Article Text

Abstract
Background Self-collection of samples for diagnostic testing offers the advantages of patient autonomy, confidentiality and convenience. Despite data showing their feasibility and accuracy, there is a need to better understand how to implement such interventions for sexually transmitted infections (STIs). To support WHO guidelines on self-care interventions, we conducted a systematic review to investigate whether self-collection of samples should be made available as an additional approach to deliver STI testing services.
Methods Peer-reviewed studies were included if they compared individuals who self-collected samples for chlamydia, gonorrhoea, syphilis and/or trichomonas testing to individuals who had samples collected by clinicians on the following outcomes: uptake/frequency of STI testing, social harms/adverse events, positive yield (case finding), linkage to clinical assessment/treatment and reported sexual risk behaviour. We searched PubMed, CINAHL, LILACS and EMBASE for articles published through July 2018. Risk of bias was assessed using the Cochrane tool for randomised controlled trials (RCTs) and the Evidence Project tool for non-RCTs. Meta-analysis was conducted using random effects models to generate pooled estimates of relative risk (RR).
Results Eleven studies, including five RCTs and six observational studies with a total of 202 745 participants, met inclusion criteria. Studies were conducted in Australia, Denmark and the USA. Meta-analysis found that programmes offering self-collection of samples increased overall uptake of STI testing services (RR: 2.941, 95% CI 1.188 to 7.281) and case finding (RR: 2.166, 95% CI 1.043 to 4.498). No studies reported measuring STI testing frequency, social harms/adverse events, linkage to care or sexual risk behaviour.
Discussion While greater diversity in study designs, outcomes and settings would strengthen the evidence base, findings from this review suggest that self-collection of STI samples could be an effective additional strategy to increase STI testing uptake.
Prospero registration number PROSPERO CRD42018114866.
- sexually transmitted infections
- self-collection
- sti testing
- sti diagnosis
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Self-collected samples for sexually transmitted infection (STI) testing are as accurate as clinician-collected methods and are feasible and acceptable in a variety of populations.
What are the new findings?
A systematic review identified 11 studies from three high-income countries (Australia, Denmark and the USA), conducted in a variety of populations.
Meta-analysis showed that, compared with clinician-collection, self-collection of samples increased uptake of STI testing services.
In meta-analysis, the intervention group (people who were offered STI services with self-collection of samples) had a higher yield of positive diagnoses (ie, case finding) compared with the group offered only clinician-collected STI tests; however, when analyses were limited to those who accepted STI testing services (rather than all offered services), self-collection was associated with lower positive yield.
What do the new findings imply?
Self-collection methods can offer an alternative approach for STI testing, with implications for universal health coverage and the achievement of the UN Sustainable Development Goals.
Introduction
Worldwide each year, there are an estimated 357 million new infections of one of the four curable sexually transmitted infections (STIs): chlamydia, gonorrhoea, syphilis and trichomoniasis.1 2 Aetiological diagnosis via STI testing is the best way to ascertain infection status and promote appropriate treatment.3 4 While STI diagnostic tests are available and used in many high-income countries, diagnostic tests in low-income and middle-income country (LMIC) settings are largely unavailable.3 5–7 Syndromic management has been the primary approach for STI treatment in LMICs,5 8 which has significant limitations despite its practicality; experts doubt it will impact STI disease burden.5 9 10 Globally, social stigma and a lack of effective policies also affect STI testing uptake and treatment-seeking behaviour. Low STI testing coverage and high transmission rates are common among at-risk vulnerable adolescents and key populations including men who have sex with men (MSM), migrants, sex workers, Indigenous and minority populations and those affected by humanitarian emergencies.9 Left undiagnosed and untreated, curable STIs can cause acute and chronic illness, infertility, ectopic pregnancy, long-term disability, neurological and cardiovascular disease and death.11 Serious diseases in their own right, STIs also increase the risk of contracting or transmitting HIV infection.11 Consequently, greater efforts are needed to expand STI testing globally to reduce this heavy burden of disease.
