Article Text

Abstract
Objectives In the Netherlands, sexually transmitted infection (STI) care is provided by general practitioners (GPs) as well as by specialised STI centres. Consultations at the STI centres are monitored extensively, but data from the general practice are limited. This study aimed to examine STI consultations in the general practice.
Design Prospective observational patient survey.
Setting General practices within the nationally representative Dutch Sentinel GP network (n=125 000 patient population), 2008–2011.
Outcome measures GPs were asked to fill out a questionnaire at each STI consultation addressing demographics, sexual behaviour and laboratory test results. Patient population, testing practices and test positivity are reported.
Participants Patients attending a consultation concerning an STI/HIV-related issue.
Results Overall, 1 in 250 patients/year consulted their GP for STI/HIV-related problems. Consultations were concentrated among young heterosexuals of Dutch origin. Laboratory testing was requested for 83.3% of consultations. Overall consult positivity was 33.4%, highest for chlamydia (14.7%), condylomata (8.7%) and herpes (6.4%). 32 of 706 positive patients (4.5%) were diagnosed with multiple infections. Main high-risk groups were patients who were <25 years old (for chlamydia), >25 years old (syphilis), men who have sex with men (MSM; for gonorrhoea/syphilis/HIV) or having symptoms (for any STI). Adherence to guideline-recommendations to test for multiple STI among high-risk groups varied from 15% to 75%.
Conclusions This study found that characteristics of patients who consulted a GP for STIs were comparable to those of patients attending STI centres regarding age and ethnicity; however, consultations of high-risk groups like MSM and (clients of) commercial sex workers were reported less by the general practice. Where the STI centres routinely test all patients for chlamydia/syphilis/HIV/gonorrhoea, GPs tested more selectively, even more restricted than advised by GP guidelines. Test positivity was, therefore, higher in general practice, although it is unknown how many STIs are missed (particularly among high-risk groups). Opportunities for a more proactive role in STI/HIV testing at general practices in line with current guidelines should be explored.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Large study population (2111 questionnaires were filled in).
-
Data were available on several demographic and behavioural risk factors; usually these data are difficult to retrieve from the general practice.
-
Not all laboratory results were available.
-
The high STI test positivity found may indicate selection bias.
Introduction
In the Netherlands, treatment of sexually transmitted infections (STIs) and care is mainly provided by general practitioners (GPs) and specialised STI centres. GPs play a central role as ‘gatekeeper’ to secondary healthcare; costs of general practice consultations are covered by the national health insurance. In addition, STI centres provide publicly funded STI care for specific high-risk groups.
Case-based data on STI diagnoses and characteristics of clients are collected in an online, real-time database from the STI centres for the purpose of national surveillance of STI and HIV. Insight into STI consultations in general practice is limited to reporting rates from sentinel surveillance based on electronic medical registration by International Classification of Primary Care (ICPC) codes. These data lack information on diagnostic tests performed and patient characteristics of those tested.1 ,2 Since an estimated 70% of all STI/HIV consultations take place at the general practice in the Netherlands,1 ,3 more detailed data on STI consultations in primary care are required to gain a more comprehensive overview of the STI epidemiology and testing behaviour in the country, necessary for surveillance and control.
Specific guidelines for STI consultations exist for GPs4 indicating which high-risk groups should be tested. Young (<25 years old) heterosexuals should be tested for gonorrhoea (when reporting discharge) and chlamydia, with further testing for syphilis, hepatitis B and HIV for those with casual contacts. Men who have sex with men (MSM), commercial sex workers (CSWs) and clients of CSWs and patients who originate from HIV endemic countries or have a partner with this ethnic background should be tested for all five STI. These STI guidelines are available online5 and enforced through continuing education and elearning for GPs.6
The number of STI consultations and positive tests among high-risk groups at STI centres has gradually increased in recent years.7 Chlamydia is the most diagnosed STI with 11.5% positive tests in 2011, slightly increasing over the past years, with heterosexuals <25 years accounting for the highest rates (14.8%). The positivity rates for gonorrhoea were stabilising but increased slightly from 2.7% in 2010 to 3.2% in 2011 (9% in MSM); rates of HIV remained stable at 0.4% (2% in MSM) while infectious syphilis among MSM steadily declined from 3.9% in 2008 to 2% in 2011 (0.4% overall). The percentage diagnosed with genital herpes and genital warts remained stable, around 0.5% and 2.1%, respectively, in 2011.7
It is unknown to what extent trends in STI epidemiology in the high-risk population at STI clinics reflect trends in the whole population; information from the, presumably lower-risk, population seeking care at a general practice may help to improve STI control in the Netherlands and enable comparisons to the situation in other countries.
