Article Text

Abstract
Objectives The WHO has called for a global action plan to control the spread and impact of antibiotic resistant Neisseria gonorrhoeae. We report on key antimicrobial susceptibility (AMS) trends in countries in Latin America and the Caribbean from 1990 to 2011.
Methods Data collected between 1990 and 2011 by up to 23 countries in the Latin American and Caribbean region were aggregated and analysed for overall trends in N gonorrhoeae AMS to six antibiotics. Methods for gonococcal identification, susceptibility testing and interpretation were standardised.
Results More than 21 500 N gonorrhoeae isolates were tested for AMS between 1990 and 2011. The number of countries reporting yearly declined from 17 in the 1990s to 7 in 2011. The first isolates (0.4%, 20/5171) with reduced susceptibility (minimum inhibitory concentration ≥0.125 mg/L) to ceftriaxone were reported between 2007 and 2011. Ciprofloxacin resistance, first noted in the mid-1990s, ranged from 1.6% of isolates tested in 1997 rising to 42.1% in 2010. Overall, azithromycin resistance reached a high of 25.8% of isolates tested in 2008 falling to 1.0% in 2010. Resistance to penicillin ranged between 24.2% in 2003 to a high of 48.5% in 1993. Tetracycline resistance ranged between a high of 61.1% of isolates tested in 2001 to 21.8% in 2010. Plasmid mediated penicillin and tetracycline resistance declined over the period.
Conclusions Gonococcal AMS surveillance initiatives are urgently needed in every country in the region to ensure that effective treatments for gonococcal infections are in place and to better understand emerging trends in gonococcal antimicrobial resistance.
- Antibiotic Resistance
- Neisseria Gonorrhoea
- Surveillance
- Public Health
- Microbiology
Statistics from Altmetric.com
Introduction
Since the introduction of sulfonamides in the 1930s, followed by other classes of antimicrobial agents, Neisseria gonorrhoeae has steadily developed resistance to all agents recommended for the treatment of gonococcal infections. As there are no vaccines against gonococcal infection, effective antibiotic therapy has been a cornerstone of public health control measures for gonococcal infections. Left essentially untreated through inadequate or inappropriate antimicrobial therapy, gonococcal infections can lead to severe reproductive sequelae in women (ectopic pregnancy, infertility) and men. Further, N gonorrhoeae can cause neonatal infection leading to blindness and can increase the transmission of HIV.1 ,2
Treatment of gonococcal infections is empirical and is based on therapeutic guidelines which are usually established nationally.3 In turn, these guidelines are typically based on aggregated current national trends in antimicrobial susceptibility. In regions/countries where no laboratory based diagnostic capability exits for N gonorrhoeae, a syndromic management approach is generally used to diagnose sexually transmitted infections.3 ,4 Appropriate treatment guidelines in these countries should ideally be based on knowledge of the local frequency of resistant phenotypes of isolates. However, many regions lack a laboratory infrastructure which could provide timely reporting of emerging trends in antimicrobial susceptibility and therefore treatment guidelines are often outdated.1 ,3 This is a particularly pressing problem at present because of increasing reports of gonococcal resistance to the last class of antibiotic for which single dose therapy is effective—the third generation cephalosporins (ie, cefixime and ceftriaxone). No new classes of antibiotic or novel treatment options for gonorrhoea have been introduced.5
This steady emergence of resistance of N gonorrhoeae isolates has been ongoing for decades. As early as 1990, the WHO called for a global surveillance network for gonococcal antimicrobial susceptibility (GASP)6 to provide reliable data on current trends, to identify new forms of resistance and to analyse data annually so that the efficacy of recommended treatment regimens could be ascertained. The South American and the Caribbean regions were identified as key participants in this early report. Twenty-two years later, in an urgent attempt to control the spread of antimicrobial resistance in N gonorrhoeae, the WHO has initiated a more comprehensive global action plan.7 The present report summarises aggregated trends in antimicrobial susceptibility across South America and the Caribbean from 1990 through 2011. It reports on the sporadic emergence of isolates with higher minimum inhibitory concentrations (MICs) to ceftriaxone and also highlights the current challenges in implementing a sustainable gonococcal surveillance programme involving all parts of the region. This study builds on and extends previous analyses providing a new perspective on trends in antimicrobial susceptibility in Latin America and the Caribbean (LAC) over two decades.
Materials and methods
Participating countries and data collection
The participation of various countries in the GASP Surveillance Program for LAC (GASP-LAC) has been documented previously.8–13 The present study represents new pooled data building on and extending previous periodic analyses collected over two decades.8–13 Before each period of data collection (1990–1999, 2000–2009, 2010–2011), detailed questionnaires were sent to potential participant countries to document capability, laboratory methods and reference strains used; as well as to document the extent of antimicrobial surveillance undertaken. These questionnaires complemented precomprehensive and postcomprehensive laboratory training programmes.8 ,9 Consensus has been achieved across the region regarding gonococcal identification and susceptibility testing methods8 ,9 and these methods have been available on the internet and are updated regularly (http://www.gasp-lac.net). Overall, 41 countries were contacted to participate in the GASP-LAC; between 1990 and 2011, GASP surveillance was conducted at various levels (ie, national, local, ongoing, periodic) in 23 countries.
