Article Text

Abstract
Objectives: Herpes simplex virus type 2 (HSV-2) is the most common cause of ulcerative genital disease in the United States, but infection is commonly unrecognised. Serological screening tests could identify discordantly infected couples and permit targeted interventions to limit HSV-2 transmission. Our objective was to evaluate the projected cost effectiveness of strategies to prevent HSV-2 transmission in couples with no history of HSV-2 infection.
Methods: We created a mathematical model to simulate the natural history and costs of HSV-2 transmission, and the expected impact of HSV-2 prevention strategies in monogamous, heterosexual couples. Strategies evaluated included (i) no screening; (ii) universal condom use; and (iii) serological screening for HSV-2 with condom use targeted to discordant couples. Screening tests considered included western blot (WB), ELISA, and ELISA with confirmation of positive test results using WB (ELISA→WB).
Results: Compared to no screening, the use of ELISA→WB prevented 38 future infections per 1000 couples, with a cost effectiveness ratio of $8200 per infection averted. The use of WB in all couples had an incremental cost effectiveness ratio of $63 600 per infection averted. Strategies of ELISA alone and universal condom use were not cost effective. The cost effectiveness of ELISA→WB improved with increasing prevalence of HSV-2, but worsened with decreasing condom compliance. Screening with ELISA alone was a reasonable strategy only when ELISA specificity increased to 99%.
Conclusions: Serological screening for unrecognised HSV-2 infection in monogamous, heterosexual couples is expected to decrease the incidence of HSV-2 infection, but increase healthcare costs. For couples choosing to be screened, a two step testing strategy (ELISA→WB) is recommended. Recommendations for a national policy to conduct serological screening will depend on the value placed on averting an incident HSV-2 infection.
- genital herpes
- screening
- cost effectiveness analysis
Statistics from Altmetric.com
Herpes simplex virus type 2 (HSV-2) is the most common cause of ulcerative genital disease in the United States, with serological evidence of infection present in 22% of adult Americans.1 The prevalence of HSV-2 infection increased by 30% between 1976 and 1994.2,3 The morbidity and economic consequences attributable to HSV-2 infection are substantial.1,4,5 Infection with HSV-2 may result in a wide spectrum of disease manifestations, including primary genital herpes syndrome,6 recurrent genital ulceration,7,8 and neonatal herpes simplex virus infection.9,10 Genital HSV-2 infection also appears to facilitate sexual transmission of the human immunodeficiency virus (HIV).11
The regular use of condoms may decrease the rate of transmission of HSV-2 infection by as much as 50%–75%.12–16 Antiviral drugs such as aciclovir decrease viral shedding, and may decrease the rate of transmission.17–19 While individuals with recognised HSV-2 infection may be able to employ such interventions to reduce transmission to sexual partners, many infected individuals are not aware of their infection and are therefore unlikely to use these interventions.3,20–22 The sexual partners of individuals with asymptomatic or unrecognised HSV-2 infection are vulnerable to the full spectrum of HSV-2 associated symptoms.23,24 Transmission of HSV-2 infection by a male with unrecognised infection to a pregnant female partner may also result in maternal-fetal transmission of HSV-2 infection, which may cause severe illness in the neonate.25–27
Consideration of serological screening is motivated by the assumption that identifying an unrecognised infection with HSV-2 in one member of a serodiscordant couple would lead to effective interventions to decrease the risk of transmission to the uninfected partner. An existing western blot (WB) assay is often considered to be a “gold standard” test for HSV-2 infection,28,29 but is expensive and requires considerable expertise for performance and interpretation. Recently, several enzyme linked immunosorbent assays (ELISA) capable of distinguishing infection with HSV-2 from infection with herpes simplex virus type 1 (HSV-1) have been developed. These assays are less costly than WB assays, and have high sensitivity and specificity.30
Our objective was to synthesise the available data in order to project the future impact of currently available HSV-2 screening methods on the future health of monogamous, heterosexual couples with no history of symptomatic genital herpes. In order to do so, we created a mathematical model that simulated the natural history of HSV-2 transmission, and the future costs and consequences of incident infection with HSV-2.