Therefore, an STI and HIV-related questionnaire was implemented in a national network of GPs, from 2008 onwards. Here we discuss the findings to 2011 and compare outcomes of demographics, test requests and positivity rates with data of the STI centres.
Methods
The nationwide Dutch sentinel GP network, founded in 1970, included 42–45 GP practices in the Netherlands in the period of study and covered a population of about 125 000 patients (0.8% of the total Dutch population) enclosing geographical dispersion and variation in population density.8
In the Dutch sentinel GP network, GPs register disease episodes, comprising of one or more consultations, with ICPC-codes.9 Since 2008, the GPs in the Dutch sentinel GP network are requested to complete a questionnaire for consultations of new episodes concerning STI/HIV issues, registered with ICPC codes for STI diagnoses or ‘fear of STI and/or HIV’, as these are codes registered in case of test-negative STI consultations. The GPs received reminders and instructions for the study annually. A completed questionnaire was recorded in the GP system, to avoid the risk of entering multiple questionnaires per episode. Data were pooled over 4 years (2008–2011), to increase statistical power.
The questionnaire addressed STI testing, diagnoses and background information from the patient with reference to ethnicity, sexual preference and sexual behaviour as well as reasons for STI/HIV consultation. When the GP requested a diagnostic test for chlamydia, gonorrhoea, trichomonas, HIV and/or syphilis (performed by the regional laboratory of the participating practice), an additional laboratory form was requested. For patients for whom no STI diagnosis was reported, no data on any other diagnosis were reported. This survey was implemented within the existing Dutch sentinel GP network surveillance8 and since it was limited to questionnaires (no additional sampling), no medical ethical permission was required; patients in the participating practices are informed about the use of (anonymised) patient data for surveillance and research, and can decline to participate.
Annually, forms were sent from the Dutch sentinel GP network to the National Institute for Public Health and the Environment (RIVM), with anonymous identification numbers. Data were entered in Access, χ2 tests were performed to compare proportions; univariate logistic regression and multivariate analysis were performed to identify determinants for the main outcomes: test request rates and STI positivity rates, using SPSS V.19.0.
Results
During the study period (2008–2011), 2111 questionnaires were filled in by GPs from 43 practices, varying from 1 to 54 questionnaires per practice per year. Annually, on an average, 0.4% (528/138 596) of GP patients (of all ages) were seen for an STI-related consultation; the highest attendance rates were for women (1.6%) and men (0.9%) aged 15–29 years. No obvious trends in attendance rates were visible over the 4 years.
In 83.3% of STI-related consultations, an STI test was requested (table 1). Tests were requested most often for chlamydia and gonorrhoea. For 15.8% of test requests, no laboratory result was available. An STI was diagnosed in 33.4% of consultations (by test or by symptoms, see table 1). In 14.7% of the consultations, chlamydia was confirmed (20.8% test positivity rate). Eight patients were confirmed HIV positive (0.9% of tests). Gonorrhoea, syphilis and trichomonas were reported in 4%, 3.5% and 4.1% of tests, respectively. Herpes accounted for 6.4% and genital warts for 8.7% consult positivity (diagnosed based on presence of symptoms only). For 31 patients, a double infection was reported and for 1 patient, a triple STI infection (4.5% of STI-diagnosed patients) was reported.
