Article Text

Abstract
Objectives: To determine whether the risk factors associated with bacterial vaginosis (BV) are consistent with it being a sexually transmitted infection (STI) by comparing the characteristics of women with BV with those of women with infections recognised as being sexually and non-sexually transmitted.
Methods: A prospective cross sectional study was conducted among female patients presenting for diagnosis at a genitourinary medicine clinic in Sheffield between January 1996 and September 1998. Demographic and behavioural characteristics were reported from patient records and a standardised questionnaire was administered. Risk factor models for BV, two STIs, and two non-STIs were compiled using a multivariable logistic regression analysis.
Results: Among the 8989 females under 45 years eligible for analysis, the prevalence of BV was 12.9%. Risk factors associated with BV included some in common with gonorrhoea and Chlamydia trachomatis and some that were not associated with these two STIs. Risk factors common to BV and the STIs included having had more than one sexual partner in the past 3 months, having a history of a bacterial STI, being of black Caribbean ethnicity, and living in a deprived area. However, BV had a contrasting age profile, being most prevalent among those over the age of 30. BV was also more common in those who were divorced.
Conclusions: BV is associated with some factors related to the acquisition of gonorrhoea and Chlamydia trachomatis. However, infection is not only determined by those factors and therefore factors other than sexual activity may be important in the development of the condition.
- bacterial vaginosis
- sexually transmitted infections
Statistics from Altmetric.com
Introduction
Bacterial vaginosis (BV) is a common cause of abnormal vaginal discharge in women of reproductive age.1 It is a polymicrobial syndrome involving the replacement of the normal vaginal lactobacilli by a variety of anaerobic bacteria and mycoplasmas.2 The rate of BV varies according to the population studied and the geographic location, with recorded prevalences ranging from 4% in university students to 33% in GUM clinics.1 BV is also thought to be the cause of substantial reproductive morbidity.3 It is associated with premature birth, and links to upper genital tract infection and infertility have now been suggested.4–7 Prospective studies have strengthened evidence for a causal link between BV and HIV-1 acquisition.8 BV is more common than other STIs associated with enhancing HIV transmission increasing the population attributable risk. Such an association makes further research into the aetiology, treatment, and prevention of BV a public health priority.
It is still uncertain whether BV is a sexually transmitted infection (STI). The syndrome was first described as “Haemophilus vaginalis vaginitis” in 1955 by Gardner and Dukes. They concluded that it was an STI as the isolated aetiological agent, H vaginalis (now renamed Gardnerella vaginalis), was found in the male contacts of the female cases.9 However, Leopold had previously described a Gram negative non-motile rod isolated from men and women with symptoms characteristic of BV and it is now known that Gardnerella vaginalis occurs in up to 50% of women without BV.10 Further research has implicated a wide range of other micro-organisms, including Prevotella spp, Mycoplasma hominis, and Mobiluncus spp, in the syndrome.2
Very few risk factor studies for BV have taken place in the United Kingdom and most have used ill defined case definitions across heterogeneous populations, producing inconsistent results. In this study we describe the demographic and behavioural characteristics of women diagnosed with BV within a large population attending a genitourinary medicine (GUM) clinic. Although GUM clinic attendees are not a representative sample of the general population, they allow a large and complete data set of clinical and behavioural outcomes to be collected and for comparisons to be made with attendees with infections that are clearly sexually transmitted. The aim was to determine whether BV was likely to be sexually transmitted by comparing the characteristics of women with BV with those of women with established STIs and to those of women without an STI diagnosis.
Methods
Since 1993, limited demographic and behavioural data have been collected from all consenting GUM clinic attendees at the Royal Hallamshire Hospital in Sheffield. This study analysed data from female patients attending between January 1996 and September 1998 (inclusive). Data from all females aged under 45 were analysed as the major burden of ill health associated with BV is for women of reproductive age. Diagnostic, demographic, and behavioural data for the first attendance with BV within a calendar year were investigated in risk factor analyses. Reattendance in a later year was taken as a new patient attendance. It is not unreasonable to presume that those reattending with BV over the study period would differ from those with a single attendance. Therefore, reattendance with BV at any point over the study period was used to investigate risk factors for reattenders in a separate analysis.
DATA COLLECTION
Data on the date of attendance, diagnosis, and demographic characteristics were collected and analysed. Behavioural characteristics were determined through a short behavioural questionnaire delivered by the doctor at each patient visit, on sexual behaviour including sexual preference, the number of partners in the past 3 and 12 months, a history of an STI, a history of high risk sexual partners, and sexual experience abroad. Data on smoking and contraceptive use were not available. Data were wholly anonymised.
