Article Text

Abstract
Lymphogranuloma venereum is caused by serovars of Chlamydia trachomatis. It is rare in industrialised countries, but is endemic in parts of Africa, Asia, South America, and the Caribbean. We discuss its clinical features, diagnosis, and management.
- lymphogranuloma venereum
Statistics from Altmetric.com
L ymphogranuloma venereum (LGV) is caused by serovars L1, L2, and L3 of the obligate intracellular bacterium Chlamydia trachomatis. These LGV strains are more virulent in animal models than the more prevalent serovars A–K of C trachomatis, and more invasive in humans. Whereas serovars A–K are largely confined to mucosal columnar epithelial surfaces of the genital tract and eye, the LGV serovars infect predominantly monocytes and macrophages, pass through the epithelial surface to regional lymph nodes, and may cause disseminated infection.
EPIDEMIOLOGY
LGV is a rare disease in industrialised countries, but is endemic in parts of Africa, Asia, South America, and the Caribbean. Its epidemiology is poorly defined, since it cannot be distinguished clinically from other causes of genital ulceration with bubo formation—for example, chancroid, and it is difficult to diagnose with confidence in the laboratory. Clinic based series of patients with genital ulcer suggest that it is an uncommon cause of genital ulceration in Africa.1,2 Ten per cent of patients with buboes presenting to an STD clinic in Bangkok were found to have LGV,3 and a large epidemic of LGV has been reported recently among “crack” cocaine users in the Bahamas.4
CLINICAL FEATURES
The clinical features are illustrated in figures 1 and 2. The clinical course of LGV can be divided into three stages. The primary stage involves the site of inoculation; the secondary stage the regional lymph nodes and sometimes the anorectum; and late sequelae, affecting the genitals and/or rectum, comprise the tertiary stage.

Left sided inguinal bubo and penile ulceration in LGV. (Photograph by courtesy of David Lewis.)

Close up of the LGV associated penile ulceration shown in figure 1. (Photograph by courtesy of David Lewis.)
Primary stage
After an incubation period of 3–30 days, a small, painless papule, which may ulcerate, appears at the site of inoculation (usually the prepuce or glans in men, and the vulva, vaginal wall or, occasionally, cervix in women). The primary lesion is self limiting. It may not always occur, and may pass unnoticed by the patient. In a series of LGV patients presenting with buboes in Thailand, more than half had not been aware of an ulcer.3
Secondary stage
The secondary stage occurs some weeks after the primary lesion. It may chiefly involve the inguinal lymph nodes, or the anus and rectum. The inguinal form is more common in men, since the lymphatic drainage of the vagina and cervix is to the retroperitoneal rather than the inguinal lymph nodes. Proctitis due to LGV is more common in women and in men who practise receptive anal intercourse, and is thought to be due to direct inoculation.
The cardinal feature of the inguinal form of LGV is the presence of painful inguinal and/or femoral lymphadenopathy, which is usually unilateral. The presence of adenopathy above and below the inguinal ligament gives rise to the “groove sign,” once believed to be pathognomonic for LGV, in 10–20% of cases.5 Enlarged lymph nodes are usually firm, and biopsy reveals small discrete areas of necrosis surrounded by proliferating epithelioid and endothelial cells. These areas of necrosis may enlarge to form stellate abscesses, which may coalesce and break down to form discharging sinuses, though this phenomenon occurs in less than a third of patients, and is more common in chancroid.
Extragenital inoculation can give rise to lymphadenopathy outside the inguinal region. For example, cervical adenopathy due to LGV has been reported following inoculation during oral sex,6 and laboratory workers who developed pneumonitis following accidental inhalation of LGV strains of C trachomatis were found to have mediastinal and supraclavicular adenopathy.7 Ocular inoculation can give rise to a follicular conjunctivitis, often accompanied by preauricular lymphadenopathy. Many patients feel systemically unwell, with fever, myalgia, and headaches.
Anorectal involvement in early LGV was described many years ago, predominantly in women and homosexual men, presenting with an acute haemorrhagic proctitis. Patients present with rectal pain and bleeding, often with pronounced systemic features (fever, chills, and weight loss). Proctoscopy reveals a granular or ulcerative proctitis, resembling ulcerative colitis, confined to the distal 10 cm of the anorectal canal.8,9
Tertiary stage
Chronic inflammatory lesions caused by C trachomatis often lead to scarring in both the eye and genital tract. In chronic untreated LGV, fibrosis can lead to lymphatic obstruction, causing elephantiasis of the genitalia in either sex, and rectal involvement can lead to the formation of strictures and fistulae. These conditions are more common in women, and can give rise to the syndrome of esthiomene (Greek: “eating away”), with widespread destruction of the external genitalia.
DIAGNOSIS
Differential diagnosis
LGV may present as a genital ulcer or as inguinal lymphadenopathy (usually painful) without evidence of genital ulceration. The differential diagnosis of sexually acquired genital ulceration includes chancroid, herpes, syphilis, and donovanosis (granuloma inguinale). Less common causes include trauma, non-venereal infections such as cutaneous leishmaniasis, and fixed drug eruption.