METHODS
The model
We constructed a Markov model (using data 3.5 (Treeage Software, Inc, Williamstown, MA, USA))31 that incorporated the probability of discordant infection status in couples, the risk of HSV-2 transmission, and future costs and consequences of new HSV-2 infections. The model was used to evaluate the cost effectiveness of HSV-2 control policies in a target population of hypothetical 25 year old couples planning to embark on a future monogamous, heterosexual relation that might include childbearing. Data on the prevalence of HSV-2 infection and the probability of symptomatic infection were used to estimate the proportion of couples who would have discordant infection status, (that is, male infected and female uninfected, or vice versa), if random assortment of the population occurred.32 The incorporation of test characteristics into the decision model permitted estimation of the proportion of couples that would be correctly or incorrectly identified as having discordant infection status if available screening methods were used.
Markov models depict the natural history of disease as an evolving sequence of health states, defined to capture important clinical outcomes and costs. In our model, health states were based on the status of the couple, rather than the individual. Possible health states included: (i) asymptomatic couple with discordant infection status; (ii) asymptomatic couple with concordant infection status; and (iii) couple with concordant infection status, with one partner experiencing symptomatic HSV-2 infection. These health states were further subdivided to reflect pregnant and non-pregnant health states in the female partner.
Transition probabilities derived from the published medical literature were used to move couples through different health states over a 25 year period (fig 1). In any given month, a couple who entered the model with discordant infection status could remain discordantly infected, or could move to a health state characterised by symptomatic or asymptomatic infection in the previously uninfected partner.

Markov model of initially asymptomatic couple with discordant HSV-2 infection status. The model has three couple health states as shown above. Allowed transitions between health states are indicated by arrows. The health states include: (i) asymptomatic couple with discordant infection status; (ii) asymptomatic couple with concordant infection status; and (iii) couple with concordant infection status, with one partner experiencing symptomatic HSV-2 infection. In couples with discordant infection status, infection may be transmitted to the uninfected partner as time passes. An individual who acquires symptomatic infection with HSV-2 may move first through a temporary “primary genital herpes” health state, characterised by the possibility of hospitalisation and increased healthcare costs.
We projected medical and patient-time costs, and projected the effectiveness of screening strategies with regard to new adult and neonatal HSV-2 infections. The comparative performance each strategy was expressed using the incremental cost effectiveness ratio.33 Sensitivity analyses were conducted to determine the stability of the results in the face of reasonable variation in model parameters.
In the base case analysis, we assumed that all couples remained monogamous over time with a constant frequency of sexual intercourse, and that the infectiousness of an asymptomatically infected individual did not decrease over time.34 The analysis assumed a societal perspective and, except where otherwise stated, followed the reference case recommendations of the Panel on Cost Effectiveness Analysis in Healthcare and Medicine.31
Clinical strategies
We evaluated three potential policies: (I) no intervention; (ii) universal condom use without serological screening; and (iii) serological screening for HSV-2 with condom use targeted to serodiscordant couples. Three distinct screening strategies were considered and included WB alone, screening with type specific ELISA alone, and screening with type specific ELISA followed by a confirmatory WB in individuals with a positive ELISA result (ELISA→WB).
Partners with newly acquired symptomatic infection were projected to experience an average number of future symptom days, based on published distributions of relapse rates of relapse in the first year of symptomatic genital herpes infection,8 and a linear decline in symptom frequency in subsequent years.35 Age specific live birth rates were used to estimate the probability that female partners were in the third trimester of pregnancy at the time of incident infection.36 In the base case, only women experiencing incident infection in the third trimester were considered to be at risk for maternal-fetal transmission of HSV-2.10 We performed exploratory analyses on the costs, benefits, and cost effectiveness of the use of aciclovir,17 instead of condoms, to prevent transmission of HSV-2 to uninfected partners.
Clinical data
Parameters used for the base case analysis are shown in Table 1. In order to estimate each probability and establish its plausible range, we conducted a formal review of the literature (table 1). A Medline search using the keywords “herpes,” “transmission,” “vaccine,” “couple,” and “clinical trial” identified studies published between January 1980 and June 2000. Additional studies were identified through a manual search of references and abstracts from major scientific meetings.
