Article Text

Abstract
Identification of causes of changes in prevalence and incidence of HIV at a national level is important for planning future prevention and intervention needs. However, the slow progression to disease and the sensitive and stigmatising nature of the associated behaviours can make this difficult. Changing rates of incidence are to be expected as an epidemic progresses, but separating background changes from those brought about by changes in behaviour and interventions requires careful analysis. This paper discusses the criteria required to determine whether observed changes in HIV prevalence are the result of changes in behaviour.
- AIDS, acquired immune deficiency syndrome
- HIV, human immunodeficiency virus
- STI, sexually transmitted infection
- UNAIDS, Joint United Nations Programme on AIDS
- behaviour change
- HIV
- epidemiology
- incidence trends
- surveillance
Statistics from Altmetric.com
- AIDS, acquired immune deficiency syndrome
- HIV, human immunodeficiency virus
- STI, sexually transmitted infection
- UNAIDS, Joint United Nations Programme on AIDS
The devastating scale of the HIV epidemic in many sub-Saharan African countries is a challenge to national and international policy makers.1 Development and welfare in the region depend upon mitigating the impact of mortality and morbidity in those already infected and preventing the further spread of infection. To understand prevention needs, epidemiological studies have to identify current patterns of HIV spread and coverage of effective interventions. This is complicated in the case of HIV because the slow progression to disease means that infection data often represent historical trends and because the behaviours exposing individuals to infection are private, sensitive, and often stigmatised. Nonetheless, if evidence of widespread behaviour change and consequent reductions in HIV spread is available then we should seek to learn available lessons.
At a national scale the burden of collecting and presenting data can often prevent a considered exploration of trends and alternative explanations for the observed patterns. Thus, the Joint United Nations Programme on AIDS (UNAIDS), the World Health Organization (WHO), and the United Nations Children’s Fund (UNICEF) sponsored a meeting of the UNAIDS Reference Group on Estimates, Modelling, and Projections in November 2004 in Harare. National epidemiologists were invited and asked to review biological and behavioural surveillance data. The selection of countries invited, although non-scientific, was made in order to include many where there had been a suggestion of declining HIV incidence. In this supplement the epidemiology of HIV in a number of these countries is described along with papers recommending best practice in data collection and analysis, and a multi-country modelling study which attempts to inform the interpretation of the country specific data.
Here we introduce the challenge of detecting and understanding changes in the risk of HIV infection at a national level in generalised epidemics.
THE NATURAL HISTORY OF AN EPIDEMIC AND CAUSES OF CHANGING PREVALENCE
As an epidemic progresses, changes in rates of incidence are to be expected and separating out these background changes from those brought about by changes in behaviour requires careful analysis. The incidence of an infectious disease is a non-linear function of the number of infectious and susceptible individuals within the population.2 Following a period of rapid growth at the start of an epidemic, we would expect incidence of new infections to decline because the number of high risk susceptible individuals falls due to prior infection. Whether this decline in incidence leads to the epidemic fading away, falling to a low steady incidence and prevalence, or maintaining a high incidence and prevalence, depends upon the way in which new susceptibles are recruited.3 Declines in numbers of new cases are often interpreted as a reduction in risk due to interventions, when they may actually represent reduced numbers of susceptibles. Likewise, reductions in prevalence of infection which follow on may also be the natural history of an epidemic rather than changes in risk. However, changes in risk are possible, in the population as a whole, in specific high risk fractions of the population, or in the new cohorts entering the population.
Uncertainty over causes of change in HIV incidence and prevalence is not new. In 1997 a similar meeting was sponsored by UNAIDS to explore trends in Uganda and Thailand with the following questions about reductions in the prevalence/incidence of HIV observed at the population level:
-
Are the observed changes valid in a statistical sense?
-
Are the observed changes a reflection of the natural progression of the epidemic?
-
Are the observed changes a product of changes in behaviour?
