Article Text

Abstract
Background: Polymerase chain reaction (PCR) has well established advantages over culture for diagnosis of herpes viruses, but its technical complexity has limited its widespread application. However, recent methodological advances have rendered PCR more applicable to routine practice.
Aim: To compare automated PCR with viral culture for diagnosis of genital herpes.
Methods: We studied 236 patients presenting with clinical features suggestive of genital herpes at an inner city genitourinary medicine clinic. Two swabs were taken from each patient. Cell culture and typing were performed by standard methods. Automated PCR was performed using the LightCycler instrument and the infecting viral type was determined by restriction endonuclease digestion of amplicons.
Results: 109 patients (46%) had a positive test for herpes simplex virus (HSV). In 88, both PCR and culture were positive; in 21 PCR only was positive. With both detection methods, lesion duration and morphology were associated with HSV detection. Compared with culture alone, use of PCR increased sensitivity by 13.3% in specimens from vesicular lesions, by 27.4% from ulcerative lesions, and by 20.0% from crusting lesions.
Conclusions: We advocate adoption of automated PCR as an efficient HSV detection and typing method for diagnosis of genital herpes in routine clinical practice. PCR allowed rapid laboratory confirmation of the diagnosis and increased the overall HSV detection rate by 24%.
- herpes genitalis
- herpes simplex virus
- laboratory techniques
Statistics from Altmetric.com
Genital herpes simplex virus (HSV) infection is a major public health issue, with substantial morbidity and transmission potential. Infection is predominantly subclinical and individuals with unrecognised infection account for the majority of new transmission episodes to susceptible partners.1 There is a need for better diagnostic methods to identify individuals with minimally symptomatic disease.
The current standard diagnostic test is virus culture, used by 97% of UK genitourinary medicine (GUM) clinics.2 However, it is slow and labour intensive. Application of polymerase chain reaction (PCR) offers rapid, sensitive, and specific identification of HSV, but has hitherto been difficult to apply to routine clinical practice because of its technical requirements. However, introduction of the LightCycler (Biogene) has rendered PCR feasible on a larger scale and potentially applicable to routine clinical healthcare practice. Real time PCR protocols employ the incorporation of dyes or the binding of probes during each cycle of the PCR so that accumulation of product can be measured while the reaction is proceeding. LightCycler is one such method.3 Real time PCR protocols are not truly automated, although there is now the capacity to load the reaction capillaries in the same machine as that in which the extraction is performed. In our assay, although automated extraction is performed using a Qiagen BioRobot, the capillaries are loaded manually. A benefit of light cycling is that the readout is electronic so gels do not have to be run.
We conducted a study to investigate the feasibility of using this technology in a laboratory serving a large, UK GUM clinic and to compare the diagnostic performance of PCR with that of viral culture in patients presenting with clinical lesions suggestive of genital herpes.
METHODS
Patients and specimen transport
After obtaining local ethics committee approval, all patients with clinical features suggestive of genital herpes who attended the GUM department at Glasgow Royal Infirmary between 13 November 1998 and 7 May 1999 were invited to participate in the study. No patients declined. Two swabs were taken from each patient, in a pre-randomised order, each placed in either standard viral transport medium (VTM) or in lysis buffer (LB) (6M guanidine-HCl, 10 mM urea, 10 mM TRIS-HCl, 20% Triton X-100 (v/v), pH 4.4 (25°C). Clinical data were recorded on duration of genital skin lesions, past history of HSV infection, use of antiviral therapy before sampling, severity of symptoms, and lesional type. Lesional type was categorised into vesicle, ulcer, or crusting lesion; specimens taken from more than one lesional type were categorised into the earliest lesional stage recorded by the attending physician (for example, patients with vesicles and ulcers were defined as being at the vesicular stage).