Selected model variables
For the purposes of this analysis, we regarded the HSV-2 western blot as a perfect test.28 Estimates of test performance of ELISA assumed the use of current assays directed at antibody to surface glycoprotein G2, which are able to distinguish previous infection with HSV-2 from infection with HSV-1.30
Costs
We assumed that individuals screened would initially require an initial office visit that would include counselling by a physician, and that the medical and patient-time costs associated with such a visit would be equivalent to the costs associated with an average office visit for genital herpes.5 Test costs were based on estimates provided by manufacturers, combined with estimates of technician time costs. Monthly costs of condoms were based on estimates of wholesale prices obtained from a survey of discount condom providers,37–39 combined with an estimated frequency of intercourse of nine times per month.24
Individuals infected with symptomatic HSV-2 accrued medical costs as a result of hospitalisation (if they experienced a severe primary HSV-2 syndrome), physician visits, and drug prescribing for symptomatic episodes and long term suppressive therapy.5,40 It was assumed that patients would be managed in accordance with current Centers for Disease Control and Prevention (CDC) guidelines for the treatment of sexually transmitted diseases.41 In base case analyses, it was assumed that treatment would be with aciclovir, with the costs of valaciclovir and famciclovir incorporated into upper bound cost estimates.40,41
Additional medical costs were attributed the excess occurrence of caesarean sections in women with a history of genital herpes,5 and to the occurrence of neonatal herpes virus infections. Upper bound cost estimates for neonatal herpes incorporated lost productivity associated with long term disability in infants who survive herpes encephalitis.5,27,42 We also estimated non-medical costs, including lost wages and opportunity costs associated with patient clinic visits and hospitalisation, using average US hourly wages.43
RESULTS
Base case
We projected that 23% of the couples in our cohort would be discordantly infected upon entry into the model (table 2). In the absence of condom use, the majority of initially uninfected partners became infected over the subsequent 25 years. The use of condoms increased the median time to transmission of infection, and reduced the probability of infection at the end of the 25 year period.
Couple infection status at baseline, and time to concordance among discordant couples
The clinical outcomes of the five screening strategies in a hypothetical cohort of 1000 monogamous, heterosexual couples are presented in table 3. In the absence of screening or condom use, we projected a total of 170 new infections per 1000 couples over 25 years. The introduction of type specific ELISA with condom use by test discordant couples reduced the projected number of infections to 133 per 1000 couples. The use of ELISA→WB prevented one additional infection in the cohort. In comparison with this strategy, the use of either WB alone or condoms for all couples were equally effective, and prevented an additional two infections.
Projected costs and outcomes of five strategies for prevention of HSV-2 infection in a hypothetical cohort of 1000 couples
In the absence of any preventative intervention (for example, screening or condom use), we estimated that 0.2 neonatal HSV-2 infections would occur in this cohort over 25 years. The use of type specific ELISA and condoms would reduce to 0.095 the projected number of neonatal HSV-2 infections. ELISA→WB prevented an additional 0.003 infections, and the use of WB alone, or universal condom use, prevented 0.005 infections over the subsequent 25 years, relative to ELISA→WB.
Cost and cost effectiveness
In the absence of any preventative intervention, the 25 year costs attributable to HSV-2 infection in a 1000 couple cohort were projected to be approximately $175 000, while screening with ELISA→WB increased projected costs to approximately $495 000 per 1000 couples, for an incremental cost effectiveness ratio of $8200 per infection averted. Screening with WB had an incremental cost effectiveness ratio of $63 600 per infection averted relative to ELISA→WB. The strategies of ELISA alone and universal condom use cost more but were less effective than competing strategies, and so were “dominated.” A strategy is “dominated” when it costs more, but provides less health benefit than some competing strategy; a dominated strategy would not be chosen regardless of available health resources.33
Sensitivity analyses
We tested our model assumptions by performing univariate and bivariate sensitivity analyses (table 4). A plausible range was established for each parameter using the highest and lowest values in the published literature, confidence intervals when available, and by adopting alternative assumptions to those in the base case. The rank ordering of strategy effectiveness remained constant with variation in all parameters except the specificity of ELISA. When the specificity of ELISA was greater than 99%, a strategy involving the use of ELISA alone was no longer dominated by a strategy of ELISA→WB. When the specificity of ELISA increased to 100%, ELISA alone was as effective as ELISA→WB, but was less costly.
