Article Text

Abstract
Objective: To describe the epidemiology and estimate the health resource use of patients with viral hepatitis in Tayside, Scotland, using record linkage techniques.
Design: A retrospective observational study.
Setting: Liver disease database, Tayside, Scotland.
Patients: All subjects resident in Tayside in the study period 1989–1999 and registered on the Epidemiology of Liver Disease in Tayside (ELDIT) database.
Main outcome measures: Incidence and prevalence of known viral hepatitis in Tayside, survival of subjects diagnosed with viral hepatitis, and the health resource use with respect to hospital admissions compared with the general population.
Results: There were 4992 patients identified with viral hepatitis in the study period 1989–1999; 86 were IgM positive anti-hepatitis A, 187 patients were hepatitis B surface antigen (HBsAg) positive, and 469 were anti-hepatitis C (HCV) positive. HCV and HBsAg seropositive patients were more likely to be hospitalised and stay in hospital longer, less likely to survive after six years, and used more drugs of potential abuse than the general population. There was an increase in cost per admission and per patient as a consequence of liver disease.
Conclusions: A record linkage population based study of viral hepatitis allows outcomes to be identified and costed. Those at risk of viral hepatitis infection in the Tayside population should be informed about the future implication to their health and costs to society. The health service should investigate the cost effectiveness of vaccination and opportunity costs to the health service of viral hepatitis taking into consideration the increasing incidence and prevalence of disease.
- epidemiology
- viral hepatitis
- observational study
- health resource use
- ELDIT database, Epidemiology of Liver Disease in Tayside database
- MEMO, Medicines Monitoring Unit
- HAV, HBV, HCV, hepatitis A, B, C virus, respectively
- HBsAg, hepatitis B surface antigen
Statistics from Altmetric.com
- ELDIT database, Epidemiology of Liver Disease in Tayside database
- MEMO, Medicines Monitoring Unit
- HAV, HBV, HCV, hepatitis A, B, C virus, respectively
- HBsAg, hepatitis B surface antigen
Many viral hepatitis studies are based on specially constructed cohorts,1–3 cross sectional surveys of populations,4–6 or outcomes of medical interventions.7 However, there are few population based observational studies of viral hepatitis that are large enough to determine the incidence and prevalence of disease. Cross sectional studies have primarily been used to estimate prevalence of disease but this study design may suffer from selection and recall bias. True ascertainment of viral hepatitis in a population is crucial to adequately identify research needs and assess health resource implications.
This paper describes the epidemiology and health service utilisation of subjects with viral hepatitis in the Tayside population and a general population comparator cohort.
METHODS
Epidemiology of Liver Disease in Tayside (ELDIT) database
We used the ELDIT database of liver disease created by record linkage of primary and secondary health care data. In Tayside (estimated mid-year resident population of 389 800 in 19988), every patient who is registered with a general practitioner is allocated a unique 10 digit identifier called the community health number that is centrally held and continuously updated. The community health number is used as the patient identifier in all healthcare activities in Tayside, in both primary and secondary care. After patient anonymisation, we record linked the following independent data sources to maximise patient specific data available for the study:
-
Virology database. Computerised patient specific records exist for all requests for viral serology from primary and secondary care for the hepatitis viruses for the Tayside region since 1980. The ELISA test was used in the regional viral laboratory to identify viral hepatitis.
-
Prescribing database. The Medicines Monitoring Unit (MEMO) has captured person specific dispensing information for the whole of Tayside since January 1993 and has been described elsewhere.9
-
Scottish morbidity records. This is a list of hospital discharges for all hospitals in Scotland. Type of hospital admission for viral hepatitis subjects and their comparator groups were obtained from this data set. Duration of stay was calculated using admission and discharge dates.
-
Death registry. Details of all deaths in Tayside since 1989 are electronically recorded through a copy of the General Registers Office-Death Certification Database and held within MEMO.