Number of test requests and diagnoses per STI in patients consulting the GP for STI-related problems, in the Dutch sentinel GP network, 2008–2011
Outcomes by risk factor and patient group
Age
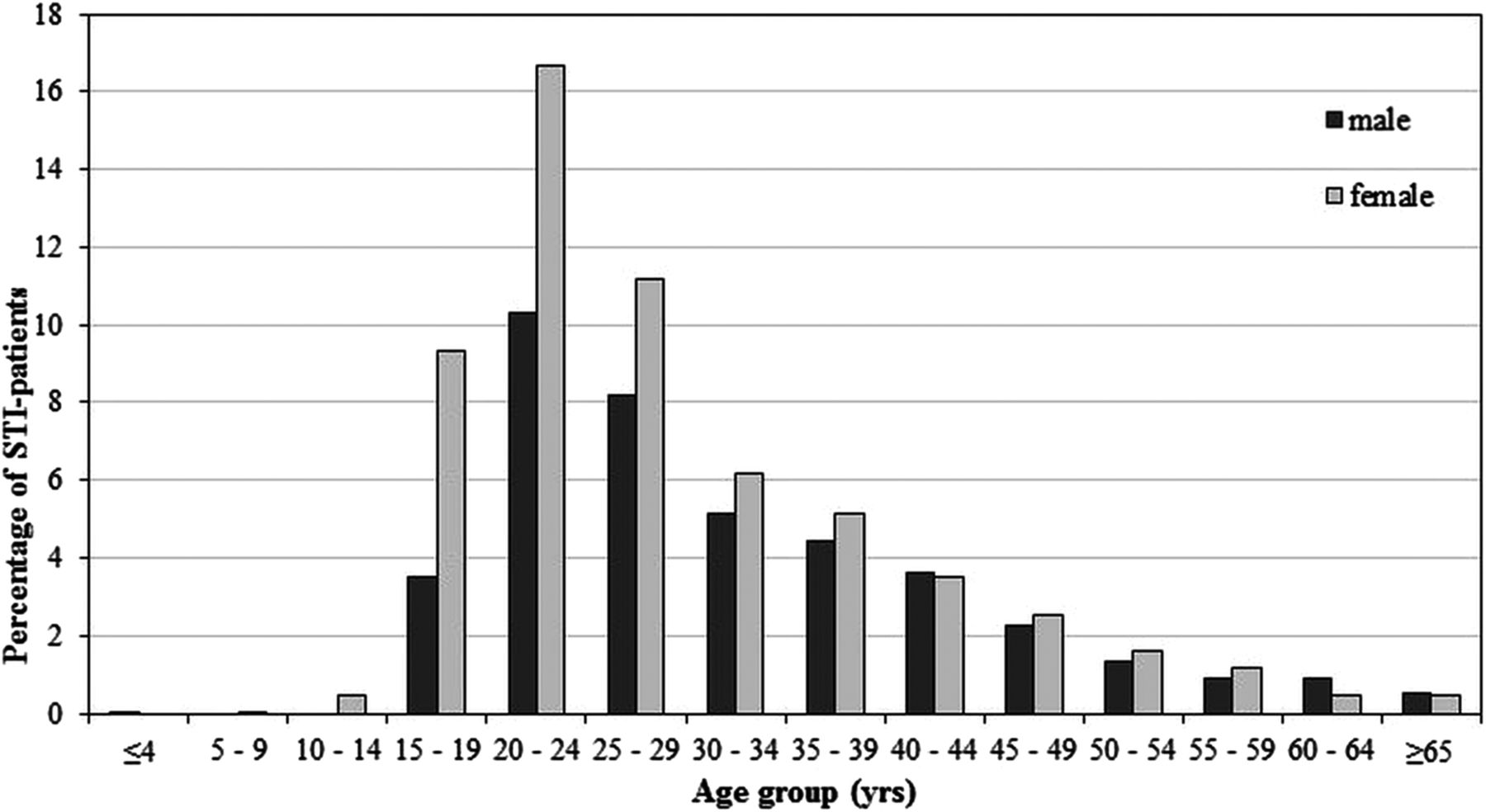
Most frequently, patients were of the age groups 20–24 years (27%) and 25–29 (19%; figure 1). Women were younger than men: 45% of women were under 25 years, compared with 35% of heterosexual men and 24% of MSM. Figure 1 shows the wide age range but clear peak in the 20–24 year age range for patients with STI-related problems; the consultations under 10 years are likely to be reporting artefacts (no details on, eg, sexual abuse were collected). Chlamydia and gonorrhoea tests were requested more frequently for younger patients (<25 years; 82% and 75%) than for older patients (>=25 years; 71% and 65%). HIV, syphilis and hepatitis B tests were less commonly requested in young people (see table 2). Patients >25 years were more often tested for HIV than the younger group (34% vs 28%).
Testing rates by demographic and behavioural risk factor (according to GP guidelines5) seen at STI consultations, in the Dutch sentinel GP network, 2008–2011

{kind=link}
Proportion of male and female patients seen by general practitioners at sexually transmitted infection (STI) consultations by age group in the Dutch sentinel GP network, 2008–2011.
Chlamydia positivity rates were significantly higher in the <25 years age group, while all syphilis infections were found in the older patients (see table 3). Six of the eight patients who tested positive for HIV were in the 25+ age group.
