Article Text

Abstract
Background: In 2007, a survey in Rawalpindi found the prevalence of hepatitis C virus (HCV) in injecting drug users (IDUs) to be low (17%), despite widespread needle/syringe sharing. This analysis uses modelling to explore hypotheses for the low prevalence of HCV to project the future HIV/HCV epidemic and to estimate the impact of a generic intervention.
Methods: An HIV/HCV transmission model was developed and parameterised using data from Rawalpindi. By incorporating different assumptions about the relative frequency/importance of needle/syringe sharing events among “strangers” and people they have shared with before, and undertaking extensive uncertainty analyses to fit the model for each scenario, the validity of different hypotheses for the low HCV prevalence was determined. Model fits were used to project the future HIV/HCV epidemic and the impact of reducing needle/syringe sharing among different IDU subgroups.
Results: The model projections suggest that the low HCV prevalence in Rawalpindi is probably due to most HIV/HCV transmissions occurring in a small IDU subgroup that shares needles/syringes frequently with strangers, with most needle/syringe sharing incidents being low risk. Projections suggest that the prevalence of HIV in IDUs will increase to 5–12% by 2015, and the prevalence of HCV will increase if HIV increases HCV transmission. Moderate reductions in needle/syringe sharing (>40%) could reduce the number of HCV/HIV infections (∼45%) if all IDUs are reached, although less impact is achieved if high-risk IDUs are not reached.
Conclusions: Despite many needle/syringe sharing events possibly being low risk in Rawalpindi, the model projects that the prevalence of HIV/HCV in IDUs is likely to increase. This highlights the importance of intervening in this low prevalence setting.
Statistics from Altmetric.com
Hepatitis C (HCV) and HIV cause substantial morbidity and mortality. Worldwide, 33 million people are estimated to be infected with HIV1 and 170 million with HCV.2 HCV and HIV can be easily transmitted through infected needles/syringes,3 4 and HCV infection rates are normally very high among injecting drug users (IDUs).5 As with HIV, HCV infection is a public health concern because most HCV infections do not resolve6 but become chronic, frequently leading to cirrhosis of the liver and possibly liver cancer and death.7
Reducing HCV/HIV transmission through injecting drug use is critical to preventing these infections in most countries. However, although needle/syringe exchange interventions and oral methadone substitution therapy are associated with reduced HIV transmission,8 9 the evidence for their impact on HCV transmission is modest,10–12 and there is no clarity on the scale of activity required to impact on both infections.
There are limited data on the transmission of HIV/HCV among IDUs in Pakistan,13–19 with data suggesting that the HCV prevalence is high (60–94%)13–15 and the HIV prevalence was low (<10%13) until recently. However, since 2003–4 a number of surveys have found prevalences of HIV of >20% in some cities, with some showing rapid increases.18 19
In 2007, two behavioural and biological surveys were undertaken among IDUs in Rawalpindi (n = 302) and Abbottobad (n = 102) in northern Pakistan, two settings with no current IDU interventions.20 These studies found that, among IDUs, the prevalences of HIV (2.7% in Rawalpindi) and especially HCV (17.3% in Rawalpindi) were low compared with many IDU populations in Pakistan.13–15 19 This was despite a high prevalence of HCV (6%) in the Rawalpindi general population,21 and IDUs reporting frequent injecting (on average 720 per year) and needle/syringe sharing (41% reported sharing needles/syringes in an average of 46% of injecting episodes). In this study, a mathematical model is fit to the IDU HIV/HCV epidemiological data from Rawalpindi to explore possible hypotheses for the low prevalence of HCV in this setting. The model is used to project the future HIV/HCV epidemic in Rawalpindi and to estimate the impact of a specific reduction in needle/syringe sharing.
METHODS
Model derivation
A deterministic compartmental model was developed to simulate the transmission of HCV/HIV among IDUs with different levels of needle/syringe sharing. The HCV transmission model was adapted from a previous model22 to incorporate recent evidence suggesting that IDUs who resolve their infection can be susceptible to reinfection.23–27 The model assumes IDUs enter an acute phase of infection once they are infected, and either resolve their infection after a number of months or progress to lifelong chronic infection. A proportion of those that resolve are assumed to become immune, and the remainder becomes susceptible again. All infected subjects develop an antibody response during their acute phase.