Selected univariate sensitivity analyses of the cost effectiveness of ELISA→WB relative to no screening
Aside from ELISA specificity, the projected cost effectiveness of ELISA→WB was also sensitive to condom efficacy, costs, and compliance, to the baseline prevalence of HSV-2 infection in the population, and to assumptions related to relationship duration and monogamy. The cost effectiveness of ELISA→WB was less sensitive, or insensitive, to variation in other model parameters. Our simulation of aciclovir use resulted in an estimated cost effectiveness ratio of $12 700 per infection averted, or slightly more than that associated with condoms.
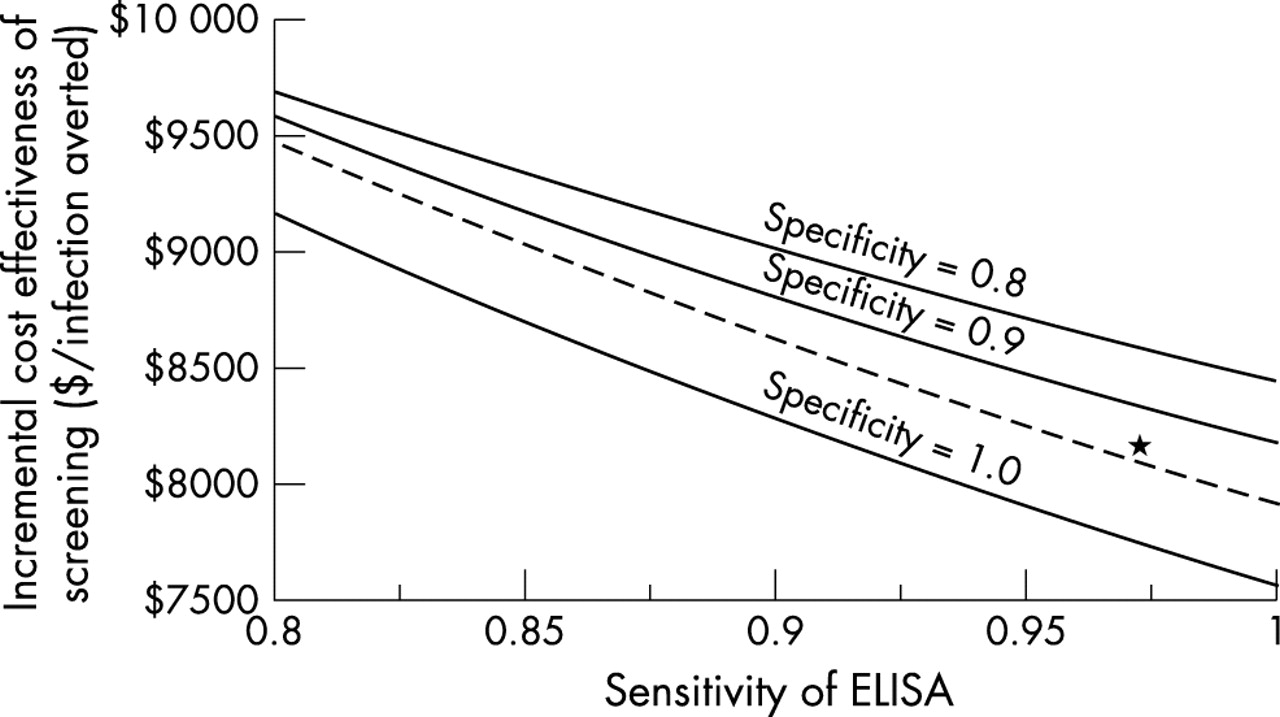
We anticipated that the performance of type specific HSV-2 ELISA might be worsened by use under suboptimal conditions, or improved as a result of ongoing refinement by industry. Therefore we performed two way sensitivity analyses, varying the sensitivity and specificity of ELISA between 80% and 100%. Despite substantial changes in test characteristics, the incremental cost effectiveness ratio associated with screening remained between $7500 and $10 000 per case averted (fig 2).