Number of isolates analysed 1990–2011
Between 1990 and 2011, a total of 21 592 N gonorrhoeae isolates were tested for antimicrobial susceptibility as reported from 23 countries.8–13 Overall, the largest number of isolates was tested in Argentina (26.1%, 5635/21 592), followed by Chile (21.2%, 4572/21 592) and Brazil (14.0%, 3017/21 592). Argentina and Uruguay (3.4%, 734/21 592, of all isolates tested) reported results continuously between 1990 and 2011. Chile reported between 1994–1996 and 2000–2011, while Brazil reported results in 1998 (n=81)12 and between 2000 and 2009.9 Venezuela (5.3%, 1139/21 592, of all isolates) reported results for the entire period except for 1999 and 2009. Peru (2.5%, 531/21 592) collected data in 1995, 1997 to 1999 and between 2005 and 2006. Colombia (1.9%, 407/21 592) reported results between 1992 and 2011. Bolivia (1.9%, 404/21 592) reported results between 2000 and 2011. Cuba reported results for 268 isolates between 1995–1998 and 2007–2011.9 ,13 In addition, 4528 N gonorrhoeae isolates were tested for penicillinase production between 1990 and 1997 in 13 Caribbean countries (n=32 Antigua, 232 Bahamas, 79 Barbados, 251 Belize, 26 Bermuda, 195 Cayman Islands, 20 Dominica, 42 Grenada, 77 Guyana, 93 St Lucia, 272 St. Vincent, 2960 Suriname, 249 Trinidad and Tobago).8 Trinidad (1992), Guyana (1994–1995) and St Vincent (1996) also reported on the susceptibilities of a total of 282 isolates to several antibiotics.11
Quality assurance among GASP-LAC members
Quality assurance programmes were competed during the 1990s8 and the 2000s.9 N gonorrhoeae WHO and Clinical Laboratory Standards Institute (CLSI) reference strains used for gonococcal susceptibility testing have been provided to all countries over the period8 ,9 ,14 including N gonorrhoeae WHO III, V and VII and ATCC 49226 (the only reference strain recommended by the CLSI).15 ,16 These strains have been consistently used by participants for MIC testing and some participants included inhouse pencillinase-producing N gonorrhoeae (PPNG) and isolates with plasmid mediated resistance to tetracyline [i.e. tetracycline resistant N. gonorrhoeae (TRNG), MIC≥16.0 mg/l] as controls as well.
Identification of N gonorrhoeae isolates and antimicrobial susceptibility testing
Results from periodic questionnaires sent to participants indicate that isolates in each country were confirmed to be N gonorrhoeae by a number of standard methods including Gram stain, oxidase test, carbohydrate utilisation tests and Gonogen II testing.8 ,9 Antimicrobial susceptibility testing methods included MIC determination by agar dilution and E test (bioMérieux, Saint Laurent, Quebec, Canada) as well as disk diffusion assays.8–13 Procedures according to CLSI and E test manufacturer's instructions were adopted.8 ,9 ,16 The medium used for antimicrobial susceptibility testing has consistently been GC Medium Base (GCMB) (Difco, Becton Dickinson, Franklin Lakes, New Jersey, USA) supplemented with 1% Kellogg's defined supplement (GCMBK) or IsoVitaleX (1%) (Becton Dickinson).8–13 For agar dilution MIC testing, GCMBK was supplemented with serial twofold dilutions of penicillin, tetracycline, ciprofloxacin, ceftriaxone, azithromycin or spectinomycin as described previously.8 ,9 ,16 Categorisation of antimicrobial susceptibility was based on CLSI criteria.16 Breakpoints for azithromycin were based on published criteria for resistance (MIC≥2 mg/L).9 ,17 For this summary, data from various countries were pooled from several periods8–13; different numbers of isolates were tested for each antibiotic (see figures). The Clopper-Pearson ‘exact’ method was used to calculate 95% CIs for antimicrobial susceptibility data.18
Results
Number of N gonorrhoeae isolates tested for antimicrobial susceptibility 1990–2011
Between 1990 and 1999, a total of 7856 N gonorrhoeae isolates were tested for antimicrobial susceptibility in countries in South America and the Caribbean while from 2000 onwards, 13 736 isolates were tested with numbers showing a slight increase from 2008 onwards (see figures) and fluctuated by country and year. For example, Argentina reported the susceptibilities of 15 isolates in 1990, 664 isolates in 2004 and 253 isolates in 2007 (data not shown). Several countries reported declining numbers of isolates tested in the 2000s including Brazil (from 655 isolates in 2001 to 120 in 2009), Bolivia (114 isolates in 2000; 13 in 2011) and Venezuela (176 isolates in 1990; 6 in 2011). By contrast, some countries such as Chile and Colombia reported a progressive increase in the number gonococcal isolates tested for antimicrobial susceptibility.9 Fifteen countries, notably in the Caribbean region, reported limited antimicrobial susceptibility information sporadically. Some countries have established national GASP networks (eg, Argentina, Chile) while others reported from single major urban areas (eg, Colombia, Venezuela).