The differential diagnosis of inguinal adenopathy includes chancroid, herpes, and syphilis, although there is usually a genital ulcer or at least a history of an ulcer in these conditions. Unilateral inguinal or femoral lymphadenopathy should prompt a careful search for septic lesions of the leg or foot. Chronic sinus formation in the inguinal region may be due to tuberculosis of the lumbar spine, and bubonic plague should be considered in the acutely ill patient with inguinal lymphadenopathy in endemic areas.
Generalised lymphadenopathy has a wider differential diagnosis, including HIV infection and lymphoma, and should be excluded by careful palpation of the neck, axillae, and epitrochlear regions.
Laboratory diagnosis
In the past, LGV was diagnosed by the Frei skin test, a test of delayed type hypersensitivity to chlamydial antigens, similar to the tuberculin test. This test was not as sensitive as serology, and probably resulted in many false positives due to genital chlamydial infection with serovars D-K, whose high prevalence has only been appreciated since the 1960s.10 The Frei test antigen is no longer available.
The diagnosis of LGV now depends on serology or on the identification of C trachomatis in appropriate clinical samples. When available, histopathological examination of biopsy specimens can also support the diagnosis.
Serology
The complement fixation (CF) test has been used for many years to diagnose chlamydial infections. It is genus specific, and therefore does not distinguish between infections with C trachomatis, C psittaci, and the common respiratory pathogen C pneumoniae. Because it is more invasive, LGV leads to higher titres of serum antibody than uncomplicated genital infections with C trachomatis serovars D–K. A titre of >1:256 strongly supports the diagnosis, while a titre of <1:32 rules it out except in the very early stages of the disease.11
The microimmunofluorescence (MIF) test can distinguish between infections with different chlamydial species, but has not been much used in routine clinical practice, since it requires a fluorescent microscope and a skilled technologist trained in the technique.12 Moreover, until recently the test has not been commercially available. A MIF IgG titre of >1:128 strongly suggests LGV, although invasive genital infection with C trachomatis serovars D-K (for example, pelvic inflammatory disease) can also give rise to high serum titres of antichlamydial antibody.4,5 A number of enzyme immunoassays (EIAs) are on the market for the serological diagnosis of chlamydial infection, but they have not been widely evaluated. Most do not distinguish between infection with different chlamydial species.13
Identification of the organism
C trachomatis can be identified in bubo fluid following aspiration, or in ulcer material. In contrast with chancroid, buboes of which contain large amounts of pus, the buboes of LGV may contain only small amounts of thin milky fluid, and it may be necessary to inject 2–5 ml of sterile saline to obtain any fluid by aspiration.3 C trachomatis can be isolated in tissue culture, using HeLa-229 or McCoy cell lines, but this technique is not widely available. Alternatively, C trachomatis can be identified by direct fluorescent microscopy using a commercially available conjugated monoclonal antibody on a smear of bubo or ulcer material. This method is less demanding, but still requires a fluorescent microscope and a skilled technologist.3
Commercially available EIAs, which detect chlamydial antigens (usually lipopolysaccharide, LPS) are widely used to diagnose urethral and cervical infection with C trachomatis serovars D–K, but have not been evaluated for the diagnosis of LGV. DNA amplification assays—for example, polymerase chain reaction (PCR) or ligase chain reaction (LCR), which detect Chlamydia specific genomic or plasmid DNA, are the most sensitive tests available for the diagnosis of genital C trachomatis infection14 but have not been well evaluated for the diagnosis of LGV. PCR has been used to diagnose LGV in samples taken from genital ulcers in the Bahamas.4
It is important to note that the detection of C trachomatis in bubo material by any of these methods strongly supports the diagnosis of LGV, whereas the detection of the organism in material from genital ulcers only supports the diagnosis if it can be shown to be an LGV strain by DNA sequencing or typing with a monoclonal antibody. This is because ulcers may be contaminated with C trachomatis serovars D–K in patients with uncomplicated urethral or cervical infections due to those strains.
MANAGEMENT
Only one comparative study of different treatment regimens for LGV has been reported. Greaves et al compared the effect of various regimens of chlortetracycline, oxytetracycline, chloramphenicol, and sulphadiazine on the rate of healing of buboes and on the occurrence of relapse and complications (for example, sinus formation).15 No difference was observed between any of the regimens, but statistical power was low since there were less than 10 patients in each group.
Recommended treatment for both bubonic and anogenital LGV is tetracycline 500 mg four times daily for 14 days or doxycycline 100 mg twice daily for 14 days or erythromycin 500 mg four times daily for 14 days.16,17 Erythromycin should be given to pregnant women, in whom tetracyclines are contraindicated. Acute anogenital disease usually responds dramatically to antibiotic treatment, bubonic disease more slowly. Patients with advanced disease may require treatment for more than 14 days. Large collections of pus should be aspirated, using a lateral approach through normal skin.