Two way sensitivity analyses of the sensitivity and specificity of HSV-2 type specific ELISA. Each line represents a different estimate of ELISA specificity. For any specificity, increasing sensitivity results in a decrease in the incremental cost effectiveness ratio of screening relative to no screening. Where ELISA specificity is equal to 80% or 90%, the cost effectiveness ratio represented is that of ELISA→WB relative to no screening. When ELISA specificity is equal to 100%, screening with ELISA→WB (broken line) costs more, but is no more effective than screening with ELISA alone (bottom solid line), and so is dominated by the latter strategy. Asterisk represents the base case.
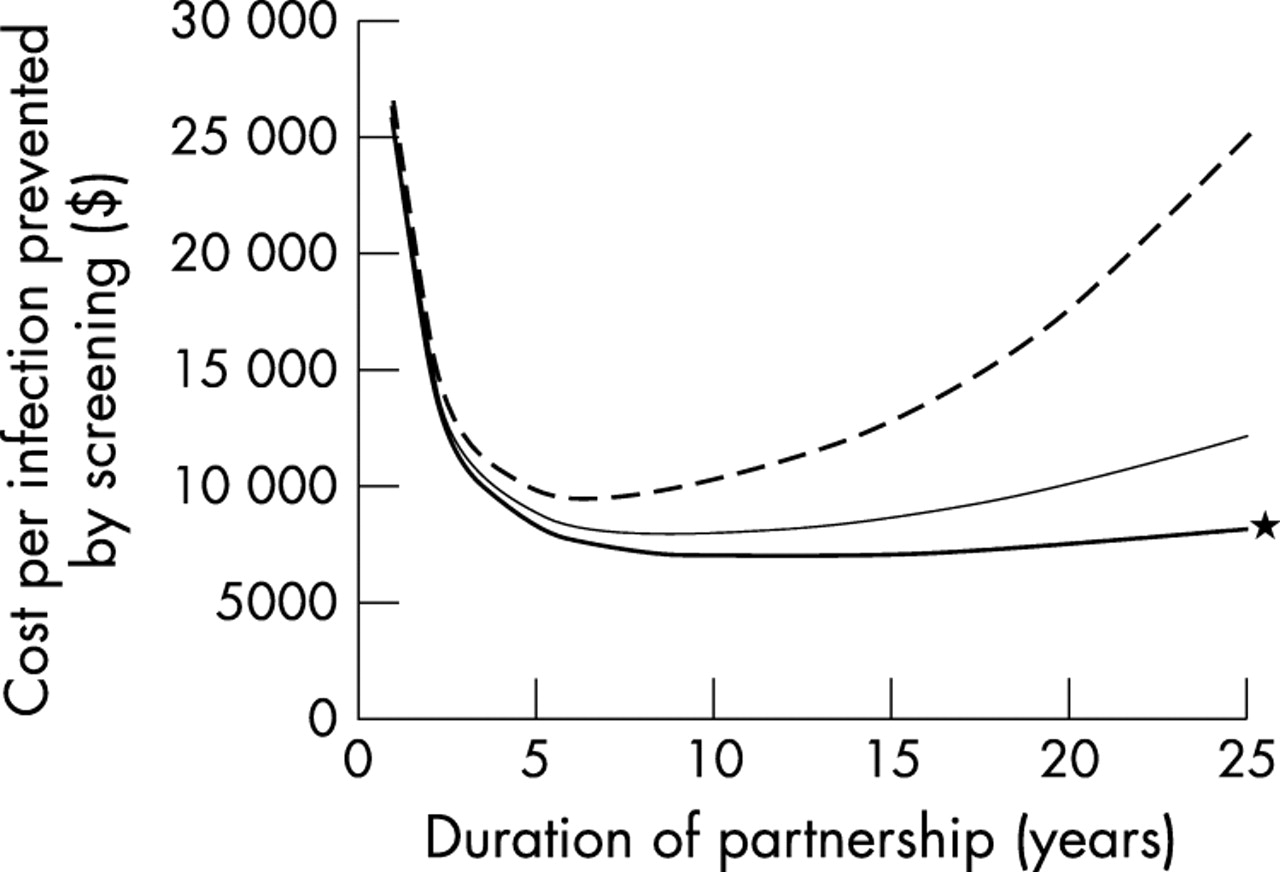
We tested the impact of non-monogamy and abbreviated relationship duration on the cost effectiveness of screening in a two way sensitivity analysis (fig 3). Non-monogamy adversely affected the cost effectiveness of screening, regardless of relationship duration. When the expected duration of relationships was brief, the cost of preventing an incident herpes infection through screening was high, dropping sharply as relationship duration increased. When relationship duration was greater than a decade, the cost per infection averted increased again as a result of delayed infections in couples making use of herpes prevention interventions,44 and as a result of infections acquired via concurrent partners in non-monogamous partnerships.