Increases in MICs to ceftriaxone
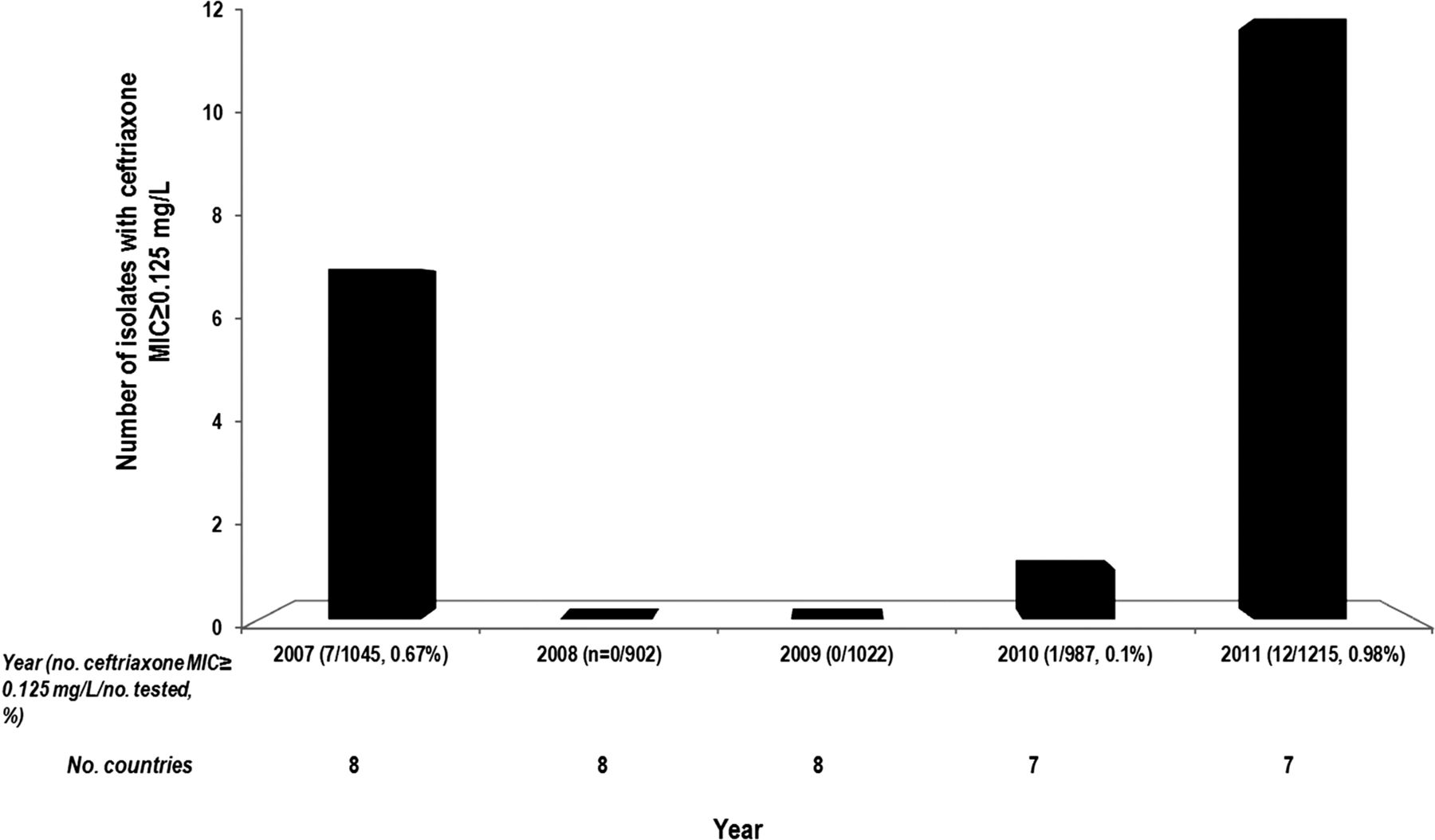
No isolate with reduced susceptibility to ceftriaxone was reported before 2006. Of 5171 N gonorrhoeae isolates tested for ceftriaxone susceptibility between 2007 and 2011, 20 (0.4%) were reported (Argentina, Brazil, Chile, Cuba and Uruguay) to have reduced susceptibility (MIC ≥ 0.125 mg/L) to ceftriaxone. In 2007, 0.7% (7/1045) of isolates tested displayed reduced susceptibility to ceftriaxone followed by 0.1% (1/987) in 2010 and 1.0% (12/1215) in 2011 (figure 1).

Minimum inhibitory concentration (MIC) increases to ceftriaxone. A total of 13 countries from South America and Cuba determined ceftriaxone susceptibility at different times. No isolate with a ceftriaxone MIC≥0.125 mg/L was reported before 2007. 20 isolates with decreased susceptibility to ceftriaxone were reported from four different countries in South America.