-
Carstairs social deprivation categories. These range from category 1 (most affluent) to category 7 (least affluent) and are based on four census variables (household overcrowding, ownership of a car, number of people in semi- or unskilled occupations, and male unemployment rate). The deprivation category is determined from the patient's postcode.10
After record linkage of the data sets, a complete outcomes data set of subjects with viral hepatitis patients was incorporated into the larger ELDIT database of other liver diseases found in a similar manner. The ELDIT database was used for liver disease comparisons and stored all data for further research.
Study population
This study was carried out on residents of Tayside, Scotland, during the study period 1989–1999. Patients with viral hepatitis were identified from the virology data set from Ninewells Hospital. The virology department performs all viral hepatitis serology in the Tayside region. Requests for viral hepatitis tests were from general practice (primary care), the hospital (general admissions and specialist clinics), and institutional services (for example, prison service). Subjects living outside the Tayside region were excluded from the study.
Comparator group
To compare and evaluate the health resource use, costs, and demographics of viral hepatitis patients, a comparator group was randomly selected from the Tayside population. The selection of the comparator group used a base population from Tayside that were alive and registered with a general practitioner. Subjects in the base population were not allowed to move out of the Tayside area but were allowed to die. This is to ensure that all healthcare activities in Tayside for the base population can be identified with little or no loss to follow up of subjects. The subjects with viral hepatitis were taken out of the base population. A program written in SAS, version 8 (Cary, North Carolina, USA) allocated a random number to each subject in the base population and then sorted by the random number to ensure a completely unbiased selection of the comparator group. Two comparators were age-sex frequency matched (by five year age bands) for each viral hepatitis patient. Random selection ensures the comparators were not the same people in each viral hepatitis disease group giving an unbiased representation of an age-sex matched general population for comparison.
Cost analysis
The cost of hospitalisation for viral hepatitis patients and comparator groups were calculated using 1997 costs, obtained from the Scottish Health Service Costs.11 The direct medical costs for hospitalised patients included hospital charges to house the patient in the hospital per day, laboratory testing, physician's fees, diagnostic procedures, and outpatient follow up. The perspective of the cost analysis was from that of the NHS hospital. The median costs of hospitalisation were compared using Wilcoxon sum rank tests of significance.
Statistical analysis
Differences between the viral hepatitis population and their general population controls were analysed using the χ2 statistic. Yearly incidence and prevalence rates were based on the number of Tayside residents with newly diagnosed viral hepatitis in the year. In calculating these rates, the entire population of Tayside for the year was considered to be at risk. The denominator was estimated from the master patient index of the Tayside Health Board of all patients registered with a general practitioner. Kaplan-Meier curves were used to illustrate the survival of hepatitis patients from the incident date of positive sample to death of the subject. The relative hazard functions of survival of viral hepatitis patients were calculated using the proportional hazards model. Statistics were performed using SAS, version 8 (Cary, North Carolina, USA).
RESULTS
Among the Tayside residents there were 4992 patients identified with viral hepatitis during the study period 1989–1999. Of these, 4090 patients were anti-hepatitis A (HAV) positive, only 86 were IgM positive indicating acute infection, 469 patients were anti-hepatitis C (HCV) positive, and 433 patients had hepatitis B (HBV). Of the HBV (HBV core antibody IgG positive) patients, 187 were identified as hepatitis B surface antigen (HBsAg) positive and were analysed separately. The descriptive analyses of the patients are given in table 1. Age of the patients differed with type of infection. HAV patients were older while HBV and HCV patients were younger than the general population. HAV patients were evenly distributed throughout the social deprivation categories but HBV and HCV patients were living in less affluent areas. HBV and HCV patients were generally male while HAV patients had a similar distribution to the general population. Table 2 shows the cross infection frequency of viral hepatitis patients in the study.