Virus culture and typing
For culture, 200 μl of the VTM specimen were inoculated into one each of tubes containing a monolayer of MRC-5 HEL cells and Vero monkey kidney cells. The tubes were incubated at 37°C until a cytopathic effect was observed or considered negative at the end of 10 days. In tubes where a cytopathic effect was considered positive for HSV, the cells were scraped off the tube, dried onto a slide, and fixed. These were then confirmed and typed using monoclonal FITC conjugated antibody stains (PathoDx Herpes Typing, Diagnostic Products Corporation, Los Angeles, CA, USA). All clinical material was maintained in culture for 10 days, before a negative result was reported.
PCR and typing
PCR was performed on both specimens from each patient (that is, those transported in LB and those transported in VTM). Extraction followed the standard protocol of the Roche Molecular Biochemicals High Pure Viral Nucleic Acid Kit (Roche Diagnostics Ltd, Lewes, UK).
PCR was carried out using a LightCycler, LC32 (Idaho Technologies). For the reaction, 2.5 μl of extracted DNA were added to 7.5 μl of PCR master mix (250 μg/μl BSA, 100 μM each dNTP, 50 mM TRIS-HCl, 4 mM Mg2+, 0.4U Taq DNA polymerase, 0.25 μl Sybr Green 1, 500 nM each primer). Following previous optimisation, informing selection of a 50 cycle protocol, PCR was carried out as follows; 94°C for 45 seconds followed by 50 cycles of heat to 94°C, cool to 65°C, heat to 74°C, and hold for 5 seconds. Product was detected by melting point immediately following the PCR reaction; melting temperature is a function of guanidine-cytosine content and product size. HSV product gives a product with a melting point of 92.5°C (plus or minus 0.5°C), total time approximately 30 minutes. The primers used were KS30 sense, 5' TCAAGGCCACCATGTACTACAAAGACGT (1022–1050) KS31 antisense, 5' GCCGTAAAACGGGGACATGTACACAAAGT (1453–1425) which are homologous to the protein coding region of the glycoprotein B (gB) gene of the HSV-1 and HSV-2 genomes (virus strains KOS and HG52 respectively).4
Key messages
-
Adoption of PCR in a routine GUM clinical setting is feasible, efficient and, in this population, increased the overall HSV detection rate by 24%
-
With both conventional culture and PCR, lesion duration and morphology are associated with likelihood of HSV detection
-
PCR shows promise as a cost efficient technology in diagnosis of genital herpesvirus infections
Typing of the PCR amplicon was by restriction fragment length polymorphism (RFLP), using the restriction enzyme BssHII (Roche Molecular Biochemicals, Lewes, UK), which cuts at G↓CGCGC. This sequence occurs at 1379–1384 in HSV-1 but not in HSV-2. The PCR was repeated using a hybrid Omnigene to obtain amplicon for restriction digest. For the reaction, 10 μl of extracted DNA was added to 40 μl of master mix (200 μM each dNTP, 75 mM TRIS-HCl (pH 8.8 at 25°C), 20 mM (NH4)2SO4, 2.0 mM MgCl2, 0.01% v/v Tween 20, 1.25U Taq DNA polymerase). PCR was carried out as follows; 94°C × 2 minutes 1 cycle, 94°C × 1 minute, 55°C × 1 minute, 72°C × 1 minute, 35 cycles, 72°C × 5 minutes 1 cycle. The resulting amplicon was used for restriction digest. The digest was carried out under the following conditions; 10 μl of amplicon was added to 40 μl of restriction digest mix (33 mM TRIS-citrate, 66 mM K-acetate, 10 mM Mg-acetate, 0.5 mM dithiothreitol, pH 7.9 (at 37°C), 2U BssHII). This was incubated at 50°C for 4 hours. Products were electrophoresed on a 2%, 3:1 NuSeive agarose gel stained with GelStar (Flowgen). HSV-1 gives a characteristic cut band of 357 bp, as opposed to HSV-2 which has an uncut band at 431 bp.
Statistical analysis
Statistical analysis was performed using κ2 tests on spss software.