The model includes three behavioural subgroups of IDUs depending on whether they do not share needles/syringes (inject with a previously used needle/syringe) or share with a low or high frequency. The model simulates the transmission of HCV/HIV over time and includes two subgroups for those that are new injectors and those that have been injecting for longer. IDUs leave the population if they cease injecting, die due to overdose or experience severe HIV-related morbidity.
The HIV transmission model has the same behavioural subgroups as the HCV model and assumes that, once a susceptible person is infected, they progress to a high viraemia phase of infection, following which they progress to a longer stage of low viraemia, a short period of high viraemia before AIDS, and then AIDS.
The model also follows the joint infection state of each IDU and assumes that HIV infection effects the transmission and natural history of HCV. Because of evidence that HIV infection increases both the HCV viral load in co-infected IDUs28–32 and the probability of mother-to-child HCV transmission,33 the HCV transmission probability was assumed to be heightened in co-infected IDUs. Second, the probability that an HCV infection resolves was assumed to be reduced in HIV co-infected individuals,28 29 34–36 as was the probability that they develop protective immunity.25 35
Because of the low sexual behaviour of IDUs reported in the survey (IDUs report a median of one sexual partner per year and less than one sex act per month), the low prevalence of sexually transmitted infections (<2% have Neisseria gonorrhoea or Chlamydia trachomatis) and the fact that all HIV positive IDUs are HCV seropositive, the model did not simulate the sexual transmission of HIV. A detailed model is shown in the online supplementary material.
Model parameterisation
The behavioural and epidemiological data used to parameterise and fit the model for Rawalpindi were largely obtained from the survey undertaken for this project20 and are shown in tables 1 and 2. Because an IDU’s main source of needles/syringes was shown to be a major predictor for HCV transmission and IDU risk behaviour, the IDU population in the model was normally stratified by whether they report never needle/syringe sharing, or report needle/syringe sharing and get their needles/syringes from a reliable provider or not. However, in one scenario (see next section) the IDU population was stratified by whether they did not share needles/syringes or whether or not they shared needles/syringes only with people they knew in the last week.
The biological data needed to parameterise the model were obtained from the literature, usually directly from studies (table 3). However, some parameters were more difficult to estimate, such as the HCV transmission probability and the degree to which HIV co-infection increases HCV infectivity (see online supplementary material). Other parameters obtained from the literature included estimates for the start date of the HIV/HCV epidemics and the HCV prevalence in the general population. A pilot HIV surveillance study in Rawalpindi in January 2005 found no HIV-infected IDUs (n = 200)37 and, as surveys before 2003 generally found little HIV in Pakistan,13 the HIV epidemic in Rawalpindi was assumed to start between 1995 and 2005. Conversely, since HCV has been highly prevalent in the Rawalpindi general population since at least 2001,21 the HCV epidemic in Rawalpindi was assumed to be endemic before HIV appeared.
The uncertainty bounds in tables 1, 2 and 3 are either the 95% confidence intervals obtained from survey data or meta-analyses, or the upper/lower bounds derived from different studies. Generally, values within these uncertainty bounds were directly used in the model, although some behavioural parameters were combined first. The only exceptions to this were the proportion of IDUs who reported ever sharing and the proportion who reported sharing with people they have not shared with before (defined as “strangers”), which were both allowed to be greater than the survey suggested since evidence suggests that IDUs may accidentally share needles/syringes or may under-report needle/syringe sharing behaviour,38 as suggested by the relatively high HCV prevalence among IDUs who reported never needle/syringe sharing in our survey (14.7%).
Model fitting
Because of uncertainty in all model parameters, a fitting algorithm was used to obtain multiple model fits to the HIV/HCV epidemiological data from Rawalpindi. The algorithm involved a number of steps. First, 400 parameter sets were randomly sampled from the HCV/HIV biological parameter uncertainty bounds. Then, because the low HCV prevalence seemed contrary to the needle/syringe sharing behaviour reported in the survey, five different scenarios of 400 behavioural parameter sets were randomly sampled. These behavioural scenarios were developed to explore different hypotheses for why there is a low prevalence of HCV and a high prevalence of HCV co-infection in Rawalpindi. Through fitting the model, while assuming different behavioural hypotheses, the degree to which each could produce the observed epidemic patterns was determined and so the validity of each hypothesis could be compared.