Descriptive characteristics of the viral hepatitis cohorts
Frequency of cross infection with other viral hepatitis infections
The incidence and prevalence of known viral hepatitis are given in table 3. While the incidence of viral hepatitis increased slowly over the study period, the prevalence of known HCV disease increased rapidly. This may be an artefact of the data because the HCV diagnostic test was not available until the late 1980s. Thus the rapid increase in the number of existing cases was because the identifying test was becoming more widely available over time. Therefore, the slope of HCV prevalence is not an indication of the true prevalence of disease (that is, starting with 0 disease in the population), but rather the prevalence of known disease in the population.
Incidence and prevalence of known viral hepatitis per 100 000 population by year
General population comparison
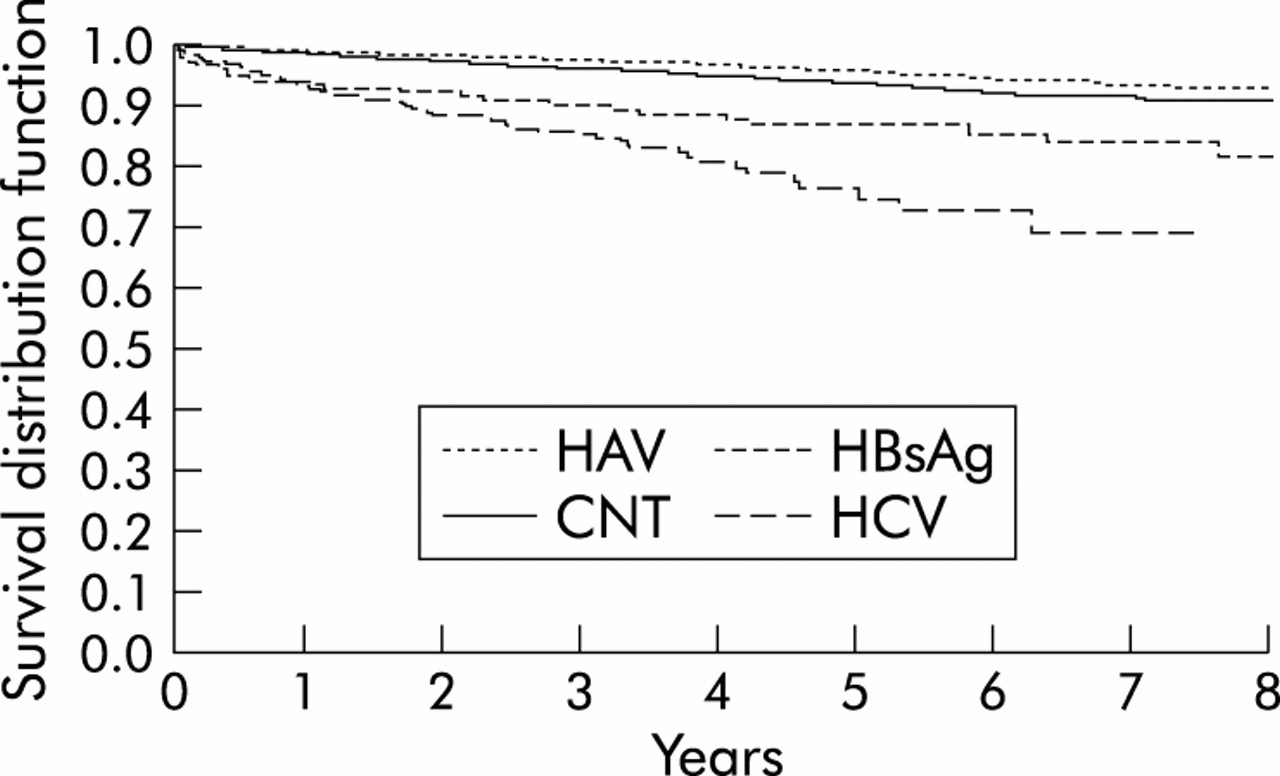
The comparative study found that HAV patients were very similar to the general population and in the case of survival, significantly better than the comparator cohort. It was hypothesised that HAV subjects had a “healthier” lifestyle, were more affluent (as seen in table 1), and were exposed to the HAV virus through travel in endemic areas. From the MEMO database of prescribed medication, 2231 subjects per year were prescribed HAV vaccinations in Tayside. Some of this group may represent prevaccination investigations but it is the policy in Tayside not to test for HAV status after vaccination. Further research into this group of subjects to identify the risks and determinants of HAV infection is needed. The HCV and HBsAg positive patients, however, were very different from the comparators. The relative hazards, as calculated by the proportional hazard model, are given in table 4. This analysis gives the odds of survival for patients with viral hepatitis compared with the general population. HCV patients were 8.03 times more likely to die at the end of seven years compared with the general population comparators. HBsAg positive patients were 2.84 times more likely to die following diagnosis after 10 years compared with the general population. This is illustrated graphically in survival after diagnosis in the Kaplan-Meier curve in fig 1. Initially, the proportion of survivors decreases rapidly for HCV and HBsAg positive patients and continues to gradually decrease in proportion with time. The underlying cause of death for HCV patients was analysed and it was found that 29 of the 69 deaths were associated with some form of drug misuse (table 5). For example, 17 patients with HCV died of an underlying cause of human immunodeficiency virus or acquired immunodeficiency syndrome and 12 with substance dependencies. Eleven of the 69 deaths in HCV positive patients were associated with liver disease (liver cancer, three; liver disease, three; viral hepatitis, five), whereas five of the 12 deaths in HBsAg positive patients were associated with liver diseases (liver cancer, three; liver disease, one; viral hepatitis, one). The majority of other underlying causes of death in both groups was cancer other than liver cancer (three in each group) and cardiovascular and respiratory disease (HCV, 11; HBsAg, 1).