-
Are the observed changes a product of interventions?
The report concluded that: “Despite the complexity in interpretation there are success stories, most visibly in Thailand at a national scale and in selected groups, such as … young adults in Uganda.”4
In these two national level examples, Uganda and Thailand, the triangulation of data from a number of sources showing reductions in HIV incidence in the youngest age groups and associated changes in risk behaviour in cross-sectional studies provided a convincing narrative. In Uganda the reduction in HIV prevalence among 15–24 year old women attending antenatal clinics, where infections would be too recent to be removed by mortality or decreased fertility, was seen as a marker of reduced HIV incidence.5 In addition, studies in some urban locations showed associated decreases in numbers of sexual partnerships.5 In a modelling exercise the only straightforward way to re-create the observed patterns of HIV prevalence was to include a decline in HIV risk.6 Thus, the decline in risk in young adults in Uganda was convincing, but how much was a direct consequence of interventions, as opposed to societal changes in response to observing the consequences of AIDS, was difficult to gauge. In Thailand, the correspondence between intervention activities in the 100% condom programme and the observed behaviour changes, where there was a reduced contact of young men with sex workers, increased condom use in commercial sex, and declines in incidence of bacterial STIs indicated the interventions were an important driver of change.7,8
Both of these examples of changing risk behaviour reducing the spread of HIV and decreasing the prevalence of infection were important examples of what could be achieved at the national level in the fight against HIV. However, both occurred in the early 1990s following the initial spread of the virus. Have there been any commensurate successes in responding to the HIV epidemic over the subsequent decade? What would be required to determine whether observed changes in HIV prevalence are the result of changes in behaviour?
RELATION BETWEEN PREVALENCE AND INCIDENCE
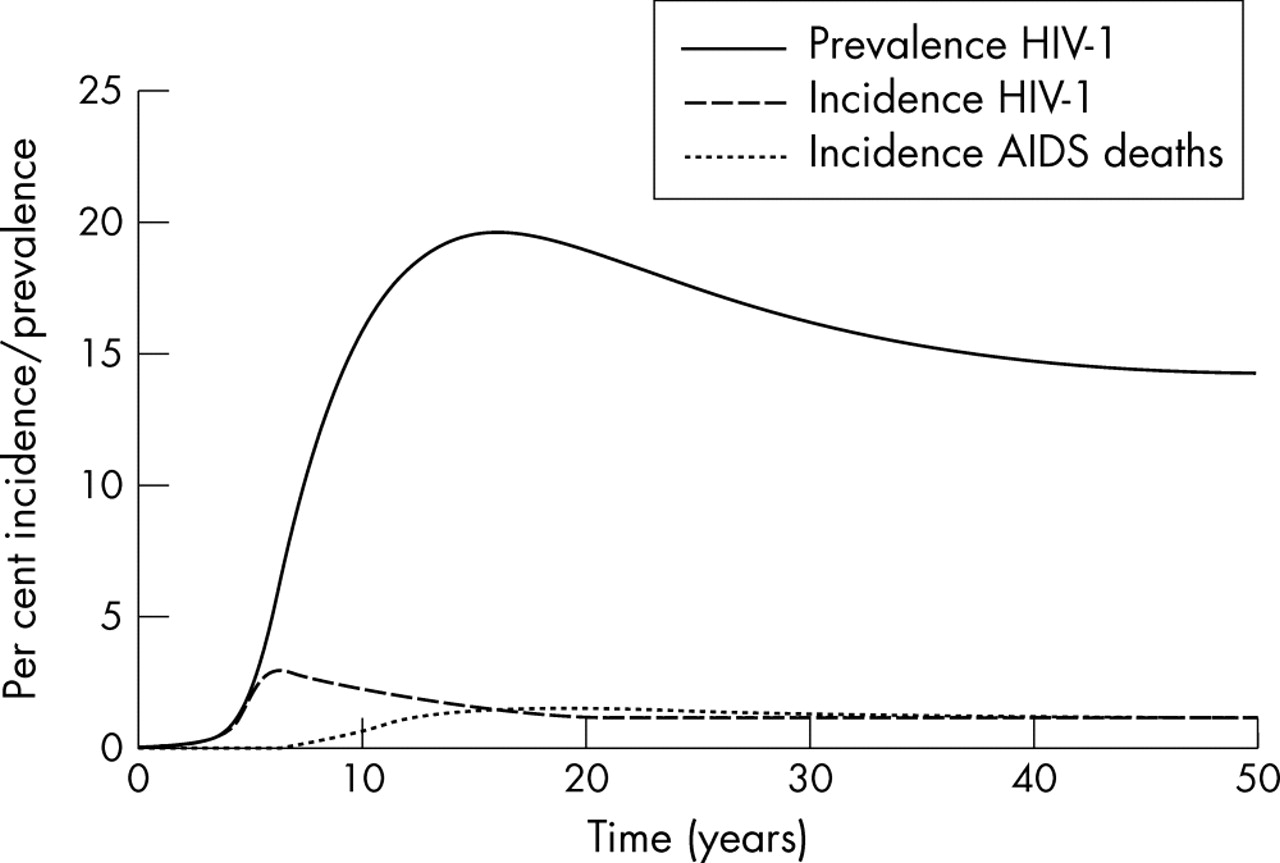