The five scenarios are described in detail in the table given in the Appendix. Broadly, because the epidemiological analysis undertaken by Platt et al20 found that an IDU’s main source of needles/syringes was an important behavioural predictor of HCV infection, the model was initially stratified by whether or not they shared syringes and, if they shared syringes, by whether they got most needles/syringes from a reliable or unreliable source. Scenarios 1–4 all use this stratification but make different assumptions about the relative transmission risk of syringe sharing incidents with people they have or have not shared with before (“strangers”). These assumptions were developed iteratively to explore possible hypotheses for why the HCV/HIV prevalence could be low when the frequency of syringe sharing is not. Lastly, scenario 5 was developed to explore whether a model that only considers needle/syringe sharing events with “strangers” and stratifies IDUs by whether they share never/infrequently/frequently with “strangers” could better mimic the observed trends. The motivation for this scenario came from the 100% prevalence of HCV among HIV infected individuals (n = 8), suggesting that the HIV epidemic may be concentrated among a group of high-risk IDUs.
Details of the parameter ranges used in these behavioural scenarios are shown in table 4 and details of how these ranges were derived from the survey data are shown in the table in Appendix 1. All other behavioural parameters were the same across the scenarios.
For each of these needle/syringe sharing scenarios, the model was run for 160 000 sampled parameter sets (400×400). For each simulation, the HCV transmission model was first run until the HCV prevalence reached equilibrium. Then, only if the projected HCV prevalence was below the upper bounds of the survey estimates, the HIV transmission model was run for 2–12 years, the assumed duration of the HIV epidemic up until the survey (2007). If at any time the projected HCV prevalence (overall, ⩽2 and >2 years injecting, and by source of needles/syringes if not scenario 5) and HIV prevalence (overall) were all within the confidence limits of the epidemiological data in table 1, then that simulation became a model fit and the model went on to the next parameter set. The validity of the model fits for each scenario was then checked against whether they projected the observed HCV prevalence among HIV-infected IDUs.
Model analyses
The overall accuracy and validity of the model fits for each scenario were used to determine which behavioural hypothesis was most consistent with the HIV/HCV epidemic in Rawalpindi. The model fits for this scenario were used to determine which parameter values/combinations were most consistent with these epidemiological patterns, to project the future HIV/HCV epidemic in Rawalpindi and to project the impact of a generic IDU intervention. The intervention was assumed to be accessible to all IDUs or just IDUs in the lower risk needle/syringe sharing category, and had the effect of reducing the average needle/syringe sharing frequency by 0–99%. To undertake these projections, the validated model fits were first repeatedly rerun with specific HIV epidemic durations assigned to each, and only the simulations that still fit the data were used. This was done because the initial model fitting algorithm stopped when the model fit the data, and so did not randomly sample the HIV epidemic duration.
RESULTS
Insights from model fitting
Table 4 shows that scenarios 1 and 2 did not produce any model fits, with the projected HCV prevalences being much higher than survey estimates even for the lowest bound HCV transmission probabilities. In contrast, scenarios 3, 4 and 5 all produced model fits that agreed with the observed HIV/HCV prevalence data, with each producing 111, 100 and 743 model fits, respectively. However, only some model fits from scenario 5 agreed with the survey’s high HCV prevalence among HIV-infected individuals (125/743 model fits). These validated model fits involved 10 of the 400 behavioural parameter sets and 43 of the 400 biological parameter sets.
For the validated model fits from scenario 5, most of the model parameters had similar ranges (posterior ranges) to the original uncertainty range used for that parameter (prior range). However, exceptions included the HIV and HCV transmission probabilities which took values towards the upper and lower limits of their ranges, respectively (see online supplementary material). Also, the frequency of risky needle/syringe sharing among lower risk IDUs, the proportion of IDUs who are higher risk needle/syringe sharers, and the rate at which older IDUs (injecting >2 years) cease injecting were all towards the lower end of their ranges, whereas the degree to which IDUs mix with IDUs of the same needle/syringe sharing activity and the proportion of IDUs who are lower risk needle/syringe sharers were both towards the upper end of their ranges.
Many of the model parameters were also correlated across the different validated model fits. The parameters that had correlation coefficients above 0.4 and had visible correlations are shown in the online supplement, with all correlations being understandable.