Self-collection of samples is one way to facilitate the expansion of STI testing services. Self-collection of samples occurs when individuals take a specimen themselves, either at the clinic or elsewhere, and send it to a laboratory for testing.12 Follow-up in the case of positive test results requires a linkage with the health system. Research in high-income countries, where organised lab facilities and healthcare are available, shows that self-collected STI samples are as diagnostically accurate as clinician-collected samples13 and that self-collection interventions are feasible and acceptable in a variety of populations.14–23 Self-collection approaches also have the potential to address some common barriers to clinician-dependent and/or clinic-based diagnosis, such as concerns around autonomy, inconvenience, stigma and lack of privacy.5 24 25 Systematic reviews have been conducted to compare STI testing programmes (some including self-collection methods) in home or non-clinic settings to those in clinic settings.19 26–31 However, no review to date has systematically compared self-collection of samples to clinician-collected methods for STI testing on programmatic outcomes. In order to develop WHO guidance on self-care interventions for sexual and reproductive health and rights, we conducted a systematic review to investigate whether STI self-sampling should be made available as an additional approach to deliver STI testing services, whether incorporated into routine STI services or as an alternative model with linkage to care.
Methods
Definition
We assessed self-collection of samples for Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), Treponema pallidum (syphilis) and Trichomonas vaginalis (TV). This is in line with ongoing multicountry evaluations of promising point-of-care testing (POCT) interventions to detect these four curable STIs as well as the goal of the WHO STI POCT initiative to achieve universal access to reliable and affordable STI testing.32 There are numerous types of self-collected samples for different STIs, including: urine (mainly among men, but also women and youth) for NG, CT and TV; vulvovaginal swabs for NG, CT and TV; and pharyngeal and anorectal swabs for NG and CT.33–35 Rapid dual tests for HIV/syphilis have been developed and evaluated, but only one so far has been prequalified by the WHO, though others are in the process.36 37
Research question and inclusion criteria
The review addressed the following research question: should self-collection of samples be offered as an additional approach to deliver STI testing services?
Population
Individuals using STI testing services.
Intervention
STI testing services that incorporate self-collection of samples.
Comparison
STI testing services that do not incorporate self-collection of samples (ie, clinician-collection) or no STI testing services (ie, syndromic management alone or no lab-based intervention).
Outcomes
Primary:
Uptake of STI testing services (eg, the proportion who accepted and completed the test).
Frequency of STI testing.
Social harms or adverse events (eg, device-related issues, coercion, violence, psychosocial harm, self-harm, suicide, stigma, discrimination and frequency of HIV testing) and whether these harms were corrected or had redress available.
Secondary:
Proportion of people who tested positive for an STI (case finding).
Linkage to clinical assessment or STI treatment following a positive test result.
Reported sexual risk behaviour (eg, condom use, condomless sex, unprotected sex, number of sexual partners).
To be included in the review, an article had to meet the following criteria:
Study design comparing people who self-collected samples to people who had samples collected by a clinician for STI testing or to those who received no STI testing services.
Evaluated one or more of the outcomes listed above.
Published in a peer-reviewed journal.
Because this study was designed to inform WHO guidelines on the viability of self-sampling as an additional means to increase testing, articles that compared self-collection of samples by the location of intervention delivery (ie, self-collection at home vs self-collection at the clinic) were not included. These articles have been reviewed elsewhere.19 26–31
A full review protocol is available on PROSPERO (CRD42018114871).
Search strategy and screening process
We searched PubMed, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Latin American and Caribbean Health Sciences Literature (LILACS) and Embase through the search date of 18 July 2018, with no limits on publication year, study location or language. We also conducted secondary reference searching on all studies included in the review and three relevant systematic reviews.19 28 31 Selected experts in the field were contacted to identify additional articles not identified through other search methods. We searched for ongoing randomised controlled trials (RCTs) on clinicaltrials.gov, the WHO International Clinical Trials Registry Platform, Pan African Clinical Trial Registry and the Australian New Zealand Clinical Trials Registry. Search terms were developed for STIs and self-sampling; the full search strategy for is available in online supplementary file 1.
Supplemental material
After initial screening of titles, abstracts, citation information and descriptor terms, records were screened independently and in duplicate by two reviewers, with differences resolved through consensus. Full-text articles were obtained of all selected records. Three reviewers independently assessed all full-text articles for eligibility to determine final study selection. Differences were resolved through consensus.