Postcode data were used as a proxy for socioeconomic status. Postcodes were linked to the local health authority ward using the post office address file database. The local health authority ward was then described as deprived, industrial, mixed urban/rural and prosperous according to the Office for National Statistics (ONS) group and cluster classification.
MEDICAL AND LABORATORY DATA
Diagnosis of BV in the clinic was based on Amsel's criteria requiring three or more of the following clinical/diagnostic features11:
-
The presence of (excessive) homogeneous vaginal discharge
-
Elevated vaginal pH greater than or equal to 5.0
-
Positive amine test
-
20% “clue cells” (vaginal epithelial cells adhered to by infective microbes) and typical Gram stain appearance upon microscopy of vaginal secretions including absence of lactobacilli.
The diagnosis of BV was made as part of routine patient assessment by all the clinicians working in the department. All medical and nursing staff had undergone training for their clinical and laboratory work and were subject to quality control procedures with regard to microscopic diagnosis.
STATISTICAL ANALYSIS
All analyses were undertaken using stata and glim software. The first attendance data were analysed using logistic regression and the reattendance data were analysed using proportional hazards regression analysis for survival data.
In the logistic regression analysis the presence of BV (KC60 code C6B) was taken as the dependent variable. A single variable analysis was performed and factors which were significant at p<0.1 were included in the multivariable logistic regression analysis (analysis of log likelihood). A p value of less than 0.05 for each variable was then regarded as statistically significant. For the final model all two way interactions between variables were investigated. The baselines chosen reflected the largest group within a variable except for age and postcode. As BV is most common among older women, while STIs are more common in the under 20s, a baseline of 20–24 was chosen to highlight both phenomenon.12, 13 A postcode description of “living in a prosperous area” was chosen as the baseline to highlight any trend of increasing prevalence with deprivation that is often common with disease.13
The final model for BV was compared with risk models compiled using the same data and methodology for two known STIs, gonorrhoea (KC60 code B1B2) and Chlamydia trachomatis (C4AC4C), and for conditions not believed to be primarily sexually transmitted, candida (KC60 code C7A) and “other conditions” requiring treatment at a GUM clinic (KC60 code D2B). To allow for direct comparison, risk factor models were run for each condition containing all the variables that had proved significant in any one individual model.
Reattendance with BV was examined in the subset of patients who had attended with BV at some point during the study period. Factors related to a reattendance with BV were analysed in the survival analysis. Follow up was considered truncated in September 1998 and time to reattendance was measured in months. Before running the model it was confirmed that all variables conformed to the assumptions of the proportional hazards model. For the survival analysis the black African and Asian ethnic groups were combined as the numbers in each group were very small. As the two amalgamated ethnic groups had almost identical survival curves it was felt that no unique information would be lost through their combination. The amalgamation of the few cases of BV within each group gave a more robust analysis.
Results
FIRST ATTENDANCE ANALYSIS
After patient loss for ineligibility 8989 female patients under 45 remained in the study. The general characteristics recorded for the first attendance of a patient within a calendar year at the Royal Hallamshire GUM clinic between January 1996 and September 1998 are presented in table 1. In all, 90.6% were white and 4.6% were black Caribbeans; 15.2% were aged under 20 and 92.9% were heterosexual leaving 7.1% homosexual or bisexual. A third of all patients had previously presented at a GUM clinic with an STI. Only 16.1% had had more than one partner in the 3 months before their attendance.
Characteristics of patients at their first attendance within a calendar year at the Royal Hallamshire GUM clinic, January 1996–September 1998
Of the 8989 patients attending during the study period, 1161 (12.9%) presented with BV. Adjusted odds ratios for the final multivariable model are shown in table 2. The initial single variable analysis showed age, source of referral, marital status, ethnicity, postcode, more than one sexual partner in the past 3 months, concurrent infections, a history of a bacterial STI, a partner with an STI, an injecting drug using partner, ever having had a homosexual or bisexual partner, and sexual preference to be significant at the 10% level. A less stringent level of significance was chosen for the initial analysis to include as many variables in the multivariable analysis as possible to ensure the best fitting model.