Two way sensitivity analysis of relationship duration and the impact of non-monogamy. Curves represent the cost effectiveness of screening using ELISA→WB in monogamous partnerships (solid thick line), in partnerships characterised by an average of two additional concurrent partnerships per partner annually (solid thin line), and in partnerships characterised by six additional concurrent partnerships per partner annually (broken line). The cost effectiveness ratio associated with screening is less favourable when relationships are non-monogamous regardless of expected relationship duration. For any level of concurrency, the cost per infection averted through screening initially drops as relationship duration increases. However, with the passing of time, and as delayed infection occurs in partners using preventive interventions, the cost per infection averted again increases. This effect is more marked with higher levels of partner concurrency. Asterisk represents the base case.
We varied the cost and effectiveness of the intervention to prevent HSV-2 transmission in a two way sensitivity analysis (fig 4). It can be seen that programmes involving screening with ELISA→WB followed by an inexpensive but modestly effective intervention (for example, condoms), or an expensive but highly effective intervention (for example, aciclovir) should be adopted by a society willing to pay approximately $10 000 to avoid a single HSV-2 infection.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Two way sensitivity analysis of the monthly cost of an intervention to prevent HSV-2 transmission and percentage reduction in the annual rate of transmission. The lines represent the incremental cost per incident HSV-2 infection averted necessary to implement a screening strategy using ELISA→WB. For a given intervention, the intersection of test cost with a given threshold line can be used to estimate the intervention effectiveness that would be required to reach that cost effectiveness threshold. It should be noted that despite large differences in projected costs and efficacies, both condom use (C) and aciclovir use (A) were estimated to have a cost effectiveness ratio close to $10 000 per infection averted.
DISCUSSION
We developed a mathematical model to estimate the economic costs and health benefits that would result from the adoption of serological screening for HSV-2 infection in monogamous heterosexual couples. Like any mathematical model, our model includes simplifying assumptions and incorporates parameter values that are subject to some uncertainty. None the less, the model’s projection that screening would decrease HSV-2 associated morbidity but increase healthcare costs remained robust in the face of wide ranging sensitivity analyses.
Similarly, our projections related to the use of confirmatory WB assays for individuals with positive ELISA results were robust. Under base case assumptions, the use of type specific ELISA with confirmatory WB would result in fewer incident cases and lower costs than the use of ELISA alone, as long as ELISA specificity remains lower than 99%. Thus, based on the best available data, it can be recommended that if currently available type specific HSV-2 ELISA assays are used for screening in monogamous couples, positive test results should be confirmed using WB assays or other highly specific testing methods.
The high specificity of WB will decrease the use of interventions to prevent HSV-2 transmission by couples in which ELISA falsely identifies one partner as infected. This is expected to diminish costs associated with unnecessary preventative interventions, as well as psychological distress resulting from incorrect identification of an individual as HSV-2 infected. It may be less intuitively obvious that confirmatory WB should enhance the effectiveness of a screening strategy. We believe that this enhancement occurs because of identification of serological discordance in couples in which one partner has a true positive ELISA result while the other partner has a falsely positive result. In the absence of confirmatory WB, interventions to prevent transmission would not be used in such couples, since they would be perceived as concordantly infected.