Data extraction and management
For each study, the following information was compiled via independent double-data extraction: study citation, objectives, location, population characteristics, description of the type of STI sampling, description of any additional intervention components, sample size, follow-up periods and loss to follow-up, analytic approach, reported numerical outcomes, results and limitations.
Methodological components of the studies were assessed and classified as high or low risk of bias. For RCTs, risk of bias was assessed using the Cochrane Collaboration’s tool for assessing risk of bias.38 For comparative studies that were not RCTs, study rigour was assessed using the Evidence Project risk of bias tool for intervention evaluations.39
Data analysis
Data were analysed according to coding categories and outcomes. Where multiple studies reported the same outcome, we conducted meta-analysis using random effects models to generate pooled estimates of relative risk (RR) using the programme Comprehensive Meta-Analysis.40 Heterogeneity was assessed using both Q and I-squared statistics. Data from RCTs and observational studies were analysed separately. For the case finding outcome for the RCTs, we ran sensitivity analyses to explore differential effects between self-collection and clinician-collection by using as a denominator (1) all study participants enrolled and randomised to study arms regardless of testing uptake (true intention-to-treat) and (2) only participants who collected samples for STI testing services (subgroup of respondents only).
Patient and public involvement
Patients and the public are currently involved in a global survey of values and preferences and in focus group discussions with vulnerable communities conducted to inform the WHO self-care guidelines and thus play a significant role in the overall recommendation outcome from this review.
Results
Online database searching retrieved 1207 records and secondary searching 4 records; there were 681 unique citations after removing duplicates (figure 1). After initial screening of titles and abstracts, 286 citations remained for double-screening and 184 underwent full-text review. Total 173 articles were excluded after full-text review, 14 of which were excluded because they compared self-sampling delivery approaches (ie, self-sampling at home vs self-sampling in the clinic) rather than self-sampling vs a non-self-collected sampling approach. A total of 11 studies reported in 11 articles met the criteria for inclusion in the review,41–51 10 of which were included in meta-analyses.41–46 48–51

PRISMA flowchart of the study selection process.
Study characteristics
All included studies—with 202 745 participants total—were conducted in high-income countries, with six in the USA,41 43–46 51 three in Denmark48–50 and two in Australia.42 47 Years of publication ranged from 199848 50 to 2018.45 Three studies focused on NG and CT,41 43 45 two studies on NG, CT and TV42 46 and five studies on CT exclusively.44 48–51 One study did not report which specific bacterial STIs were covered.47 No studies compared findings for syphilis. Studies varied in location of self-collection (ie, clinic-based41 45 47 vs home-based42–44 46 48–51) as well as target population (ie, general population,44 51 MSM,41 47 people living with HIV,41 47 adolescents and young people,43–47 50 51 detainees,46 people who inject drugs,42 47 sex workers47 and partners of CT-positive patients48 49). Sample self-collection methods included first-void urine,42 45 48–50 vaginal flush using saline49 50 and pharyngeal,41 rectal,41 47 urethral41 and vaginal42–47 51 swabs. Table 1 presents descriptions of the included studies, and table 2 details their reported outcomes.
Description of included studies
Reported outcomes
Five included studies were RCTs,43 48–51 and the remaining six were observational studies (four serial cross-sectional41 42 45 47 and two cross-sectional44 46). Risk of bias was deemed moderate in the RCTs. Regarding selection bias, one RCT randomly assigned participants ‘according to date of birth’48 and two did not specify the method of random sequence generation.49 50 Due to the nature of the intervention, blinding was impossible and may have biased performance; four RCTs did not report whether the laboratory personnel conducting the STI testing were blinded.48–51 The observational studies were judged to have high risk of bias. Four studies used serial cross-sectional surveys to compare before and after implementation of an intervention package which included self-collection of samples for STI testing.41 42 45 47 None of the observational studies clearly controlled for confounders, though some stratified analyses by gender45 or by clinic type.47Table 3 presents an assessment of study rigour.
Quality assessment of included studies
For each of the main outcomes, results are presented below and summarised in table 4.
Summary of effect sizes and meta-analyses
Uptake of STI testing services
All five RCTs43 48–51 and three observational studies41 45 47 reported some measure of uptake of STI testing services. Substantial heterogeneity was present in all meta-analyses of STI testing uptake.