Ciprofloxacin and azithromycin resistance
Pooled data for the years 1990–2011 indicated that in the GASP-LAC region, ciprofloxacin resistance was 14.8% (1892/12 730) overall, ranging between 1.6% (2/127; 1997) and 42.1% (429/1019; 2010) of isolates tested (figure 2). Although no isolates were tested for ciprofloxacin susceptibility in 1990, it is notable that no ciprofloxacin resistance was reported between 1991 and 1994, in 1996 and from 1998 to 1999. Ciprofloxacin resistance remained below 5.0% of isolates tested until 2004. After 2006, resistance to ciprofloxacin continued to be greater than 15.0% of the isolates tested.

Trends of ciprofloxacin and azithromycin resistance in Neisseria gonorrhoeae isolates from Latin America: 1990–2011. A total of 13 countries reported on ciprofloxacin susceptibility over the period with different countries reporting for any given year. A total of 10 countries reported on azithromycin susceptibility. *Excludes 10/91 azithromycin resistant isolates from Cuba (1995–1998).13
The overall percentage (1992–2011) of N gonorrhoeae isolates resistant to azithromycin (figure 2) was 10.0% (1114/11 135) ranging from 1.0% (6/612; 2010) to 25.8% (191/739; 2008) of isolates tested. Azithromycin resistance remained above 6.0% of isolates tested between 2000 and 2009. No azithromycin resistance was detected between 1993 and 1999, except in Cuba where 10 azithromycin resistant isolates were reported between 1995 and 1998.
Susceptibility to penicillin
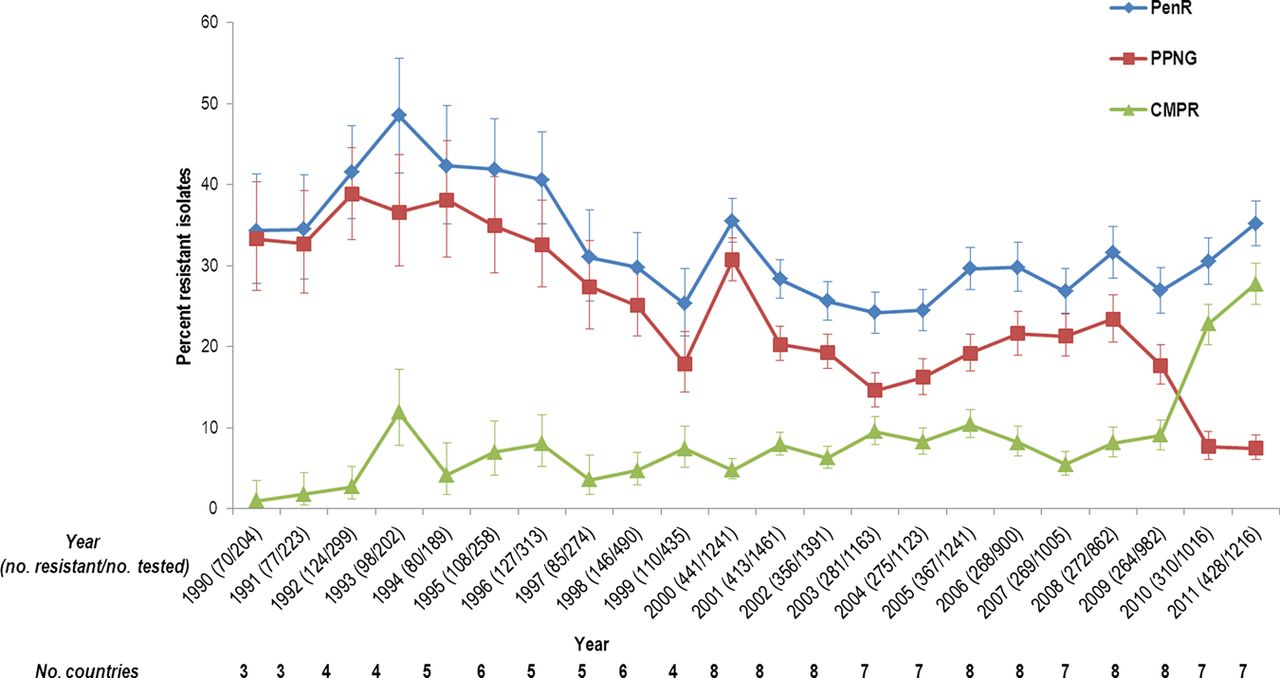
The prevalence of penicillin resistance in N gonorrhoeae isolates reported from the GASP-LAC network remained above 24.0% of isolates tested throughout the 1990 to 2011 surveillance period. Resistance to penicillin ranged between 24.2% (281/1163; 2003) and 48.5% (98/202; 1993) of isolates tested (figure 3). After 1993, overall penicillin resistance declined to 25.3% (110/435) of isolates tested in 1999. This percentage increased to 35.5% (441/1241) of isolates tested in 2000, decreased again between 2000 and 2003 to 24.2% (281/1163) of isolates tested in 2003, and increased to 35.2% (428/1216) in 2011.