Test positivity for different high-risk groups per STI, in the Dutch sentinel GP network, 2008–2011
Gender and sexual preference
Women accounted for 59% of STI/HIV consultations. The sexual preference of 9.1% of men and 1.5% of women was recorded as homosexual/bisexual, for 4.2% this was unknown and the rest indicated to have heterosexual relations only. Tests for chlamydia and gonorrhoea were more frequently requested for heterosexuals (75.6% and 69.6%, respectively) than for MSM (54.9% and 56.3%). For HIV and syphilis, more tests were requested for MSM (46.5% and 39.4% vs 30.8% and 24.6% in heterosexuals). Women were tested more often for HSV and trichomoniasis than men. Seventeen per cent of MSM was tested for all five STI mentioned in the general practice guidelines. Rectal samples were collected in five MSM patients only (5/40 gonorrhoea tests (12.5%) and 4/39 chlamydia tests (10.3%)).
Table 3 shows that positivity rates for syphilis and gonorrhoea were higher for MSM (33.3% and 25%, respectively, p<0.05) than for heterosexual men (4.4% and 6.3%) and women (0.4% and 1.8%); chlamydia positivity was comparable. Six of eight HIV cases were diagnosed in MSM.
Reasons for consultation
The most common reason to consult the GP was ‘having symptoms’ (43%) followed by routine check-up (19%), recent risk (14%) and partner notification (11%). Fear of/concerns for STI (5%) and risk behaviour by the patient’s partner (4%) were less frequently reported as reason for STI consultation. Patients reporting a recent STI risk for themselves or their partner or indicating a (periodic) STI check-up as their reason to come to the general practice were tested more often (96% and 97.5%, respectively) than those who did not (90% and 81.8%). Reporting of symptoms or partner notification as a reason did not elevate the testing rate (80%), whereas these reasons were related to a higher positivity rate for STIs (see table 3). Patients who reported (periodic) check-up or ‘fear of STI’ as their reason for visit had a significantly lower risk to be diagnosed with chlamydia (8.5% and 6.9%, respectively).
Type of sexual contact
Half of the population indicated to have a steady relationship, one-third had successive casual sexual relationships and 4% reported two or more concurrent sexual partners. In total, 1.2% (2.2% of men and 0.6% of women) reported recent commercial sex contact(s). People reporting casual relationship(s) in the previous 6 months were more often tested for STIs compared with patients with steady relationships. A small part of this risk group was tested for all five STI: 17% of <25 years old with recent casual contacts (table 2). People reporting casual contacts showed a significantly higher positivity rate for gonorrhoea (table 3). Among (clients of) CSWs (n=26), more syphilis, HIV and HBV tests were requested; they were not consistently tested for all five STIs (35%).
Ethnic background
Of the patients, 84% were of Dutch origin, 5% were Surinamese/Antillean and 5% were Turkish/Moroccan. Testing rates were quite similar for Dutch and non-Western ethnic groups and for patients with a partner originating from these countries (table 2). Also, positivity rates were comparable (table 3), except for gonorrhoea, with a significantly higher risk among Surinamese/Antillean patients (OR 5.6). Comparing the reasons for STI consultation between ethnic groups, Turkish/Moroccan patients came less commonly for a check-up than Dutch patients (10.2% vs 20.1%). Homosexual contacts were reported by 9% of Dutch men, compared with 6% of Surinamese/Antillean and 2% of Turkish/Moroccan men.
Discussion
This study observed that GPs in the Dutch sentinel GP network reported an STI consultation for 1 per 250 patients in their practice per year, with higher rates for ages 15–29: 1 in 65 for women and 1 in 110 for men. The GPs requested one or more laboratory tests in the majority of these consultations and diagnosed an STI in about one-third of them. Test requests were quite selective, usually limited to one or two STIs, also for higher risk groups, such as MSM. The implementation of GP guidelines which recommend testing for multiple STIs in specific high-risk groups were poorly adhered to, varying from 15% to 75%, depending on the high-risk group involved. This suggests that GPs might need to engage in less restrictive testing to optimise the efficiency of STI control in primary care.
A limitation of the survey is uncertainty regarding completeness of the data. Owing to lack of time, questionnaires may not have been filled for all STI consultations, and selection bias could have occurred, if STI consultations with a positive diagnosis were more frequently reported. Other bias might have been caused by the fact that not all test results were reported. Finally, since the questionnaire is filled for one consultation, information is lacking on previous or follow-up consultations where GPs may have carried out related examinations or sent the patient for referral, influencing the decision for further testing at the consultation incorporated in the study.