Meta-analysis of the five RCTs found that participants were three times as likely to get tested for any STI when using self-collection of samples compared with clinician-collection (RR: 2.941, 95% CI 1.188 to 7.281, I-squared: 98.942) (figure 2).43 48–51 Three of these RCTs took place in Denmark48–50 and two in the USA;43 51 two focused on partner screening,48 49 two on young people43 50 and one on rescreening.51 Self-collected sampling methods evaluated by these RCTs included urine,48–50 vaginal flush49 50 and vaginal swab;43 51 participants returned the self-collected specimen(s) for laboratory testing by mail, using a postage-paid, preaddressed envelope or carton.

Meta-analysis of RCTs: uptake of STI testing services for any STI. RCTs, randomised controlled trials; STI, sexually transmitted infection.
When stratifying to RCTs testing solely for CT, meta-analysis of four studies found an even greater impact on STI testing uptake (RR: 3.567, 95% CI 1.096 to 11.608, I-squared: 98.982).48–51 When stratifying to RCTs testing for multiple STIs, only one was identified: this RCT among young women in the USA found increased uptake with self-collection of samples for CT and NG testing (RR: 1.370, 95% CI 1.190 to 1.580).43
We also conducted meta-analysis stratified by gender (figure 3). Among male participants, we found a strong association between self-collection of samples and STI testing uptake (RR: 6.900, 95% CI 1.721 to 27.656, I-squared: 96.784).48–50 Among female participants, the RR was lower but still strong (RR: 3.292, 95% CI 1.072 to 10.115, I-squared: 98.946).43 49–51
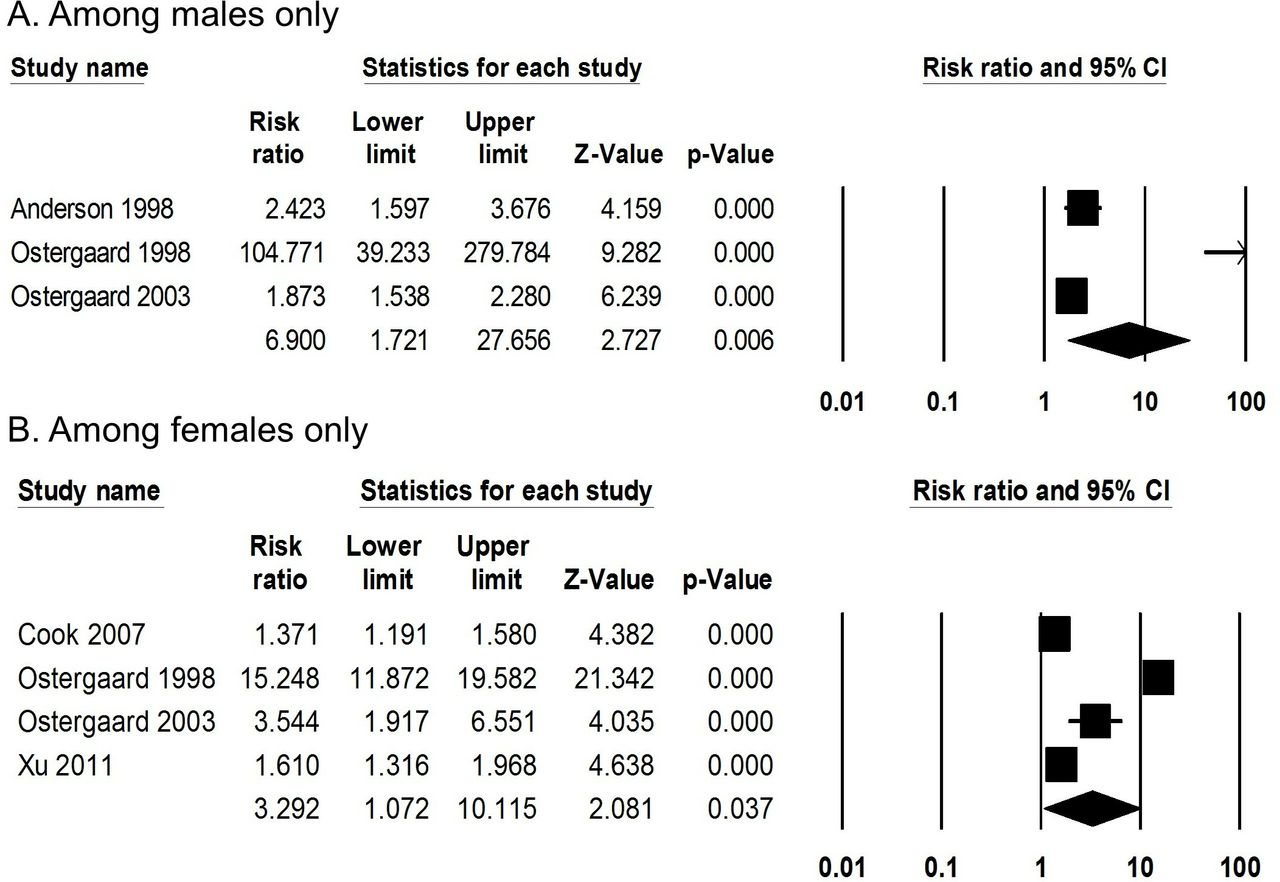
Meta-analysis of RCTs: uptake of STI testing services for any STI, stratified by gender. RCTs, randomised controlled trials; STI, sexually transmitted infection.