HIV prevalence is determined by the history of the incidence of new infections and the loss of existing infections through mortality. Figure 1 illustrates the time course of a local HIV epidemic and the relation between incidence and prevalence. Early in the epidemic, because of the long incubation period of AIDS, incidence of HIV will outweigh mortality, and prevalence of HIV will rise. However, over time mortality will balance incidence, and at a steady state, prevalence is a function of the incidence and duration of infection. If we define incidence per person, irrespective of current HIV status, then prevalence will simply be the product of incidence and mean duration of infection (d), whereas if incidence (I) if defined per susceptible the product of incidence and duration of infection is the odds of an individual being infected and prevalence (P) is given by the relation: P = Id/(1−Id). From this steady state, a further decline in incidence will result in a fall in prevalence. However, as already described, we initially expect incidence to decline as an epidemic progresses as those left susceptible are progressively those who have lower risk behaviours and hence less exposure to infection. This decline can occur prior to increased mortality allowing prevalence to increase as incidence declines (fig 1). Likewise, when mortality does become extensive, HIV prevalence can decline reflecting the earlier fall in incidence. Thus, it is possible to see a decrease in HIV prevalence when there is no concurrent decline in incidence as observed in the Rakai, Uganda, by Wawer and colleagues.9
{kind=link}
Relation between incidence, prevalence, and AIDS associated deaths in a simulated HIV epidemic.
Prevalence of HIV infection is a good measure of the extent of the HIV epidemic and the subsequent burden of associated morbidity and mortality. As an instantaneous measure prevalence can be estimated from cross-sectional surveys, and since it reflects cumulative infection numbers it can often be reasonably estimated from a practical sample size. However, it is a slowly evolving measure, whereas the incidence of infection will respond immediately to changes in patterns of risk behaviour. Unfortunately incidence is less easily monitored, requiring study of a cohort, or, more recently, the use of special testing methods.10 Testing algorithms that identify recent infections—that is, those in the last half year—may in the future allow regular monitoring of incidence especially as testing due to prevention of mother to child transmission and for enrolment in treatment programmes becomes more common. However, there is currently no history of incidence for comparison and, possibly more problematic, large sample sizes are required to estimate incidence accurately because of the low numbers of infections which will occur over a half year period.