Results of the unadjusted and adjusted proportional hazards model for viral hepatitis from diagnosis to death
Underlying cause of death for hepatitis C and HBsAg positive subjects

{kind=link}
Kaplan-Meier curve of viral hepatitis survival compared with a control (CNT) group. HAV, hepatitis A virus; HCV, hepatitis C virus; HBsAg, hepatitis B surface antigen.
Exposure to drugs of abuse for HCV and HBsAg positive patients was compared with the general population. Table 6 gives the results of exposure to drugs of abuse. Generally, the viral hepatitis patients were more likely to be dispensed drugs with a potential for abuse (temazepam and anxiolytics). However, these drugs were also used in combination with methadone to treat drug abuse, indicating that there may be some drug dependency, especially in HCV patients (dispensed methadone odds ratio 50.5).
Analysis of proportions for exposure comparison of hepatitis C and HBsAg positive subjects with general population controls
Tables 7–9 show the results of hospital admissions and cost analysis for each viral hepatitis group and their comparators. There was an increased cost associated with HCV (table 9) and HBsAg patients (table 8) compared with the general population. Generally, patients with viral hepatitis were more likely to stay in hospital longer and stay in more expensive specialties while in hospital (for example, intensive therapy units). There was a significant difference in duration of stay between patients with viral hepatitis and comparators (near or at p<0.05). The difference in median cost per patient admitted and median cost per patient was significant (p<0.05). The median cost of HCV was £1626 more per admission and £1671 more per patient than the comparator group. HBsAg patient admissions cost £1231 and £584 more per patient than comparators. The costs presented were from the NHS hospital perspective (that is, costs borne by a hospital admission). The HCV outpatient may present a further £10 000 per year to the NHS budget for drug costs alone (α interferon and ribivarin therapy).
Hospitalisation admission analysis of hepatitis A subjects separated into IgG and IgM positive groups with general population controls
Hospitalisation admission analysis of HBsAg and HBcAb positive subjects with general population controls
Hospitalisation admission analysis of hepatitis C subjects with general population controls
DISCUSSION
To the best of our knowledge, this is the first population based study that record links clinical data to identify viral hepatitis subjects from primary and secondary care. We found that the incidence and prevalence of known viral hepatitis rapidly increased over the seven year study period. The hospital costs of treating a HCV patient was £1671 more than the general population comparator cohort, while treating a HBsAg patient cost £584 more.