Adjusted risk factors for BV, gonorrhoea, Chlamydia trachomatis, and other conditions requiring treatment at a GUM clinic (for first attendance in a calendar year):
Initial investigations found significant interactions between year and chlamydial infection as well as year and herpes. The latter was an artefact of the small number of herpes cases. As the interaction between chlamydial infection and year was thought to be due to increased testing, given the recent interest expressed in Chlamydia trachomatis and newly developed diagnostics, it was not included in the final multivariable model.14
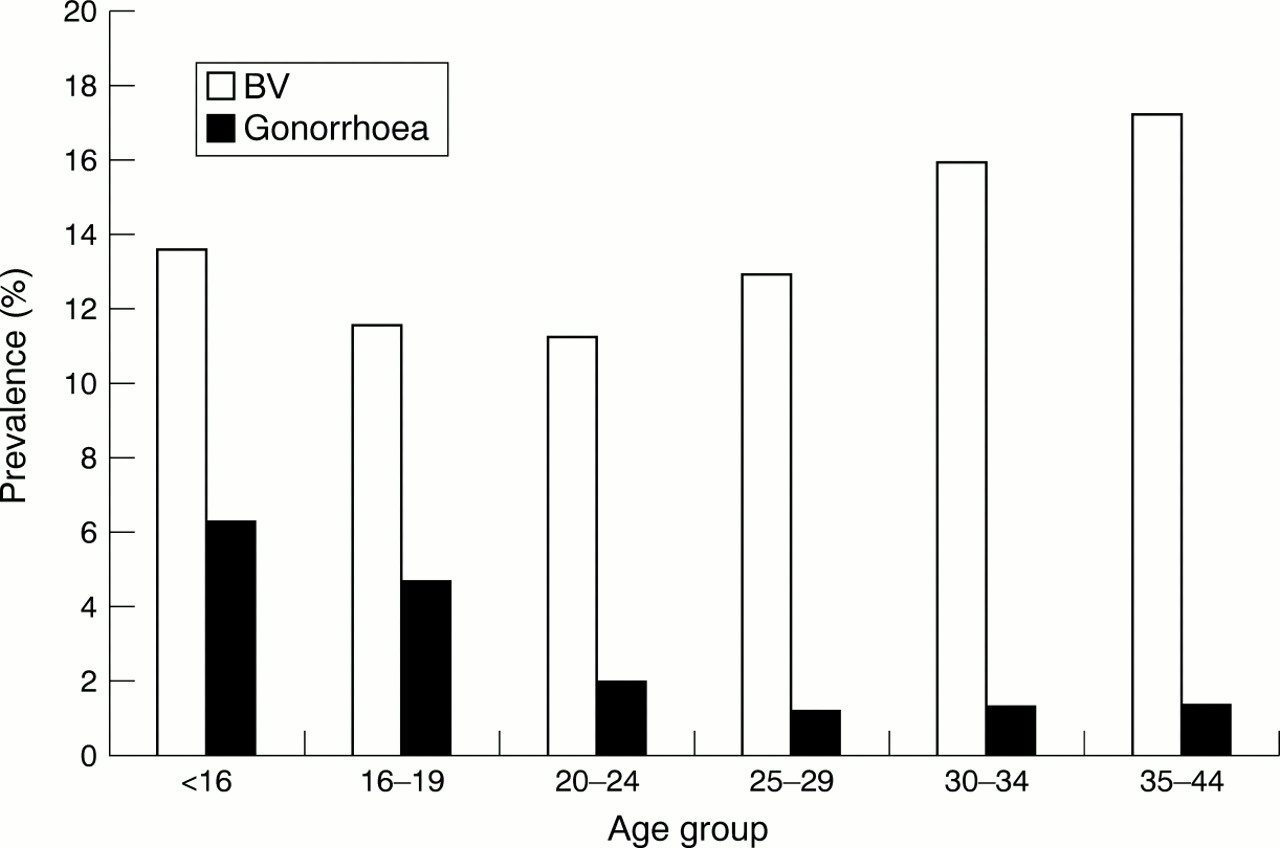
BV was more prevalent among the 35–44 year olds than the 20–24 year olds (Fig 1) and among those of black Caribbean than those of white ethnicity. BV was more common among those living in a deprived area compared with a prosperous area, among those with two sexual partners rather than one or no partners in the past 3 months, and among those with a history of a bacterial STI. Although BV was more prevalent among homosexual than among heterosexual patients (15.7% v 12.7%), the difference proved non-significant in the multivariable analysis. Patients with BV were more likely to attend with a concurrent gonorrhoea infection, but less likely to attend with concurrent trichomoniasis, warts, herpes, or candida.
{kind=link}
Age specific prevalence of BV and gonorrhoea in a Sheffield GUM clinic 1996–8.