The observational studies showed similar findings. Meta-analysis of two observational studies testing for multiple STIs (CT and NG,41 and NG and TV42) found a RR of 2.990, but this was not statistically significant (95% CI 0.426 to 20.978, I-squared: 95.333). When examining the uptake of CT testing specifically, one study found a positive association with self-collection (RR: 2.351, 95% CI 1.597 to 3.462).42 A third observational study could not be combined in meta-analysis but found that after implementing an express clinic with self-collection of genital and rectal samples within a large sexual health clinic, 5335 patients were seen (combining both the express and main clinics) compared with 4804 patients seen through the prior routine STI triage and testing services.47
Case finding
Four RCTs48–51 and five observational studies41 42 44–46 reported comparisons of STI test positivity rate comparing participants who self-collected samples to those whose samples were collected by a clinician.
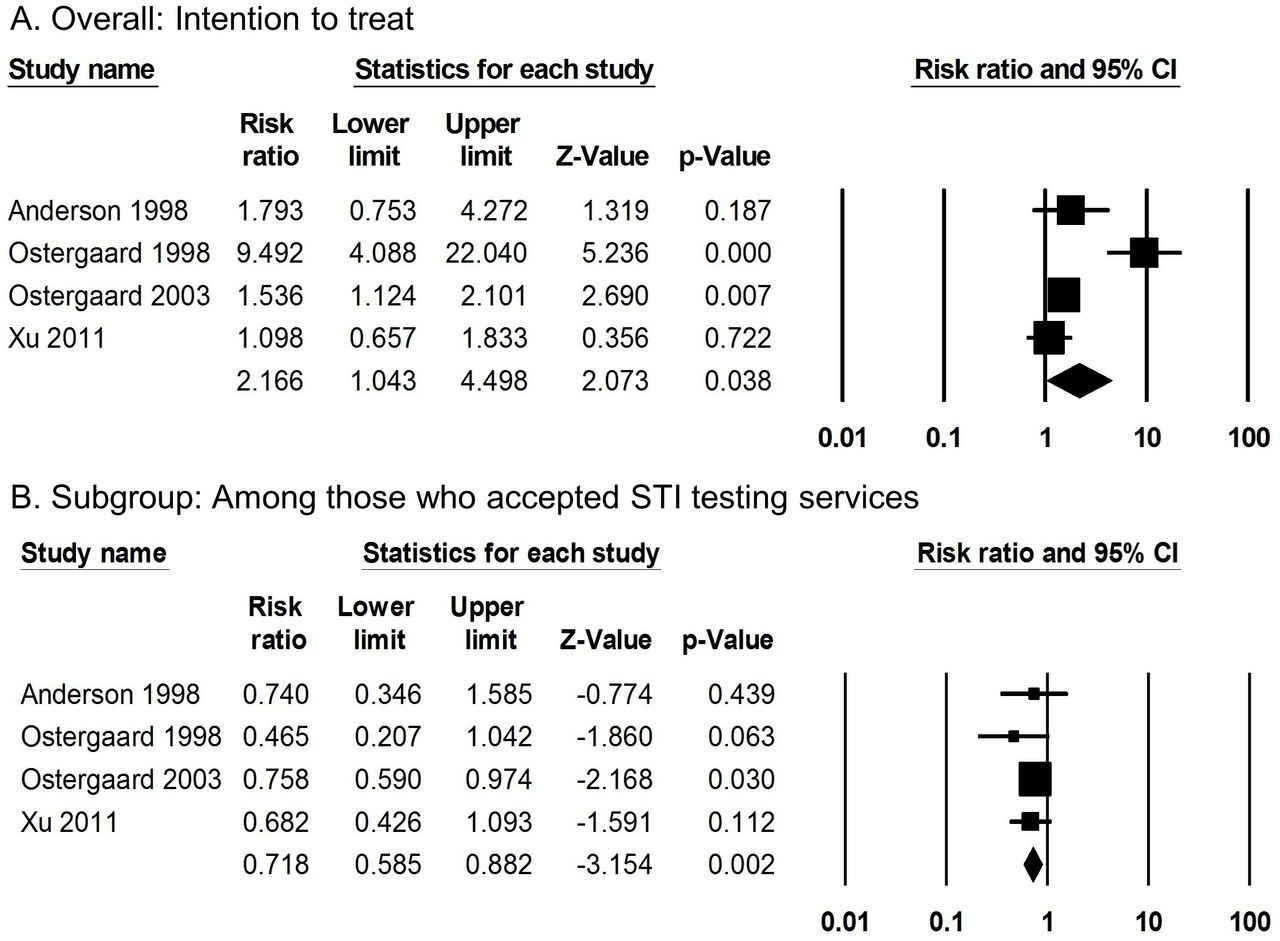
Meta-analysis of RCTs for case finding found effects in opposite directions, depending on which sensitivity analysis was used (figure 4). When the denominator was all study participants who were enrolled and randomly allocated to self-collection or clinician-collection (intention-to-treat), meta-analysis of the four RCTs measuring the proportion of people who tested positive for any STI found double the likelihood of receiving a positive test result among those who self-collected samples for STI testing, with significant heterogeneity (RR: 2.166, 95% CI 1.043 to 4.498, I-squared: 84.387).48–51 However, when comparing self-collection to clinician-collection among only those who ultimately provided samples for STI testing, the association between proportion of positive tests and self-collection went in the opposite direction (RR: 0.718, 95% CI 0.585 to 0.882, I-squared: 0.000).48–51 These four RCTs measured CT only.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of RCTs: case finding for any STI. RCTs, randomised controlled trials; STI, sexually transmitted infection.