RESULTS
Over the study period, 236 patients agreed to participate and paired specimens were available from all for analysis. Table 1 shows the results of both methods of viral detection in relation to clinical characteristics. Overall, 109 patients (46%) had a positive test for HSV, by either PCR or culture. A total of 187 specimens were taken from genital sites, of which 95 (50.8%) were positive; 18 were from extragenital sites, of which a much lower proportion (5/18; 27.8%) were positive (κ2 = 7.7, p=0.02). The site of the lesion was unknown in 31 patients. Sixty three patients had a past history suggestive of genital herpes, which was previously identified as HSV-2 in 11, HSV-1 in three, and not culture confirmed in the remaining 49. Fourteen study participants were taking antiviral therapy at the time of sampling.
Clinical characteristics
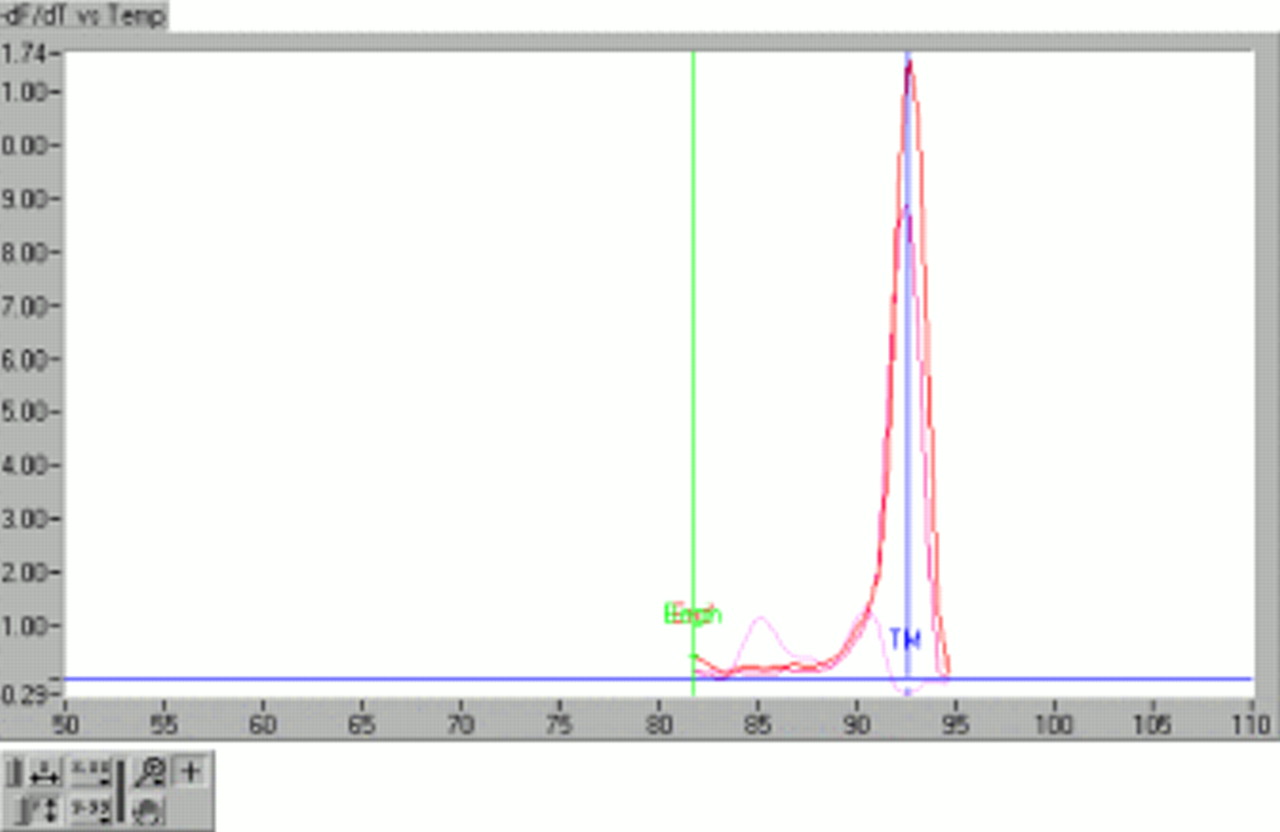
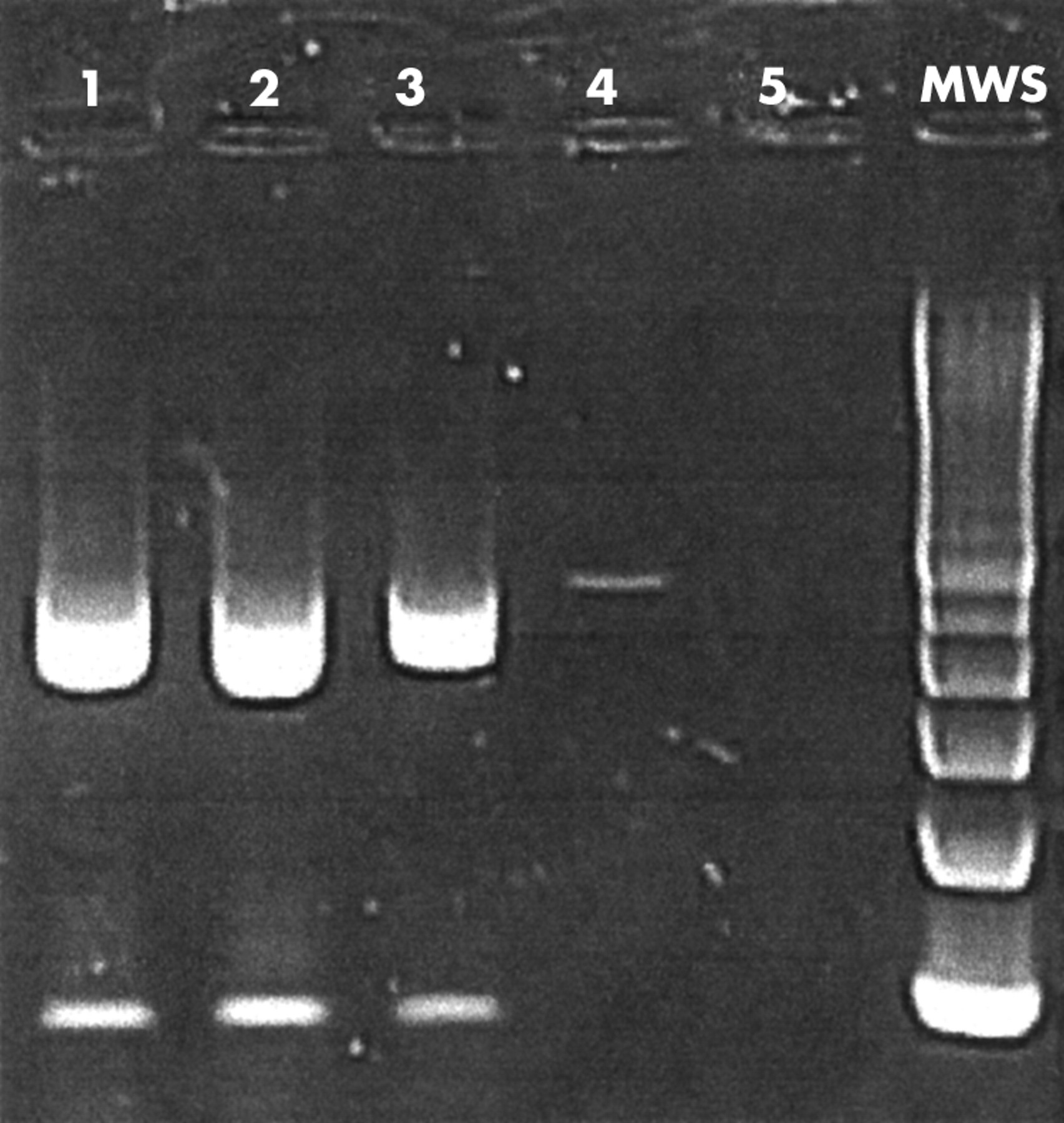
Table 2 compares results of virus culture with PCR. Figure 1 provides an example of the readout from the LightCycler. In 88 patients, both PCR and culture were positive. In 21 patients (24% of all positive tests), the PCR was positive and virus culture was negative. Ten of these had a past medical history of culture confirmed genital herpes. All positive PCR tests were analysed by restriction endonuclease digestion and gel electrophoresis, showing a banding pattern characteristic of HSV-1 or HSV-2 (fig 2). No patients with positive cultures had negative PCR results. There was no difference in the rate of PCR positivity between the samples transported in TM and LB; all PCR positive specimens were positive in both samples.