Adjusted risk factors for the gonorrhoea, Chlamydia trachomatis, and non-sexually transmitted conditions seen at GUM clinics are also shown in table 2. Both BV and Chlamydia trachomatis were more prevalent among black Caribbeans compared with whites and among women who were divorced, separated, or widowed compared with those who were single. Both BV and gonorrhoea were more common in deprived areas. BV, gonorrhoea and Chlamydia trachomatis were most prevalent among women with two partners in the past 3 months compared with none or one partner. Those in the “other condition” category were significantly less likely to report two partners compared with no or one partner. Those with BV, gonorrhoea, and Chlamydia trachomatis were more likely to have a history of a bacterial STI.
Gonorrhoea and Chlamydia trachomatis were most common among teenagers. Only those in the “other treatment” group followed the pattern of BV, where the risk was greatest in the 35–44 age group. Patients with gonorrhoea and Chlamydia trachomatis were much more likely to have had a sexual contact with a partner with an STI. Those with candida and in the “other treatment” group were less likely to have had contact with a partner with an STI.
There were few significant results from the candida model. There were no direct similarities to the results for BV or the STIs. Because of this the results are not presented in table 2.
REATTENDER ANALYSIS
One hundred and five patients out of the 1280 presenting with BV had more than one diagnosis of BV within the study period. The proportional hazards assumptions held for all variables and the single variable analysis proved significant for ethnicity, postcode, numbers of partners in the past 4–12 months, a history of an STI, a partner with a STI, having a concurrent infection with trichomoniasis and warts, and being a commercial sex worker. There were no significant two way interactions.
The results for a multivariable survival analysis to investigate the risk factors associated with a reattendance for BV for these 1280 patients are shown in table 3. Time to reattendance with BV was shorter for black Caribbeans and those of mixed/other ethnicity compared with those of white ethnicity. The likelihood of reattendance increased with the number of sexual partners in the past 4–12 months and peaked in those with three or more partners. Finally, those with a history of a bacterial STI had a shorter time to reattendance.
Adjusted risk factors for reattenders with BV
Discussion
The prevalence of BV within the study population was 12.9%. This is consistent with data from UK antenatal populations and is lower than one would expect from a GUM clinic population when previous studies have reported figures of up to 33%.4, 12, 15, 16 However, most GUM clinic studies were based in the United States and Scandinavia and it is possible that the results are not applicable in the United Kingdom. Another UK study set in a west London GUM clinic reported a prevalence of BV of only 9.6%.17 The low prevalence could reflect certain characteristics of the present study population. Over 90% of the population were white with very few patients representing black ethnic minorities known to have higher rates of BV. In addition, only 16% of the study population had had more than one sexual partner in the past 3 months, representing a population with lower risk sexual behaviour than those investigated in the studies yielding higher prevalences of BV. Alternatively, diagnostic differences may have led to differing results. This study used a pH cutoff point for BV of greater than or equal to 5.0 rather than pH 4.5 used elsewhere. This higher cutoff may have excluded some cases and lowered the prevalence. However, as a more sensitive microscopy technique was also in use this should have been avoided.
A common risk factor profile for a sexually transmitted infection (STI) includes having higher numbers of sexual partners, higher rates of partner change, a lower age of first intercourse, and being aged under 25.13 Previous studies have reported that the prevalence of BV also rises with the number of lifetime sexual partners and is more common in those with a lower age of first intercourse.18 In this study the risk of BV was greatest among those reporting more than one partner in the past 3 months reflecting the pattern reported for the known STIs, gonorrhoea, and Chlamydia trachomatis. This suggests that a diagnosis of BV is associated with a recent partner change. It is possible that BV is favoured by certain vaginal physiological changes induced through a new sexual partnership.19 Alternatively, as short term sexual history was of greatest importance, having a new sexual partner may prompt that patient to seek treatment for symptoms.
However, BV and “other non-sexually transmitted conditions” exhibited an age profile in direct contrast with the known STIs. Both showed prevalences peaking in the over 30s when one would expect lower rates of sexual partner change than in younger adults. It is hard to interpret the age data given the limitations of our knowledge of the aetiology of BV. Little is known about the incubation time of BV, but recurrences are common. It is possible that the women became infected at an earlier time and suffer persistent vaginal abnormalities.
There was no association between BV and having a partner infected with an STI, but this non-specific category provides little information on possible routes of infection for BV especially as there is no direct male equivalent of BV. There were no data on the concordance of BV infection in lesbian parternships that would have allowed the passage of infection to be investigated. However, past studies focusing on concordant BV infections within lesbian couples have failed produce consistent results.20, 21
The risk of BV was greatest among black Caribbean women, supporting findings from previous UK and US studies of antenatal populations.4, 22 Those studies were disadvantaged by failing to consider socioeconomic status as a possible confounder in the unequal distribution of BV across ethnic group. By using postcode to obtain a proxy for socioeconomic status, this study suggests that ethnicity is an independent risk factor. However, one should be cautious when interpreting the data as postcode is only a crude proxy.