The observational studies generally showed no difference in case finding between self-collection and clinician-collection groups, whether meta-analyses were performed using a denominator of the entire study population or a subgroup of only those who took up STI testing services, and regardless of which specific STI or combination of STIs were getting tested.41 42 44–46
Other outcomes
No studies compared the impact of self-collection of samples to clinician-collection of samples on the following outcomes: frequency of STI testing, social harms or adverse events, linkage to clinical assessment or STI treatment following a positive test result and reported sexual behaviour.
Discussion
Despite a limited evidence base and considerable heterogeneity in meta-analyses, the existing literature suggests that using self-collection of samples for STI testing increases uptake of STI testing services, whether for testing of any STI, a combination of multiple STIs or CT alone. Meta-analysis also showed that self-collection of samples had a greater impact on uptake among men than women, though it was positively associated with uptake among both. Meta-analysis also found increased case finding with self-collection of samples when examined among all participants, though it decreased among those who self-collected samples if analysing only those who accepted STI testing services. The evidence base generally supports self-collection of samples as an additional approach to deliver STI testing services.
We identified only a small number of articles that met the inclusion criteria, limiting the evidence base from which we could draw conclusions. Included studies presented comparative data for CT, NG and TV, but not for syphilis. This is not surprising, given the early stage of developing rapid tests for syphilis and the difficulty of collecting whole blood. The number and type of outcomes were also limited; no studies compared the effect of self-collection of samples to clinician-collection on frequency of STI testing, adverse events, linkage to care or sexual risk behaviour. The included studies varied in their target populations, delivery strategies and STIs of interest, making cross-study comparisons difficult. Finally, no studies were conducted in LMICs. STIs are a global epidemic, and more data are needed on self-collection of samples for STI testing in resource-limited settings.