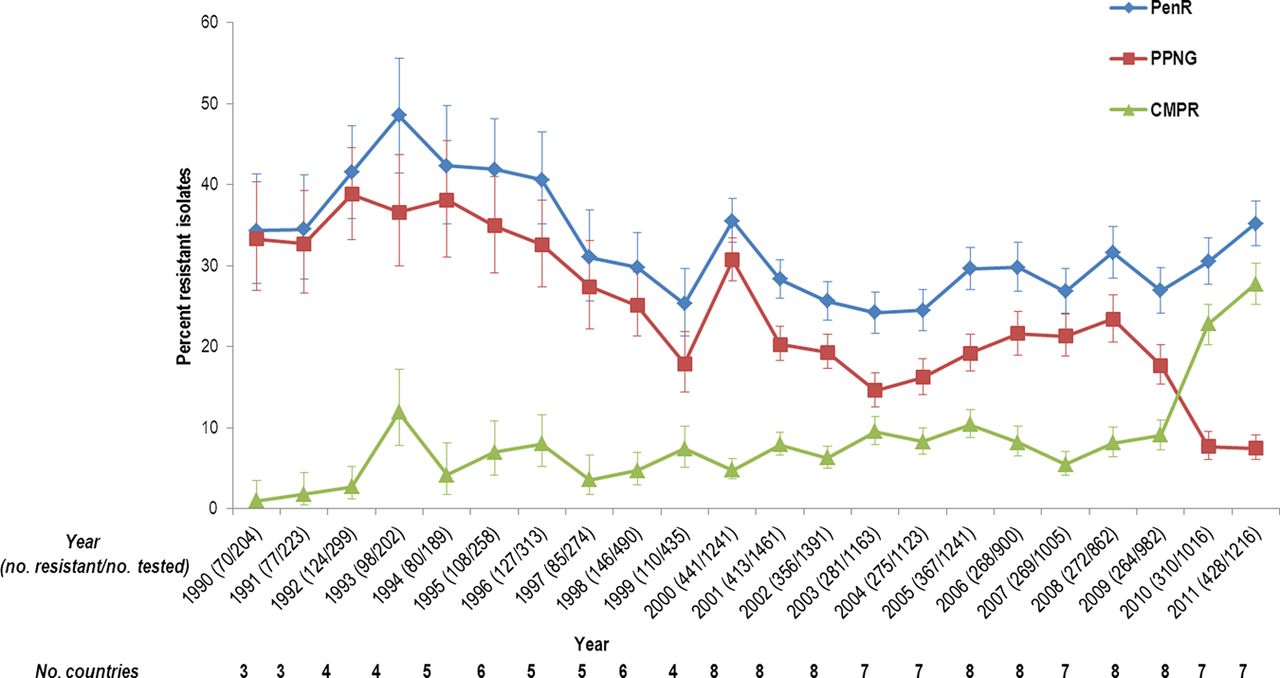
Trends of penicillin resistance in Neisseria gonorrhoeae isolates from Latin America: 1990–2011. Overall 35.28% of isolates tested were penicillin resistant (PenR); 27.6% were penicillinase-producing N gonorrhoeae (PPNG) isolates; and, 7.64% carried chromosomally-mediated penicillin resistance (CMPR). A total of 21 016 isolates were tested for susceptibility to penicillin. This data excludes sporadic information from Caribbean countries on PPNG (n=2445) reported over different small aggregated periods (1990–1997).8
From 1990 to 2009, the contribution of isolates with plasmid-mediated resistance to penicillin (ie, PPNG) to overall penicillin resistance was higher as compared with N gonorrhoeae isolates with chromosomally mediated penicillin resistance (CMPR, figure 3). PPNG prevalence remained above 7% throughout the surveillance period ranging between 7.5% (91/1216) of isolates tested in 2011 and 38.8% (116/29) of isolates tested in 1992. For the most part PPNG prevalence waxed and waned over the period with low percentages recorded in 1999 (17.9%, 78/435), 2003 (14.6%, 170/1163) and declining sharply from 2009 (17.8%, 174/982) to 2011 (7.5%; 91/1216). In contrast, a notable spike in PPNG percentages was noted in 2000 (30.7%, 381/1241).
The prevalence of CMPR isolates ranged between 1.0% (2/204; 1990) and 27.7% (337/1216; 2011) of isolates tested (figure 3). In 1993, CMPR isolates comprised 11.8% (24/202) of isolates tested, up from 1.0% (2/204) in 1990. Notably, aggregate CMPR numbers steeply increased in 2010 (22.8%, 232/1016) and 2011 (27.7%, 337/1216).