Patients consulting the GP with STI-related issues were mainly young (<25 years old), heterosexual and of Dutch origin and often reported symptoms as the reason for consultation. Known high-risk groups were regularly seen at the general practice for STI consultations. The proportion of MSM among the male study population is comparable with the estimated proportion of MSM in the total Dutch population.10 Compared with the overall Dutch population, where 20.3% belongs to ethnic minorities,11 the proportion of patients from non-Dutch origin is lower (16%), which suggests that this group less frequently consults a GP for STI-related issues. However, in this study self-reported ethnicity was used, which is likely to underestimate the percentages based on the person's and his/her parents’ country of birth.7 ,12
Various STI tests were requested by the GP, depending on the patient's profile, for example, young patients and heterosexuals were more often tested for chlamydia; MSM and people engaging in paid contacts were tested more for HIV, gonorrhoea and syphilis. GPs did not follow the testing recommendations4 consistently for any of the high-risk groups. Young people with casual sexual relationships, MSM and people (with partners) of non-Western ethnic background were tested for the five main STIs only in one of six persons. HIV tests were not carried out in 64% of the patients for whom it is indicated; among these the larger group is of non-Dutch ethnic background. Chlamydia and gonorrhoea tests were requested for only half of the MSM on STI consultation and GPs rarely took rectal samples for this group. Although recently published results from the Dutch sentinel GP network show that the proportion of HIV-related consultations initiated by the GPs did increase over time from 11% in 1988 to 23% in 2009,13 non-adherence to the guidelines is still apparent and may result in underdiagnosis among high-risk groups. Our survey is limited by the lack of contextual information around the reported consultations; a test request might not be appropriate due to previous testing at an STI clinic or the minimum required time between exposure and test. Nevertheless, further research could explore the reasons for non-adherence to testing guidelines; these can be lack of awareness or training from the GP, but could also relate to patient preferences or practical reasons such as availability of equipment and logistical issues.
When the Dutch sentinel GP network was extended with other practices participating in the Dutch Primary Care Database and STI consultations were analysed based on ICPC-codes,1 ,2 the most recent estimated reporting rate for STI-related episodes was about 1 in 100 patients/year (2010).7 In an earlier study on STI health-seeking behaviour (2001),3 0.8% of registered patients said that they visited their GP because of STI-related symptoms during the previous year; this is the subgroup (43%) in our study with STI symptoms. Two questionnaire-based national studies on sexual health suggest much higher rates: 9% of persons of all ages and 15% of young people (<25 years) indicated to have been tested for HIV and/or another STI in the previous year of whom about 50% said that they had carried out this at the general practice10 ,14; this would equal to an annual incidence of STI consultations of about 5–8 per 100. Hence, 1 in 250 patients/year with a questionnaire in the current study most probably underestimates the number of patients seen at the general practice with STI-related issues, which may have resulted in some biases in the estimates for (determinants of) consult positivity.
Patients attending the GP for an STI-related consultation in the Dutch sentinel GP network belonged less often to known risk groups than clients at STI centres. Although at the general practices a larger proportion of STI consultations was performed for women (59% vs 48% of consultations in STI centres) and at both venues most patients were young, a striking difference was observed for the proportion of MSM; in the Dutch sentinel GP network, 9% of male patients reported having homosexual contacts in comparison with 37% in the STI centres.7 The proportion of ethnic minorities was comparable, but the proportion of Turkish/Moroccan patients was higher in the Dutch sentinel GP network. Similar proportions of male patients reported recent commercial sex contact(s), but for women the 10% in the STI centres7 is clearly higher in comparison with 0.4% in the Dutch sentinel GP network. These results illustrate preferences for low-threshold STI care provided by STI centres among these high-risk groups. Patients more often reported symptoms at a GP consultation than at the STI centre (29%),7 indicating differential health-seeking behaviour depending on a person's health status and risks.