Certain sexual practices, such as douching, are known to be more common among African-American women in the US and African-Caribbean women in the United Kingdom.23, 24 A recent study of an urban population in Seattle found that douching was linked to the practice of “dry intercourse” which is known to increase the risk of bacterial lower genital infection.25 A UK case control study within an inner city GUM clinic has now reported douching to be an independent risk factor for BV. Once vaginal douching was adjusted for in the analysis there was no ethnic difference in the occurrence of BV (adjusted OR 1.1; 95% CI 0.5–2.5).26 The role of vaginal cleaning practices in the development of BV needs to be investigated further.
BV is more prevalent in lesbians; 33% of lesbians were infected compared with 13% of heterosexuals in a recent study at an inner London GUM clinic. Lesbians usually have lower rates of STIs and this fact together with studies that have found BV in virgins indicate that specific practices, and not sexual intercourse with an infected partner, spread BV.27
The ethnic profile of women attending with BV was very similar to that for women attending with gonorrhoea.17 Twelve per cent of women attending with BV had a history of gonorrhoea. It is possible that those women were attending the clinic for what they believed to be the recurrence of a previous gonococcal infection introducing some bias in the ethnic profile of women presenting with BV. However, given the strength of the association between BV and black Caribbean ethnicity, the data are likely to reflect a true relation and not simply model the association between gonorrhoea and ethnicity
Those with a history of a bacterial STI (gonorrhoea or Chlamydia trachomatis) were at a greater risk of BV. The relation between high risk sexual behaviour and a history of a bacterial STI is well documented, though having previously experienced the symptoms of STIs may make patients more aware of vaginal abnormalities and therefore more likely to attend the GUM clinic.
The association between BV and other genital tract infections may reflect biological interactions in the vaginal microflora rather than common risk factors for their acquisition. Those presenting with BV were more likely to have a concurrent infection with bacterial gonorrhoea, but less likely to be diagnosed with a protozoal, viral, or fungal infection. An inhibitory effect of the bacterial amines, putrescine and cadaverine, on the cell division and germ tube formation of Candida albicans has recently been reported.28 Such bacterial amines are produced by anaerobes characteristic of the BV microflora. The negative correlation between BV and candida is likely to be due to inhibitory effect of bacterial amines. Mycoplasmas, often a common feature of BV flora, are known to colonise less frequently in the presence of fungal candida, but are found with a raised incidence in women infected with Neisseria gonorrhoeae and Chlamydia trachomatis.29
Synergistic relations between different BV associated organisms have now been demonstrated: M hominis and G vaginalis prevalences are known to increase following an increased prevalence of various anaerobes. The stimulation of G vaginalis growth has been observed with the production of amino acids by anaerobes and ammonia by P bivia.30
The study does have several limitations. The study population is not broadly representative, but a GUM clinic does give access to large numbers of accurately diagnosed cases of BV. Although, information on a wide range of behavioural risk factors was collected there was no data on smoking and contraceptive use (particularly intrauterine device use), both documented risk factors for BV. The use of postcode to gain a proxy for socioeconomic status was a crude measure and should be interpreted with caution. A better approach may have been to identify the electoral ward for each postcode and to interpret it using small area statistics measures of social deprivation, such as Jarman or Townsend scores.
BV is related to sexual activity, though it is hard to confirm that its development is entirely determined by those variables. BV could be a marker of specific sexual practices or may be related to changing biological mechanisms that mean that a woman's susceptibility increases with age. The epidemiological picture of BV is likely to be complex and can only be revealed through more detailed behavioural studies considering the specific sexual and contraceptive practices of high risk groups. Only when the transmission dynamics of infection are properly understood can interventions be designed that will effectively reduce the burden of morbidity.
Acknowledgments
We thank the staff of the GUM department of the Royal Hallamshire hospital for their work in collecting the data. We also thank Gwenda Hughes for her help with the preparation of the dataset and Dr Mike Catchpole, Dr Angus Nicoll, and Professor David Taylor Robinson for their invaluable comments on previous versions of this paper.
Funding: No external funding.
Conflict of interest: None.
Contributors: MM analysed the data and wrote the main body of the paper; PR supervised the data analysis and commented on previous drafts of this paper; GK is the consultant of the GUM clinic at the Royal Hallamshire Hospital. It was under his guidance and supervision that the sentinel survey was established and that the data for this study were collected. He also commented on previous drafts of this paper.