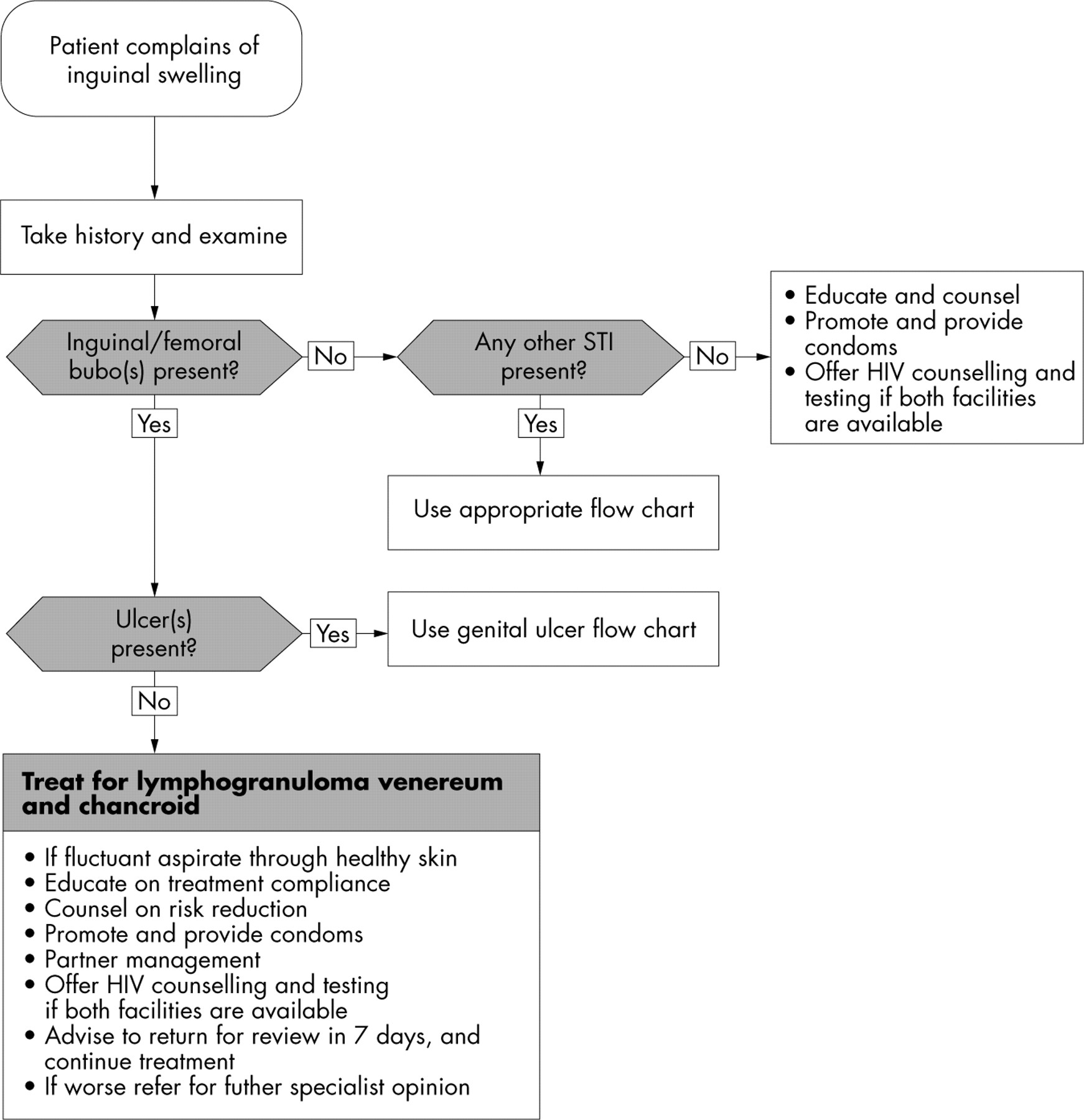
In practice, it is often difficult or impossible to distinguish LGV from chancroid. Syndromic management guidelines for both genital ulcer and inguinal bubo are available from the World Health Organization. The flow chart for genital ulcer does not include treatment for LGV, since it is a less common cause of this condition than chancroid and syphilis in most areas. As mentioned above, erythromycin is effective against both chancroid and LGV, but a longer course of treatment is recommended for LGV. The flow chart for inguinal bubo recommends treatment for both chancroid and LGV in patients without genital ulcers17 (see fig 3).
{kind=link}
{kind=link}
{kind=link}
Flow chart for management of inguinal swelling.
Azithromycin, if available, is likely to be effective against both conditions, but has not been evaluated for the treatment of LGV. A single oral dose of 1 g is effective against uncomplicated genital chlamydial infections caused by non-LGV strains; a longer course is likely to be required for the treatment of LGV.
Late complications such as rectal stricture may be improved by antibiotic treatment, which reduces the inflammatory component, but does not correct damage due to fibrosis. Rectovaginal fistula, bowel obstruction, and esthiomene require surgical correction under antibiotic cover.