Strengths of this review include the inclusion of both randomised and non-randomised studies and inclusion of studies in any location or language. While we searched multiple online databases and used several additional approaches to identify relevant articles, it is always possible that our search strategy missed some articles. We also relied on peer-reviewed journal articles, which while ensuring a minimal level of quality, may also be subject to publication bias.
This review expands on previous reviews, which have assessed accuracy, feasibility and acceptability of self-collection of samples for STI testing and have compared sample (self-) collection in clinical and non-clinical settings.19 28 31 Our findings that self-collection of samples is associated with increased uptake of testing are comparable with other reviews, which found that home-based sampling is associated with greater uptake compared with clinic-based sampling.19 28 31 Together, these reviews and ours generally support the idea of self-collection as an approach to facilitate STI testing uptake among diverse populations.
Similar to a Cochrane review of home-based versus clinic-based sample collection for chlamydia and gonorrhoea testing,28 we found that, among participants who collected samples for STI testing, self-collection of samples was associated with a lower proportion of positive results, though when we expanded the denominator to all enrolled and randomised study participants, case finding increased among self-collectors. It is possible that people who perceived themselves as having lower risk of STIs were more willing to test for STIs when given the option to self-collect samples than if they were asked to come to a clinic for a provider to collect samples for STI testing. Conversely, individuals experiencing symptoms or who believed themselves at higher risk of STIs might have had additional motivation to use clinic-based STI testing services, possibly due to the care and support offered by a conventional STI clinic or the perceived accuracy and trust of a clinician-performed exam. A systematic review of patients' values and preferences around sample self-collection suggests that accuracy and trust in test results is a concern in some populations.21 Thus, for programmatic purposes, self-collection of samples may both increase STI testing uptake and the number of positive diagnoses, though the proportion of case finding among those who actually self-collected samples for STI testing may be comparatively less than those who had samples collected by a clinician.
The STI burden in many countries has not been adequately addressed, particularly in the face of institutional and funding capacities focused on prevention and treatment of HIV.52 53 Self-collection of samples for STI testing—already the standard in most high-income settings and well-accepted by a variety of end-users and providers—has the potential to increase uptake of testing services, thus reaching individuals at higher risk of STIs, in particular, those who may be unwilling to provide samples in the traditional manner by healthcare providers.18 If both uptake and case finding increase, expansion of STI services through sample self-collection may be cost-effective, though more research on this is warranted. Several studies have suggested that internet-based screening or other models using self-collection of samples for STI testing may be cost-effective compared with clinician-collected samples.27 54 Self-collection as an additional approach to STI testing and diagnosis supports the WHO global health sector strategy on STIs, which emphasises the need for identifying targeted accessible interventions, which ensure that people use the quality health services they need without suffering financial hardship or stigmatisation.53 Promoting self-collection of samples as an additional approach for STI testing service delivery could contribute to the achievement of the United Nations Sustainable Development Goals, including universal health coverage and integrated services for sexual and reproductive health, which requires achieving early diagnosis of STIs and linkage to effective treatment.55
Acknowledgments
We thank Laura Ferguson, Gina Ogilvie and Nandi Siegfried for their thoughtful comments on the systematic review protocol. We also thank Poonam Gupta and Eric Rodriguez for their assistance in extracting data.
References
Footnotes
YO and PTY contributed equally.
Handling editor Seye Abimbola
Contributors MN conceptualised the study. CEK and PTY designed the protocol. CEK conducted the search. YPO and PTY conducted screening, data extraction and assessment of bias and quality of reporting. YPO and PTY drafted the manuscript. YPO, PTY, CEK, IT and MN reviewed the draft, provided critical review and read and approved the final manuscript. The corresponding author, as guarantor, accepts full responsibility for the finished article, has access to any data and controlled the decision to publish. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding We gratefully acknowledge financial support of the UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) and the Children's Investment Fund Foundation (CIFF). HRP was involved in the study design.
Disclaimer The funders played no part in the decision to submit the article for publication nor in the collection, analysis and interpretation of data. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extracted data are available on request to the corresponding author.