Susceptibility to tetracycline
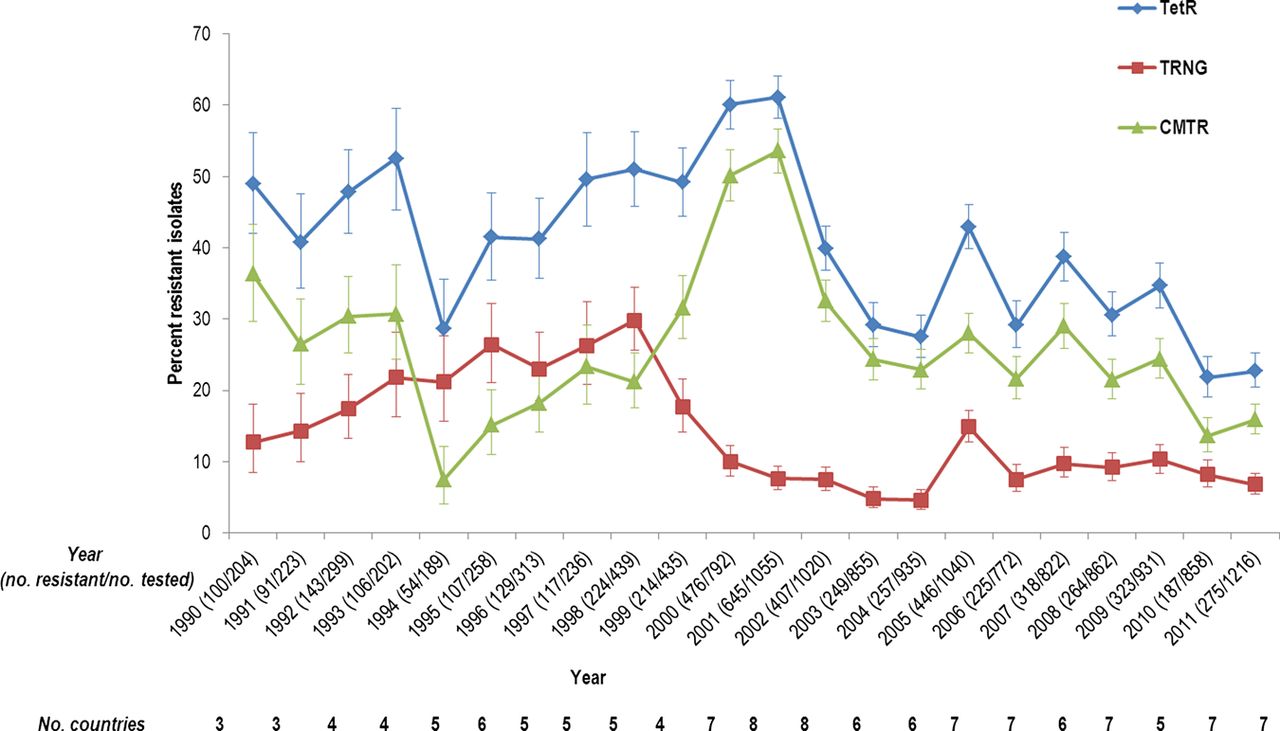
Tetracycline resistance overall varied between 21.8% (187/858; 2010) and 61.1% (645/1055; 2001) of N gonorrhoeae isolates tested between 1990 and 2011 with the overall percentage of resistant isolates remaining above 21% throughout the surveillance period (figure 4). After 1994, in which 28.6% of N gonorrhoeae isolates tested were tetracycline resistant (54/189), tetracycline resistance showed a steady increase with the highest levels of resistance reported in 2001 (61.1%; 645/1055; 2001). Thereafter, tetracycline resistance decreased overall with marked fluctuations. The prevalence of isolates which were TRNG ranged between 4.6% (43/935; 2004) and 29.8% (131/439; 1999) of isolates tested and remained above 4.5% throughout the surveillance period (figure 4). After 1998 (29.8%, 131/439), TRNG prevalence showed a decline to 4.6% of isolates tested in 2004, only to spike in 2005 (14.9%, 155/1040). Between 2006 and 2011, TRNG prevalence varied between 6.8% (83/1216, 2011) and 10.3% (96/931, 2009).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends of tetracycline resistance in Neisseria gonorrhoeae isolates from Latin America: 1990–2011. Overall, 38.4% (5358/13 956) of the isolates tested were tetracycline resistant (TetR); 11% carried plasmid mediated tetracycline resistance (TRNG, minimum inhibitory concentration ≥16 mg/L); and, 27.32% of the isolates carried chromosomally mediated tetracycline resistance (CMTR). Twelve different countries reported over the period.
From 1998 onwards, the contribution of isolates with chromosomal resistance to tetracycline (CMTR; figure 4) to overall tetracycline resistance was higher as compared with TRNG, ranging between 7.4% (14/189; 1994) and 53.6% (565/1055; 2001) of isolates tested. CMTR isolates displayed a sharp increase from 1994 (7.4%) to 2001 (56.3%) and then decreased progressively till 2004 (22.9%, 214/935). After 2004, reported CMTR prevalence fluctuated; in some years CIs overlapped (eg, 2003–2009) so that the minor changes observed may not be significant.
Discussion
The GASP network has been active in LAC for over two decades and has identified trends in emerging antimicrobial resistance in the region. The first reports on the emergence of low level and high level azithromycin resistance emerged from the GASP-LAC network.8 ,13 ,19 Notably, the aggregate percentage of azithromycin resistant isolates is somewhat higher than reported in other countries, although the dramatic and significant drop in azithromycin resistance in 2010–2011 remains unexplained.20 ,21 Isolates resistant to ciprofloxacin emerged only during the mid-2000s in the GASP-LAC region and have not reached the high percentages noted in some Asian countries and the Southern Pacific region.22 ,23 Nevertheless, levels of ciprofloxacin resistance are greater than 5% of isolates tested in most countries indicating that this antibiotic should not be used for treatment.7 ,9 Our recent analysis of treatment guidelines in many countries from Latin America indicates that this antibiotic is still recommended as front line treatment for gonococcal infections.9 Clearly action must be taken in a timely manner to link public health treatment policies for gonococcal infections in the region with the prevalence of resistant isolates.