The guidelines for GPs5 and STI centres in the Netherlands are quite similar; implementation is different, however. Owing to government-backed financial endorsement of the standard at STI centres, all patients fitting certain risk-criteria are tested for four STIs and for hepatitis B when indicated. From 2012 onwards, young people (<25 years) are only tested for chlamydia unless they also fulfil other risk criteria. At GPs, patients have to pay for STI tests themselves when their health expenditures are still below their own risk limit of their health insurance. The overall STI test positivity rate in STI centres was lower (14%) compared with the positivity rate in the Dutch sentinel GP network (28%). Higher rates at GPs were found for chlamydia, HSV and condylomata; the latter two probably resulting from the fact that they are mostly diagnosed after experiencing symptoms. In both databases, chlamydia was predominantly found in young, heterosexual patients, often notified by their partners. Gonorrhoea, HIV and syphilis were diagnosed more often in STI centres, often in MSM and CSWs, with high-risk groups commonly opting for STI centres rather than GPs.
The GP is an important provider of STI care, not only in the Netherlands, but also in other countries. In Europe, testing for chlamydia is carried out in primary care in 23 of 29 countries and reported as the most common venue for testing in 11 countries.15 In the UK, during follow-up of a chlamydia screening study, around four-fifths of women in the study had paid at least one visit to the GP in a 12-month period, but only 14% had visited a specialised genitourinary medicine (GUM) clinic. With increased STI risk, that is, the number of reported sexual partners, women were more likely to have visited a GUM clinic.16 Opportunistic STI testing at the GP is an important tool in STI control in several countries (USA, Sweden and the UK), and could also work in the Netherlands, since annually about 78% of Dutch people visit their GP.17 Especially for HIV, GPs could play a more proactive role in testing high-risk groups by closer adherence to the guidelines, with the aim to access the population unaware of their positive HIV status, which is still quite high in the Netherlands (estimated in 2008 at 40%18). We observed a large variation in the number of HIV tests per practice; on an average, only 0.13% of patients were tested per year. In the general practice in two different areas in England, HIV testing rates were higher; HIV testing rates varied from 0.6 to 10.4 (per 1000 patients aged 15–44 years).19 In our study, only one-third of consultations in defined high-risk groups of MSM and patients of non-Western ethnicity included a test for HIV. In Australia, primary care adherence to the guidelines of annual HIV testing in MSM was in the same range: only 35% of MSM were retested at 1 year.20
Encouraging GPs to take a more proactive role in STI care could be challenging where workload for GPs is high. Previous studies identified factors that could act as motivations or barriers to overcome these challenges. On the one hand, practical tools, such as sufficient (financial) incentives and support, could be a possible motivation for more proactive testing practices, that is, of chlamydia tests as was shown in an intervention setting in England21 while productivity goals could discourage such practices.22 Increasing clinician experience with patients attending the GP for an STI-related consultation and use of standardised (online) protocol sheets may help improve the quality of care,23 ,24 as well as accessible and relevant continuing medical education.25 Raising awareness and increasing collaboration improved STI services in a US study.26 STI care may also be hampered by GPs attitudes towards STIs, such as limited confidence in the ability to change patients’ behaviour, time constraints and lack of feeling responsible for delivering prevention services.27 Within GP practices, training and delegation of well-protocolled STI testing to practice nurses and/or auxiliaries also opens opportunities for a more proactive approach.
In conclusion, in the Netherlands, GPs could play a stronger role in testing patients with STI-related questions according to the guidelines and addressing STI issues when high-risk individuals come for consultation. Extra GP training and raising awareness may contribute to bridge this gap, delegation to well-trained practice nurses and/or auxiliaries as well as addressing potential financial barriers for STI testing on the patients’ side (no complete coverage by health insurance). Recently, in September 2013, an updated version of the STI guidelines for GPs has been launched, focusing more on testing in high-risk groups; this might give a new impulse to STI care in the general practice in the Netherlands. In future, open discussions about testing practices, identifying motivations and barriers to test could improve adherence to guidelines and explore ways to further implement proactive testing in general practices, which are necessary to reach high-risk patients and limit missed diagnoses.
Acknowledgments
All general practitioners who participated in the Dutch sentinel GP network from 2008 to 2011 are gratefully acknowledged.
References
Footnotes
-
Contributors IVFvdB designed the study and composed the questionnaire with contributions of JEAMvB and GAD. GAD coordinated the data collection in the Dutch sentinel GP network. SCMT analysed the data. SCMT and IVFvdB interpreted the data and drafted the manuscript. JEAMvB, GAD and MABvdS contributed to the drafting and revising of the article. All authors read and approved the final manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval Ethical approval for the study was not necessary following Dutch law as the study used anonymous patient data collected for routine surveillance.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.