Comparison of virus culture with PCR: overall results

Electronic output of LightCycler. One positive sample and one positive control have generated the high peaks. The negative control has generated the much lower dual peak profile. The peak indicates fluorescence intensity, so correlates with the amount of PCR product or primer-dimer generated. The product is heated until its melting temperature (TM), at which point the product dissociates into two single DNA strands and the fluorescence is lost. The TM is specific to the length of the product and the GC content.

{kind=link}
{kind=link}
Gel electrophoresis showing characteristic banding patterns of HSV-1 and HSV-2. PCR products are digested as described in Methods. As HSV-1 contains the specific restriction enzyme site but HSV-2 does not, only HSV-1 is digested into two bands. The lengths of the two bands add up to the overall length of the uncut product. The upper band appears brighter, despite being equimolar with the lower, because it is much longer; consequently, more fluorescent dye intercalates into the DNA.
Table 3 shows the results of both methods of viral detection in relation to lesion morphology and duration. Lesion duration and morphology remained strongly associated with the likelihood of obtaining a positive HSV detection test, irrespective of the HSV detection method used. Compared with culture alone, use of PCR increased the yield of positive results by 2/15 (13.3%) in specimens from vesicular lesions, by 17/62 (27.4%) from ulcerative lesions, and by 1/5 (20.0%) from crusting lesions. Negative PCR results were obtained in 12 (41.4%) patients presenting with vesicles, 74 (48.4%) with ulcers, and 20 (76.9%) with crusting lesions.
Virus culture and PCR results, by lesion characteristics
Twenty one patients had positive PCR tests and negative cultures (in 20, data were available on clinical characteristics) and 89 were both PCR and culture positive, with clinical data available in 87. Table 4 compares the clinical characteristics of the two subgroups. Although a higher proportion of the patients who were PCR positive only (4/20; 19%) had lesions of more than 10 days' duration, compared with 8/87 (9%) of the patients with concordant PCR and culture results, this was not statistically significant (p=0.3).
All PCR positive specimens; comparison of culture positive and culture negative specimens
DISCUSSION
In this direct comparison of PCR with virus culture in patients presenting to a large GUM clinic with clinical features suggestive of genital herpes, PCR increased the overall detection rate of HSV by 24%. This improvement in test performance was observed across a wide range of clinical presentations and was not associated with lesion morphology or duration.
Virus culture has hitherto been the standard test used in routine clinical practice for diagnosis of genital herpes.2 However, it has a number of deficiencies; it fails to detect virus in a substantial proportion of infected individuals, even in the presence of clinical lesions. In Scotland, 849 patients attended GUM clinics during the year ending March 1999 with clinical features suggestive of genital herpes; however, culture confirmation was only obtained in about half (483; 57%).5 The findings of the present study suggest that if PCR had been the diagnostic method employed a further 116 patients could have been given an accurate diagnosis, including typing information, which allows accurate advice to be given to patients about issues such as recurrence risk, frequency of subclinical shedding, and risks of potential transmission to partners, which differ substantially between HSV-1 and HSV-2.6 Culture also requires a laboratory with tissue culture facilities and is highly dependent on the stage of clinical lesions; while HSV can be isolated from over 90% of vesicular or pustular lesions, isolation of virus from lesions at the ulcerative stage is only 70% and falls to 27% at the crusting stage of disease.7 A further problem with current reliance on virus culture is the need to transport live virus to the laboratory within a short period, which requires maintenance of the cold chain at 4°C. If a molecular detection method is used preservation of viable organisms is not essential and transporting issues would become less critical to the diagnostic outcome.