The GASP-LAC network was also one of the first to note high levels of chromosomal resistance to penicillin and tetracycline, trends that are now emerging around the world.20–23 For example, the percentage of N gonorrhoeae isolates with chromosomal resistance to penicillin in the Western Pacific and South East Asia in 2010 was 13.4% of isolates tested ranging between 18.1% (New Zealand) and 39.2% (Japan).22 Similarly, an overall burden of 24% to 31% chromosomal penicillin resistance in N gonorrhoeae isolates between 2006 and 2008 was noted in European countries.20 The high percentages of PPNG isolates initially noted in the GASP-LAC during the 1990s are decreasing, as has been noted in other countries.21 ,24 ,25 For example, the prevalence of PPNG isolates in Canada decreased from 3.0% of isolates tested in 2000 to 0.9% in 2009.21 A decline in the prevalence of PPNG was recorded in USA from an annual peak of 11.0% in 1991 to 0.4% in 2007.24 PPNG prevalence in Korea also showed a drastic decrease from 64% in 2000 to 21% in 2006.25 It is thought that over-the-counter availability of antibiotics coupled with inadequate and inappropriate treatments may have contributed to the high percentages of penicillin (and tetracycline) resistant isolates in the GASP-LAC and other regions of the world.6 ,7 Interestingly, Brazil has recently banned the sale of over-the-counter antibiotics, an action which hopefully, will impact the development and maintenance of gonococcal antimicrobial resistance.
The last bullets in the single dose treatment arsenal for gonococcal infections are third generation cephalosporins. N gonorrhoeae isolates with treatment failures to this class of antibiotic and reduced susceptibility or resistance to cephalosporins have been reported worldwide.20 ,22–30 So far, reports of decreased susceptibility to these agents in Latin America have been sporadic.10 This result may reflect the lack of antimicrobial susceptibility testing of an appropriate number of isolates to these agents in many countries. Alternatively, since treatment with cephalosporins has not been universally adopted in the region, the lack of isolates with reduced susceptibility may offer some time before resistance develops in response to steady selective pressure.
The call for a global action plan to control the spread and impact of antimicrobial resistance in N gonorrhoeae isolates is urgent.7 In order to achieve this goal in the GASP-LAC network several important issues must be resolved. The network has faced complicated challenges in being sustainable. One of these challenges includes sufficient financial support to perform the tasks required at all levels of public health surveillance.7 A possible indirect cost of the widespread adoption of syndromic management of gonococcal infections in many countries in LAC is decreased laboratory capacity as well as diminished capability in obtaining the clinical specimens required to test gonococcal antimicrobial susceptibility.3 ,4 Consequently, renewed efforts are underway to retrain laboratorians and clinical practitioners in relevant methods. Interestingly, no laboratory has reported the use of nucleic acid amplification testing in South America and the Caribbean for the identification of N gonorrhoeae isolates. Thus, the issues arising from the use of these tests, namely the potential unavailability of cultured isolates of N gonorrhoeae for antimicrobial susceptibility testing, does not appear to be a concern at the present time.7
This synopsis presents a number of challenges and limitations which really reflect challenges to the comprehensive global call for action. For one thing, the number of countries able to fully or partially participate in surveillance has continually changed over the period reflecting changing capability and capacity. Interestingly, contacts were not lost over the period; rather, the inability to participate in the GASP-LAC reflects a true loss in laboratory based testing capability and requires a refurbishment of laboratory infrastructure. A sustained and not intermittent quality assurance programme for the region must be maintained and the cost of such a continuous programme has been a major challenge in the past. The periodicity and extent of testing within and between countries varies and might be standardised. Also, there is no capacity, at present, to collect enhanced epidemiological and clinical information, verified treatment failures, etc and to link such information to laboratory based observations. Lastly, there is a need to develop standard protocols for the collection of strains and to develop a comprehensive laboratory backup system to confirm reports of resistant isolates, particularly to third generation cephalosporins.
Often appropriate antibiotics are not available or are too expensive for laboratory based GASP testing. This situation could be resolved through the advocacy of international health agencies. The collection and analysis of susceptibility data must become more proactive; the GASP-LAC is moving from periodic analysis of retrospective data to the yearly collection, analysis and appropriate communication of data. Such information must be effectively used to inform national public health strategies and policies, especially the timely review and revision of treatment guidelines.9 Finally, the capacity to understand the dynamics of the transmission of antibiotic resistant N gonorrhoeae strains and emerging mechanisms of resistance, through the molecular analysis of gonococcal strains and populations, has diminished since the 1990s as laboratory capacity has decreased. Such studies are vital to better comprehend what strains should be targeted for control measures.
Key messages
-
The number of countries participating in the Gonococcal Antimicrobial Susceptibility Surveillance Program for Latin America and the Caribbean (GASP–LAC) has steadily declined since the 1990s due to a loss of laboratory capability.