Using the best available data, we projected that serological screening could prevent a new case of HSV-2 infection at a cost of $8000–$9000. In order to compare the cost effectiveness of screening for HSV-2 to other commonly accepted preventative health interventions the impact of HSV-2 infection needs to be valued using a preference based measure of health gains, such as quality adjusted life years (QALY). However, determining the QALY gains associated with HSV-2 prevention is methodologically complicated, due to: (i) heterogeneity in the course of HSV-2 infection; (ii) limitations in the application of health utility theory to chronic health states punctuated by repeated exacerbations45,46; (iii) the requirement that QALY gains in adults and newborns be incorporated into the denominator of the same cost effectiveness ratio; and (iv) by the requirement that any estimate of QALY gains associated with prevention of infection would have to incorporate loss of health related quality of life among asymptomatically infected individuals who receive a new diagnosis of genital herpes infection as a result of screening.47
None the less, this analytic framework does allow for insight into the magnitude of the impact of HSV-2 infection on health related quality of life that would be necessary for the cost effectiveness ratio associated with HSV-2 screening to fall below $50 000 per QALY, a commonly cited threshold. For example, if prevention of incident HSV-2 infections were associated with a net average gain of 0.2 QALY, screening with ELISA→WB would compare favourably with many commonly accepted preventative health interventions.48 Clinical studies to assess the impact of HSV-2 on health related quality of life are a major research priority.
Our analysis is subject to several important limitations. We have included only asymptomatic, heterosexual couples in this analysis. The use of serological screening in the partners of individuals with symptomatic genital herpes, and in homosexual couples, warrants further exploration. Additionally, it should be noted that our analysis does not address the question of serological screening to prevent genital infection with HSV-1, although this virus does cause a significant, and possibly increasing, proportion of incident genital herpes cases.49
Completion of our analysis has been accompanied by promising reports of an effective vaccine that appears to prevent transmission of HSV-2, at least from men to HSV-1 uninfected women.50 Preliminary exploratory analyses (not shown) suggest that an effective vaccine would provide both health and economic benefits, relative to currently available HSV-2 preventative interventions.
In conclusion, we found that serological screening for HSV-2 infection in asymptomatic, monogamous, heterosexual couples is expected to decrease the incidence of HSV-2 infection in both adults and newborns, but would increase healthcare costs. Recommendations for national policies on serological screening will depend on the value placed on averting incident HSV-2 infections; as such, we recommend that clinical studies to quantify the impact of HSV-2 infection on health related quality of life be given high priority. For healthcare providers of couples who choose to be screened for HSV-2, we recommend the use of a two step testing strategy consisting of an initial ELISA followed by a confirmatory WB for positive ELISA test results.
Key messages
-
Symptomatic genital infections caused by herpes simplex virus type 2 (HSV-2) are common, and may be acquired from sex partners who have unrecognised HSV-2 infection. Serological screening could be used to identify individuals with unrecognised HSV-2 infection, which could reduce the risk of HSV-2 acquisition by their sex partners
-
A mathematical model was constructed to simulate the natural history of genital herpes infection, and to project the cost effectiveness of a screening based herpes prevention strategy in a simulated cohort of monogamous, heterosexual couples
-
The model projected that screening could delay new HSV-2 infections, and could reduce the total number of projected HSV-2 infections, but at a cost of $8000–$9000 per infection prevented
-
The effectiveness of screening with type specific enzyme linked immunosorbent assays (ELISA) was enhanced, and costs were decreased, when positive ELISA results were confirmed through the use of a highly specific herpes simplex virus western blot
Acknowledgments
The authors wish to thank Dr Rhoda Ashley for her kind provision of data on HSV-2 ELISA test performance, Lydia Napper and Marguerite Garwood for expert assistance in preparation of the manuscript, and two anonymous reviewers for helpful suggestions. D Fisman was supported by National Research Service Award No 5-T32-HS00020–15.
CONTRIBUTORS DF contributed to the design and construction of the mathematical model, literature review and synthesis, and manuscript preparation and revision; EH contributed to the literature review and synthesis, manuscript preparation and revision; SG contributed to the design of the mathematical model, literature review and synthesis, and manuscript preparation and revision.
Conflicts of interest: DF, none; EWH, previous honoraria from GlaxoSmithKline; SJG, none.