Epidemic projections
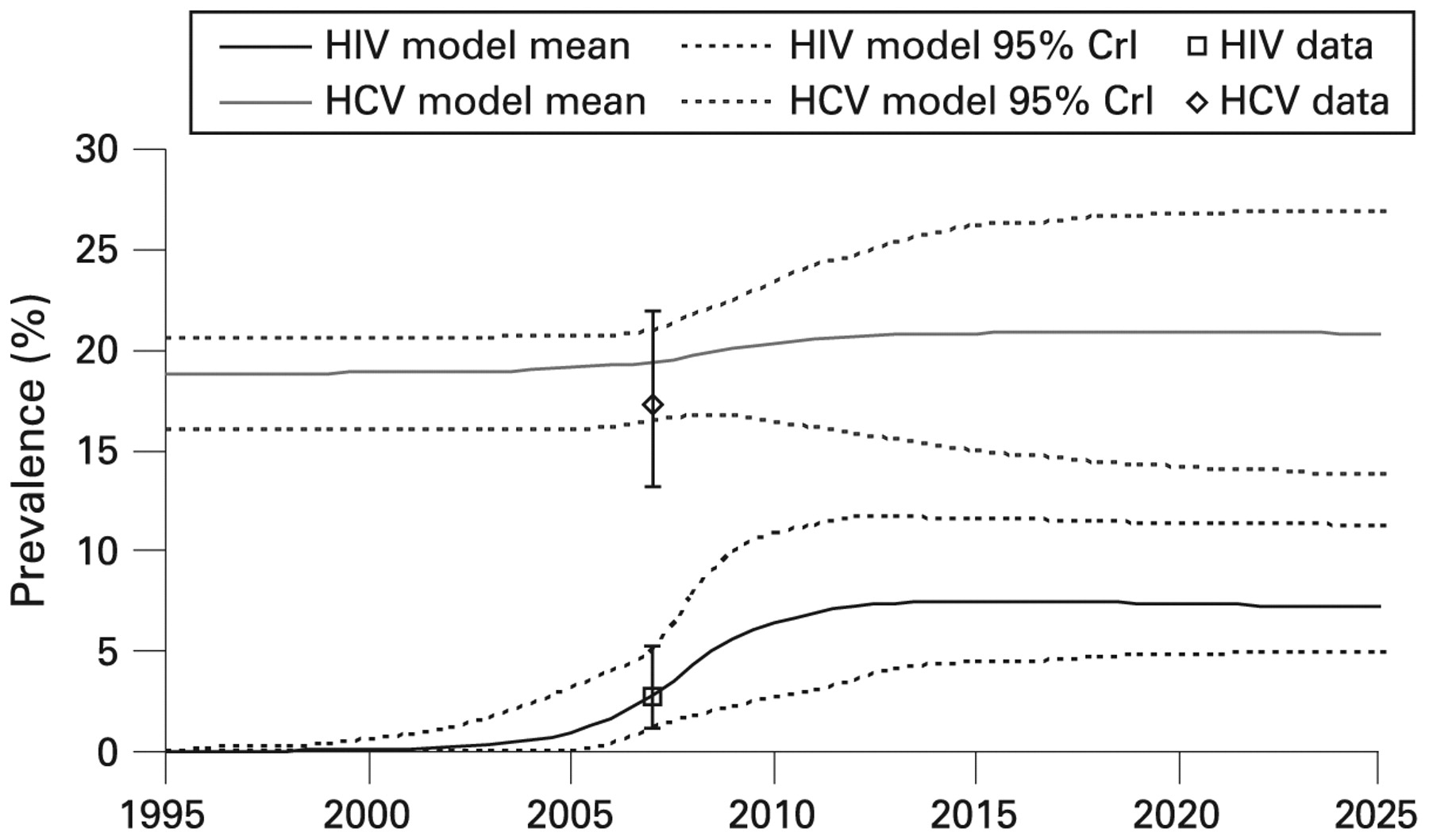
The dynamic projections for these validated model fits agree well with survey HIV/HCV prevalence data and suggest that the prevalence of HIV among IDUs in Rawalpindi could increase to 12% by 2013 (fig 1). Conversely, the prevalence of HCV could increase or decrease over the same period, to as low as 14% or as high as 27% by 2027. These contrasting projections are dependent on the degree to which HIV co-infection increases an IDU’s HCV infectivity, with the model projecting that the prevalence of HCV will decrease by 15% (9–28%) by 2027 if HIV co-infection has no effect on HCV transmission, and will increase by about 0–11% or 14–30% if HIV co-infection increases HCV infectivity by two- or three-fold, respectively (see online supplementary material). Indeed, since HIV was introduced (until 2027), the model projects that 25% (0–47%) of all new HCV infections can be attributed to the modelled effect that HIV co-infection has on HCV infectivity, resolution of HCV infection and HCV immunity. Most of this is due to the effect on HCV infectivity (23%, range 0–44%), with each unit increase in the HIV co-infection cofactor for HCV infectivity resulting in the attributable fraction increasing by about 19% (see online supplementary material).