SENTINEL SURVEILLANCE DATA
To initially estimate the scale of HIV spread in a population, those with many risky contacts, such as men who have sex with men, injecting drug users, and sex workers, along with those more representative of the population as a whole, such as women attending antenatal clinics and military recruits, should be screened for infection. Thereafter, in locations with generalised epidemics, to monitor trends in the epidemic, periodic anonymous testing of women attending a sample of antenatal clinics has been common practice. Comparisons of antenatal and household based surveys have identified biases in women who become pregnant and attend antenatal clinics in representing all women within a population, and frequent differences in prevalence between men and women.11 Some of these biases, such as the ratio of HIV infection in men and women and the infertility associated with infection can change as an HIV epidemic ages. Changes in the former are unlikely to cause misidentification of declines in overall HIV risk, since prevalence due to increasing mortality would typically fall first among men.12 In contrast, as women infected with HIV progress towards AIDS, infection associated sub-fertility could reduce their presence in antenatal samples.13 However, this could be counteracted by a decrease in infertility caused by bacterial STIs as those more likely to be infertile are also more likely to acquire HIV and suffer increased mortality.14
In part to reduce the influence of such biases and the influence of mortality, second generation HIV surveillance recommended the oversampling of women aged 15–24 years and the concentration of analyses on this age group.15 Women in this age group represent those who have recently entered the sexually active population and hence their HIV infections will consistently represent infections from the past decade. This does still leave some problems since HIV associated mortality seems to be reasonably high among those in their early twenties,16 and also if women delay sexual debut they reduce both their risk of acquiring HIV and their risk of pregnancy. Thus, reduced risks of HIV infection solely due to an increase in the mean age of sexual debut will not be reflected in reduced prevalence in antenatal samples.17 Those old enough to be sexually active but young enough to have only been exposed to HIV for a few years best represent recent incidence of infection.
Reductions in the prevalence of HIV in young women are the best indicator of reduced incidence but often these may be insignificant, representing small numbers of cases, local or transitory. The observed changes in HIV prevalence in multiple sites in Zambia illustrates very well how the epidemic can move in different directions in the same country.18 Either such changes are random fluctuations in measuring HIV prevalence or represent local transmission dynamics where multiple local epidemics are in different phases. Care needs to be taken that observed reductions in HIV incidence and risk behaviour are not simply local effects, and that they continue. It is crucial that sample sizes, confidence intervals, and potential biases are considered in assessing HIV surveillance data.
BEHAVIOURAL DATA
In addition to a focus on young women, second generation surveillance has promoted the collection of behavioural data that can indicate where exposure to the virus is occurring and to monitor changes in behaviour. Patterns of risk behaviour should direct intervention programmes, but, additionally, time series data on risk behaviours inform interpretations of patterns of HIV incidence. Risk of HIV infection for those susceptible depends upon unprotected sexual or blood related contacts with those already infected. Therefore, changes in behaviours which reduce contacts with those potentially infected, such as decreased numbers of recent sexual partnerships or increased condom use, are the key indicators of changes in risk behaviour responsible for reduced HIV incidence.19
To explore changes in behaviour, individuals could be prospectively studied, but in such cohort studies observed alterations could be associated with ageing or selection biases for those who have remained within the cohort. Thus, for cohort studies to be informative they need to be open and representative of the same demographic groups over time. More common are serial cross-sectional studies such as the Demographic and Health Surveys and the UNICEF–Multiple Indicator Cluster Surveys (MICS). Here a number of mechanisms could contribute to observed changes in sexual behaviour:
-
changing age and sex structure of the population independent of HIV infection
-
direct demographic impacts—differential AIDS associated mortality reducing the presence of high risk individuals within the population
-
indirect demographic impacts—altered opportunities for sexual partnership formation due to the removal of high risk individuals from the population
-
conscious changes in risk behaviour brought about by changes in social norms and individual perception of risk due to experience of morbidity and mortality within the population
-
conscious changes in risk behaviour brought about by direct exposure to intervention programmes.
The distinction between the last two is somewhat blurred since education and information is required to guide changes in norms, perceptions of risk, and appropriate behaviour change.