PCR is a well characterised method for rapid and sensitive diagnosis of HSV but, largely because of its cost and the requirement for appropriately trained technical staff, its role has been confined to investigation of suspected HSV encephalitis.8 Four previous published studies have compared the performance of PCR with virus culture diagnosis of genital herpes in a routine clinical setting, with consistent findings of superior sensitivity of PCR; compared with PCR, the sensitivity of culture ranged between 67% and 81%.9–12 Cullen et al compared PCR and culture, using combined culture and PCR as a “gold standard” in specimens taken from 112 ulcerative genital lesions.9 PCR had a sensitivity of 93.2% and a specificity of 100%, compared with respective values of 84.1% and 100% for culture. Safrin et al reported on PCR and culture on samples from 246 patients with a wide spectrum of lesions at all clinical stages.10 Thirty one samples were PCR positive and culture negative; in contrast with the present study, discrepant results were significantly more likely to occur with lesions which were crusted or of longer duration. The Safrin study reported 27 cases of typical genital herpes, including two with vesicular lesions and 15 with ulcers, in which all were PCR negative. In the present study, 12 of 29 (41%) patients with vesicular lesions and 74 of 153 (48%) with ulcers had a negative PCR result. Collectively, these data show that the diagnosis remains a difficult one to confirm; several factors, including poor primers, poor assay sensitivity, poor sample collection in the context of painful genital lesions, and lack of specificity of clinical diagnosis may potentially contribute to this. The sensitivity and specificity of the PCR assay used in the present study has been compared previously with nested PCR, with highly concordant results; in a blinded comparison of a single round LightCycler assay with nested PCR, 33 of the 34 specimens positive by nested PCR were positive by the LightCycler assay and 17/17 negative specimens were correctly identified (unpublished in-house data). Underdiagnosis of genital herpes by currently available tests is recognised as a barrier to diagnosis, even when the clinical features invoke a strong clinical suspicion of genital herpes.13 In summary, clinical factors appear to be the predominant explanation for the discordance between clinical and laboratory diagnoses. The present study shows that, in the majority of patients presenting with genital vesicles, a diagnosis of HSV infection will ultimately be made and PCR significantly increases the proportion of cases in which laboratory viral confirmation is achieved. However, a wider differential diagnosis of genital vesicular lesions (including Varicella zoster infection) should be considered by clinicians and further clinical research in this area would be desirable.
The potential health gain achievable by introduction of PCR is substantial, in respect of improved case detection and (as yet unproved) potential for prevention of transmission by appropriate information provision at the time of diagnosis. Although a formal health economic analysis was not within the remit of this study, the costs of consumables and staff time were calculated; for PCR, this was estimated at £29.35 per test and, for viral isolation, £42.22. In the present study, 109/236 samples were found to be positive by PCR and 88/236 by isolation; this equates to a cost per case detected of £63 for PCR and £113 for viral isolation, suggesting that PCR shows promise as a cost efficient technology in diagnosis of genital herpesvirus infections. From a laboratory resource perspective, use of the LightCycler significantly improved efficiency of testing. After extraction of DNA, final confirmation of the results took 30 minutes, contrasting with the 3–4 hours that would be required for a standard PCR gel running protocol. Consequently, HSV detection and typing results are potentially available to the clinician within a single working day. Although only a small volume of amplicon is generated, this is sufficient for digestion. We are currently developing an assay that will allow discrimination between HSV-1 and HSV-2 without a subsequent digestion.
In summary, we advocate adoption of PCR as an efficient HSV detection and typing method for diagnosis of genital herpes in routine GUM practice.
CONTRIBUTORS
AS contributed to all aspects of the study design, coordinated clinical data collection, performed data analysis, and wrote the first draft of the manuscript; GG contributed to all aspects of the study design, performed all laboratory analyses and contributed to data analysis; WFC formulated the original idea for the project, contributed to all aspects of the study design, and assisted with revision of the final version of the manuscript.
REFERENCES
Linked Articles
- Brief encounters