Comparison of survey HIV/HCV prevalence data with projections for the validated model fits for scenario 5. The 95% credibility interval (95% CrI) are the 2.5% to 97.5% percentiles of the model projections. HCV, hepatitis C virus.
Intervention impact projections
The intervention impact projections (fig 2) show that moderate decreases in syringe sharing (>40%) are needed for an intervention that reaches all IDUs to attain noticeable decreases in the prevalence of HIV/HCV over 10 years, but can avert a large proportion of the HCV/HIV infections that would have occurred. Similar decreases in the incidence of HIV/HCV are also seen. However, although substantial decreases in the prevalence of HCV can occur if the decrease in syringe sharing is large (>50%), the model suggests that any decrease will be 35–50% less than the corresponding decrease in the prevalence of HIV and is unlikely to decrease the prevalence of HCV to <10% even after 10 years.

{kind=link}
{kind=link}
Ten-year impact (2009–2019) on the prevalence and relative number of infections averted in Rawalpindi of an intervention that result in different relative decreases in syringe sharing in all IDUs or just in lower risk IDUs. (A) Prevalence of HIV and HCV. (B) Percentage of HIV and HCV infections averted. The 95% credibility interval (95% CrI) are the 2.5% to 97.5% percentiles of the model projections. HCV, hepatitis C virus; IDU, intravenous drug user.
In contrast, any intervention that only reaches the lower risk needle/syringe sharers can only have limited impact, with a 50% reduction in needle/syringe sharing frequency resulting in <26% of all HIV/HCV infections being averted (over 10 years), and possibly even an increase in both the number of HIV infections occurring (due to more partnerships now forming between the higher prevalence higher risk IDUs) and the overall HIV/HCV prevalence compared with current levels. Indeed, because most model fits suggest the overall prevalence of HIV/HCV will increase with no intervention, even an intervention that reaches all IDUs needs to achieve a certain minimum decrease in the needle/syringe sharing frequency (30% for HIV and 10% for HCV) before it will definitely decrease the prevalence of HIV/HCV in Rawalpindi.
DISCUSSION
A dynamic HCV/HIV transmission model was developed that incorporates key biological features of HIV/HCV infection and detailed behavioural/epidemiological data from Rawalpindi, Pakistan. Through extensive model uncertainty analyses, the model was used to explore the validity of different hypotheses for the low prevalence of HCV among IDUs in Rawalpindi. Only one hypothesis could reproduce the observed HIV/HCV prevalence data, with the other hypotheses either projecting very high overall HCV prevalences or low HCV prevalences among HIV-infected individuals. The validity of the hypothesis suggests that many needle/syringe sharing incidents reported by IDUs in Rawalpindi are relatively low risk for transmitting HCV, but there is a smaller high-risk IDU subgroup that shares more frequently with strangers. The small but high-risk IDU subgroup is needed to project the high HCV prevalence found among HIV-infected individuals. Many needle/syringe sharing incidents in Rawalpindi are likely to be low-risk because they occur in small “buddy” groups, as observed elsewhere.39
Take-home messages
The low prevalence of HCV in Rawalpindi is probably due to most HIV/HCV transmission occurring in an IDU subgroup that shares needles/syringes frequently with strangers, with most other sharing incidents being low risk.
The prevalence of HIV in Rawalpindi is likely to increase over the next 10 years, and so will the prevalence of HCV if HIV co-infection increases HCV infectivity.
For low prevalence HIV/HCV epidemics among IDUs, interventions that do not reach higher risk IDUs are likely to have limited impact.
HIV co-infection could be a significant driver of HCV transmission among IDUs even in relatively low HIV prevalence settings.
The model fits for the validated hypothesis were used to give a number of insights. First, they suggest a smaller uncertainty range for the HIV (0.34–1.4%) and HCV (1.5–5.0%) transmission probability per needle/syringe sharing act. Second, they suggest that Rawalpindi will experience an increasing HIV epidemic over the next 5–10 years, with the prevalence of HIV possibly increasing to 12% if risk behaviour does not change. This is similar to the HIV prevalence found in some settings in Pakistan, but lower than others (>30%).19 In contrast, the prevalence of HCV in Rawalpindi could increase or decrease over the same period depending on the amount HIV co-infection increases HCV infectivity. If HIV co-infection has no effect on HCV infectivity, then the prevalence of HCV is likely to decrease due to HIV morbidity whereas, if it increases HCV infectivity twofold, then the prevalence of HCV could increase by 0–11% by 2027, with 17–32% of new HCV infections being due to dual infection with HIV. This illustrates the large effect HIV could have on HCV transmission and highlights the importance of better understanding this interaction.