A study by Termorshuizen and colleagues12 found a prevalence of 33.8% seropositive HAV in a Dutch population tested in a cross sectional study. The result is similar to ours where 37.1% tested seropositive for HAV. This study also agrees with a pattern of increasing HAV seropositivity with increasing age.1,12 Termorshuizen et al suggested that the cohort effect was associated with an increase in HAV seropositivity in the elderly population because the possible time exposed is greater in the older population. Increasing hygiene may also affect transmission of HAV in the younger population. One possible hypothesis for the high number of “well” HAV (IgG) positive patients in this study is that it represents further investigations (battery of tests for hepatitis) for liver dysfunction after initial abnormal liver function tests. Prevaccination testing may also play some part in the high number of HAV positive patients. However, post vaccination testing cannot account for the high positive rate because it is a policy in Tayside not to test after HAV vaccination. Further research into investigation results after abnormal liver function tests is needed.
The majority of HCV and HBsAg positive patients were younger males. Exposure to intravenous drug use is a possible transmission route for HCV and was significantly associated with HCV infection in this study. The prevalence of disease is similar to published studies. NHANES II found a HBV prevalence of 4.2% and HBsAg prevalence of 0.3% which is similar to the prevalence rates of those tested in our study.13 The prevalence of HCV positive tests among those tested for HCV was higher than the estimated world prevalence of approximately 1.5%—this represents testing of high risk groups, such as patients that are drug dependent which is a major risk factor for HCV infection.14
HBsAg positive and HCV patient survival after diagnosis was significantly different from the general population. The risk of death after diagnosis with HBsAg and HCV shows the clinical burden of disease. The economic burden of viral hepatitis is shown in the increased cost per admission and per patient, which is significantly more than the general population. This disease has become a major public health issue—its prevalence will continue to rise as testing becomes more wide spread. However, it is vital that the projections of need for health service resources are based on the correct numerator and take into account the high death rate of these patients, as this will impact on the number of patients who progress to the most costly complications of disease. This is illustrated by the rates of diagnosed cases used in the recent Scottish Needs Assessment Programme (SNAP) report on HCV.15 The rate of diagnosed cases for Tayside was 177.62 per 100 000 people in 1998, based on acquired virology laboratory data. This is larger than the HCV prevalence in this study of 103.64 per 100 000. However, the SNAP report does not account for deaths in the HCV cohort, the prison population, or anonymous testing by the laboratory (which may lead to duplicate reporting). Careful consideration and patient specific data analysis will reveal the true prevalence of disease and target populations.
There are limitations to every study design. In this study the majority of viral hepatitis cases were diagnosed by clinical suspicion of underlying disease and this is likely to underestimate the total number of viral hepatitis infections in our population as there may be subclinical or asymptomatic infection. Patients symptomatic of liver disease and those entering the health care field are tested for viral hepatitis only if clinically indicated. It is policy in Tayside not to routinely screen patients for viral hepatitis unless they are in the “drug problem service” or prison. None the less, more than one data set was used to identify patients so that ascertainment of those with true and/or possible disease was maximised. The prevalence of known viral disease compares well with other published studies suggesting that our method of identifying patients is comparable with other study designs.
CONCLUSION
In conclusion, the epidemiology of viral hepatitis from a population base should aid in prioritising preventive measures by identifying the at-risk populations. This will allow for the most appropriate use of available resources. Accordingly, the appropriate precautions can be implemented to decrease the prevalence of this emerging infection.
Acknowledgments
ELDIT study group would like to acknowledge the British Liver trust for funding the project and the computer programmers at MEMO for their assistance in formatting the data for the study. MEMO is part of the MRC Health Services Research Collaboration. We thank the Tayside Health Board and ISD (Scotland) for ongoing collaboration.