groups (eg, Asian, Native American or Alaskan Native, Native Hawaiian or Pacific Islander) and thus had to group them together for analyses. Although the study included adolescents, our sample sizes for the youngest age groups were low, particularly when stratified by race/ethnicity. We believe these results represent a greater diversity of SMM than those conducted specifically of clinic-based or exclusively urban samples, though the results nonetheless represent individuals who were willing to join a study that required receiving testing kits at home, and thus likely exclude those who might be more concerned about such procedures and risks to their privacy.
Conclusions
Though rates of undiagnosed HIV infection were higher for Black and Latino SMM, there was significant within-group variability in these rates when looking at the intersection of racial and ethnic identities with sociodemographic and other factors. Among Black, Latino and multiracial SMM, rates of undiagnosed HIV infection were higher among those with public insurance than those with no insurance, a trend that was reversed among white men. Similarly, a history of incarceration had an outsize impact on higher rates of undiagnosed HIV infection for Black and Latino relative to white SMM. Rates of HIV infection were highest among Black SMM, whereas rates of bSTI were lowest among this group, suggesting behavioural transmission risk factors are unlikely to sufficiently account for observed disparities in HIV diagnoses. Instead, these within-racial/ethnic group findings suggest that systemic racism and structural factors within the US healthcare and carceral systems produce not only an elevated but also an inequitable burden of HIV infection among Black and Latino SMM, among whom “protective factors” like insurance were both less common and less protective. Approaches to HIV surveillance must examine the intersection of racial and ethnic identities with other factors to develop a more nuanced approach to HIV prevention for SMM of colour and increased focus on policy and structural change is necessary to reduce inequities in the domestic epidemic.
Key messages
Black and Latino sexual minority men (SMM) had higher rates of undiagnosed HIV infection than white SMM, but rates of infection were influenced by different factors across groups, with particularly disparate impacts of insurance status and incarceration history for Black and Latino SMM relative to white SMM.
Within-group heterogeneity by race and ethnicity in terms of factors that influence rates of undiagnosed HIV infection point to structural inequities as driving forces behind disproportionately high infection rates for Black and Latino SMM.
Rates of undiagnosed HIV and bSTI infection were found to be significantly associated for most racial and ethnic groups, consistent with their shared behavioural route of infection, but rates were unassociated for Black SMM, which further underscores the role of non-behavioural factors placing Black SMM at heightened risk
Data availability statement
Data are available for non-commercial purposes by contacting the corresponding author and establishing a data transfer and use agreement.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the City University of New York (CUNY) integrated IRB (protocol #2017-0444)
Acknowledgments
We gratefully acknowledge the support of the National Institutes of Health, particularly our project scientists, Drs Gerald Sharp, Sonia Lee and Michal Stirratt. We acknowledge the contributions of other key members of the UNITE study team (Stephen S Jones, Juan Castiblanco and Ruben Jimenez) and all of the staff at Hunter College’s PRIDE Health Research Consortium. We are grateful for the time and contributions of Dr Mark Pandori and the Alameda County Public Health Laboratory. Finally, we thank all of our participants in the UNITE study.
References
Footnotes
Handling editor Henry John Christiaan de Vries
Twitter @nicotavella09
Contributors HJR was the study’s principal investigator and contributed to the study design, data collection and manuscript revisions. AT contributed to data collection, data interpretation, literature search and manuscript revisions. KMS contributed to data analysis, data interpretation and manuscript writing/revisions. NFT, BS and OS contributed to the data collection, literature search and manuscript writing/revisions. BM and CER-D contributed to the study design and manuscript revisions. All authors reviewed and approved the final submitted manuscript and are accountable for the accuracy and integrity of this work.
Funding This study was supported by a grant jointly awarded by the National Institute on Allergy and Infectious Diseases, National Institute on Mental Health, Eunice Kennedy Shriver National Institute on Child Health and Human Development, and National Institute on Drug Abuse (UG3-AI133674, principal investigator: HJR). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.