Lastly, the model projections suggest that moderate decreases in needle/syringe sharing (>40%) are required to result in noticeable decreases in HIV/HCV prevalence over 10 years. However, in contrast with model projections from a higher HCV prevalence setting,22 much less impact is achieved if the intervention only reaches lower risk IDUs. This gives cause for concern because lower risk IDUs may be more readily reached by this type of intervention. Indeed, in some low prevalence scenarios, our analysis suggests that just reaching the lower risk IDUs could sometimes increase the HIV infections occurring. This apparent anomaly could occur in settings where HIV is highly concentrated in the higher-risk IDUs (ie, those more likely to be sharing outside relatively stable sharing groups), and is due to any reductions in needle/syringe sharing among lower-risk IDUs resulting in a smaller “pool” of potential people with whom to share. As a result, higher risk IDUs are more likely to share with other higher risk IDUs, resulting in an increase in the prevalence of HIV among these IDUs.
Study limitations/strengths
One potential limitation of the analysis was that the model did not incorporate the possibility of HIV/HCV transmission through sharing other injecting equipment (such as cookers),40 primarily because of a lack of data on its infectivity and insufficient behavioural data. This may have resulted in our model overestimating the HIV/HCV transmission probabilities, the amount of needle/syringe sharing or the impact of reducing needle/syringe sharing. The use of a deterministic compartmental model also limited the degree to which we could portray the variability in IDU needle/syringe sharing behaviour or simulate how network effects could have produced the observed epidemic patterns.
The analysis also lacked sufficient data on the characteristics of needle/syringe sharing groups, so it was difficult to directly use survey data to parameterise the model. This is an issue because needle/syringe sharing usually occurs within social groups,41 and so highlights the importance of undertaking additional improved epidemiological surveys.
Lastly, it is important to remember that making model projections over 10 years or more involves assuming that IDU risk behaviour will remain the same. Although this is unlikely, the projections are still useful pointers for understanding where current risk behaviours could lead. The accuracy of these long-term model projections was also limited by the availability of epidemiological data from only one time point which made it difficult to determine the type of HIV/HCV epidemic occurring in Rawalpindi.
Despite these limitations, the analysis is still a significant step forward in the use of modelling to understand the transmission of HIV/HCV among IDUs. Previous modelling analyses generally only modelled one infection or the other, and none evaluated the possible interactions between them.42 In addition, no other modelling analysis has considered the prevalence of HCV among HIV-infected individuals, which our analysis suggests could be important for determining model validity.
CONCLUSIONS
We believe that these findings carry important implications for current and future programmes. At the time of undertaking this study, there were no needle/syringe exchange programmes in Rawalpindi. Our model shows that widely accessible needle/syringe exchange programmes could result in noticeable decreases in HIV/HCV incidence. Political analysis has highlighted the acceptability and perceived feasibility of this intervention among the policy elite in Pakistan.43 Rolling out this intervention, stimulating user awareness and use of services in Rawalpindi and other cities should therefore be a priority.
Acknowledgments
The authors thank Matthew Hickman for useful discussions.
APPENDIX
REFERENCES
Supplementary materials
web only appendix 85/Suppl_2/ii23
Files in this Data Supplement:
Footnotes
Additional material is published online only at http://sti.bmj.com/content/vol85/issueSupplII
Funding: Financial support was provided from the UK’s Department for International Development (DFID), a Medical Research Council New Investigators Award (held by PV) and the DFID-funded Research Programme Consortium for Research and Capacity Building in Sexual and Reproductive Health and HIV in Developing Countries of the London School of Hygiene and Tropical Medicine.
Competing interests: None.
Contributors: PV designed the study; LP and SH contributed to the study concept and designed the original data collection; LP undertook numerous epidemiological analyses; PV undertook all model analyses; all authors contributed to the interpretation of results and writing of the manuscript.
The views expressed are those of the authors and cannot be taken to reflect the official opinions of the World Health Organization or the Department for International Development.
Linked Articles
- Correction