Sexual behaviour studies rely on interviewees to report correctly often sensitive and stigmatised activities and are consequently particularly vulnerable to social desirability and recall biases. Methods have been developed such as self-completion forms, computer assisted audio cassettes and confidential voting methods to increase the accuracy of reports.20,21 While such methods elicit reports of increased risk, it is impossible to be fully confident of validity. However, to detect changes in risk, consistency of reporting biases is more important than the complete eradication of biases. Hence, comparison should ideally be between surveys with similar methods of sampling and interviewing participants. Unfortunately, social desirability biases are likely to change in response to the spread of HIV and associated information and education activities.
MEASURING THE EFFECTIVENESS OF INTERVENTIONS
Attribution of behaviour change to particular interventions is a further link that is difficult to establish. Here it is helpful to measure coverage of interventions and exposure in populations to interventions, attitudes to interventions, whether contact with interventions occurs before reported changes in behaviour, and whether the behaviour changes are those associated with interventions. Such observational evidence is a poor relation to randomised controlled trials in assessing the efficacy of interventions.22 Recent community randomised trials have suggested that what are believed appropriate interventions could sometimes have little impact on HIV incidence.23,24 However, randomised controlled trials, particularly those where populations are the focus of the intervention and unit of analysis have some distinct problems. Foremost, the complexity of behaviour interventions aimed at whole populations means that actually carrying out these interventions appropriately can run into many logistical and political problems. In interpreting a negative community randomised trial result for a behaviour intervention there will always be concern that an intervention that could work was not appropriately implemented. This relates to the external validity or generalisability of the trial—even when a trial does work, questions remain over whether it will be equally successful in other social, political, and epidemiological contexts.25
Trials are generally small in scale and the interventions implemented in a research context. This raises questions of the impact of increasing scale and problems of sustainability when trial interventions are taken to a national level. In addition, the delay incurred in carrying out trials of interventions that are believed to work is often unacceptable. Despite these problems, repeated examples have shown that interventions believed to work do not do so when actually tested or have relatively little measurable impact on secular trends at the population level.26
CONCLUSIONS
Where does this leave us in developing an evidence based prevention response to HIV? Observational studies carried out at a national level automatically deal with the problems of scale, sustainability, and preventing delay. Both internal and external validity in analyses of the effectiveness of the intervention and its applicability to other circumstances rely on the collection of good quality, comprehensive data and cautious analysis. However, if national level changes can be confidently identified without trials, as has been the case in Thailand and Uganda, then much can be learned. It is possible to compare the expected course of the epidemic with that observed and estimate the magnitude of change in risks within the population. Further, with data on behaviours within populations it is possible to determine which interventions are likely to have influenced HIV incidence. Such evidence does not provide definitive measures of effectiveness but does create plausible explanations that can inform policy.
In this supplement, sentinel HIV prevalence and sexual behaviour data are presented to explore recent trends in generalised epidemics. HIV prevalence data are compared with a null model of HIV prevalence trends, where the decline in incidence in the absence of behaviour change is minimised. Some important results emerge: in urban Kenya and Zimbabwe convincing evidence of a decline in prevalence associated with reductions in incidence are presented. Indeed in Kenya the decline in prevalence is more marked than would be expected from the concomitant behavioural data. For Haiti there is a similar decline but the lower prevalence is restricted to one time point. In urban Ethiopia the gradual decline in prevalence is slower and less indicative of a change in risk. Elsewhere the news is less good, with no evidence of declining prevalence in Malawi, Rwanda, and Cote d’Ivoire. In Uganda we see the declining prevalence that has been the focus of study and debate in generating prevention lessons. Similar study is warranted in Kenya and Zimbabwe.
REFERENCES
Footnotes
-
GPG and SG thank UNAIDS, the UK MRC, The Wellcome Trust, and the CDCP Zimbabwe for grant support
-
Competing interests: none declared
-
Edited by N Walker, H Ward and R Miller