-
Most countries in the region reported a high prevalence of isolates resistant to ciprofloxacin with sporadic reports of reduced susceptibility to ceftriaxone.
-
Treatment guidelines in some countries often do not reflect the prevalence of resistant gonococcal isolates indicating a need for their regular, evidence-based revision.
References
Footnotes
-
Handling editor Jackie A Cassell
-
Acknowledgements The authors gratefully acknowledge the contributions of individual former and present GASP-LAC members: Susana Fiorito, Patricia Galarza and GASP Argentina (Centro Nacional de Referencia en ITS INEI-ANLIS ‘Dr Carlos G Malbran’, Buenos Aires, Argentina); Maria Elena Trigoso Carvallo (Centro Departamental de Vigilancia, Información Referencia, La Paz, Bolivia); Adele Schwartz Benzaken and GASP Brazil (Fundcao Alfredo da Matta, Manaus—Amazonas, Brazil); Valdir Monteiro Pinto (Division STD Control, Hepatitis and Aids Departamiento National ITS/SIDA, Brasilia, Brasil, Current address STD/AIDS State Program—Sao Paulo, Brazil); Pamela Araya, Aurora Maldonado (Instituto de Salud Publica de Chile, Santiago, Chile); Clara Ines Agudelo, Olga Marina Sanabria, Maria Elena Realpe (Instituto Nacional de Salud, Bogota, Colombia); Alina Llop Hernandez, Rafael Llanes and GASP Cuba (Instituto de Medicina Tropical ‘Pedro Kourı’, Ministerio Salud Publica, Habana, Cuba); Eduardo Aguilar Jarrin (Ministerio de Salud Publica del Ecuador, Quito, Ecuador); Nicolas Aguayo (Ministerio de Salud de Paraguay, Asuncion, Paraguay); Jose Luis Portilla (Instituto Nacional de Salud, Lima, Peru); Parimi Prabhakar and the Caribbean GASP Network (Caribbean Epidemiology Centre, CAREC, Port of Spain, Trinidad and Tobago); Graciela Borthagaray, Ana Acevedo, Carolina Marquez (Facultad de Quimica, Universidad de la Republica, Montevideo, Uruguay); Daisy Payares, Lilia Leon (Instituto Nacional de Higiene ‘Rafael Rangel,’ Caracas, Venezuela).8–13 The authors are also grateful to Aura Helena Corredor for her assistance in preparing this manuscript and Dr Cheryl Waldner (College of Veterinary Medicine, University of Saskatchewan) for her advice on statistical methods. We gratefully acknowledge funding from the Public Health Agency of Canada (contract no. 4500294744) for supporting the preparation of this paper. We also acknowledge the University of Saskatchewan (grant to J-ARD) and the Saskatchewan Health Research Foundation (Grant # 9127, the Research Alliance for the Prevention of Infectious Disease) for their support of this research.
-
Collaborators GASP-LAC members: Susana Fiorito, Patricia Galarza and GASP Argentina (Centro Nacional de Referencia en ITS INEI-ANLIS ‘Dr Carlos G Malbran’, Buenos Aires, Argentina); Maria Elena Trigoso Carvallo (Centro Departamental de Vigilancia, Información Referencia, La Paz, Bolivia); Adele Schwartz Benzaken and GASP Brazil (Fundcao Alfredo da Matta, Manaus—Amazonas, Brazil); Valdir Monteiro Pinto (Division STD Control, Hepatitis and Aids Departamiento National ITS/SIDA, Brasilia, Brasil, Current address STD/AIDS State Program—Sao Paulo, Brazil); Pamela Araya, Aurora Maldonado (Instituto de Salud Publica de Chile, Santiago, Chile); Clara Ines Agudelo, Olga Marina Sanabria, Maria Elena Realpe (Instituto Nacional de Salud, Bogota, Colombia); Alina Llop Hernandez, Rafael Llanes and GASP Cuba (Instituto de Medicina Tropical ‘Pedro Kouri’, Ministerio Salud Publica, Habana, Cuba); Eduardo Aguilar Jarrin (Ministerio de Salud Publica del Ecuador, Quito, Ecuador); Nicolas Aguayo (Ministerio de Salud de Paraguay, Asuncion, Paraguay); Jose Luis Portilla (Instituto Nacional de Salud, Lima, Peru); Parimi Prabhakar and the Caribbean GASP Network (Caribbean Epidemiology Centre, CAREC, Port of Spain, Trinidad and Tobago); Graciela Borthagaray, Ana Acevedo, Carolina Marquez (Facultad de Quimica, Universidad de la Republica, Montevideo, Uruguay); Daisy Payares, Lilia Leon (Instituto Nacional de Higiene ‘Rafael Rangel,’ Caracas, Venezuela).
-
Contributors J-ARD cowrote and edited each draft and is project leader responsible for liaison with each country in Latin America and data collection, analysis and communication of results. SDT compiled and performed data analysis, wrote the first draft and edited subsequent drafts; MT performed statistical analysis of the data.
-
Funding Public Health Agency of Canada (contract no. 4500294744) and Saskatchewan Health Research Foundation (Grant # 9127, the Research Alliance for the Prevention of Infectious Disease) and the University of Saskatchewan.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.