Article Text

Abstract
Objectives: To assess the feasibility and acceptability of home screening for repeat chlamydial infection using urine test kits sent through the mail.
Methods: A letter offering home rescreening was mailed to 399 adults who previously tested positive for chlamydia. Kits were then mailed to anyone who did not actively decline. The home testing kits contained instructions on how to collect a urine specimen and return the specimen by mail. Specimens were tested with strand displacement amplification. A short survey asked individuals their level of concern about confidentiality, safety, and privacy of mail screening.
Results: Among the 313 potential test kit recipients, 22.4% responded. Response rates were highest among homosexual and bisexual men (38.6%), people 35 years or older (34.3%), and white people (34.6%). The overall positivity rate was 3.2% (2/63). In women 18–25 years old, the positivity was 13.3% (2/15).
Conclusions: Home testing with mailed urine collection kits is feasible and an acceptable method to screen for recurrent chlamydial infection. Young women would probably benefit most because of their higher rates of reinfection and risk for sequelae.
- chlamydia
- screening
- recurrent infection
Statistics from Altmetric.com
Individuals with urogenital chlamydia are at high risk for re-exposure and reinfection, either from untreated partners or other members of a high prevalence sexual network.1 Repeat infection occurs in 13–29% of women within 6 months of initial diagnosis1,2 and in 18% of men within 30 months.3 Studies have suggested that recurrent infections increase the risk for adverse sequelae, such as pelvic inflammatory disease, in women.4,5 Rescreening is now recommended by the Centers for Disease Control and Prevention (CDC) for all women 3–4 months after initial infection.6
Individuals, especially those with little regular contact with the healthcare system, may be more likely to be rescreened if testing is convenient and readily available. Recent studies from the United Kingdom7,8 and Denmark9,10 have shown self collection specimen kits sent through the mail to be an inexpensive and publicly accepted method for chlamydia testing. We evaluated whether screening through the postal system was a feasible approach to test for recurrent infection in treated chlamydia cases.
METHODS
We offered home screening to 399 men and women over 18 years old who initially tested positive for chlamydia at the San Francisco municipal STD clinic (n=200) or other providers (n=199) between January and June 2000.
We sent a letter informing people about the project 1–6 months after the initial positive test. The letter did not refer to past infections or indicate on the envelope that the letter was from the health department. The letter explained the nature of chlamydial infection and informed them that a specimen kit would follow in 1 week for screening. The letter instructed people not wishing to receive a kit to telephone the STD programme to decline. Those declining were subsequently removed from the project.
One week after the mailing of the letters, we mailed large envelopes containing urine specimen shipping kits from Doxtech (Portland, OR, USA). Kits included a letter explaining the project, a flyer providing information about chlamydia, detailed instructions explaining the collection process of first void urine and handling of the specimen cup, and a one page questionnaire that asked individuals to rank their concerns about the confidentiality, privacy, and safety of this type of testing.
We tested urine specimens with strand displacement amplification (SDA) (Becton-Dickinson ProbeTec SDA, Sparks, MD, USA) according to manufacturer’s guidelines. The ProbeTec preservative pouch was included in the mailed specimen cups to allow the specimens to be at ambient (10–20°C) temperature for 2 days.
Health department staff followed up with individuals with positive results according to San Francisco Department of Public Health protocol, providing treatment and partner management.
We analysed data using sas Version 8 (Cary, NC, USA) and conducted χ2 tests to examine between group differences. Costs were calculated by summing the price of specimen cups, packaging and postage, and estimating the labour required to develop educational materials and assemble the kits.
RESULTS
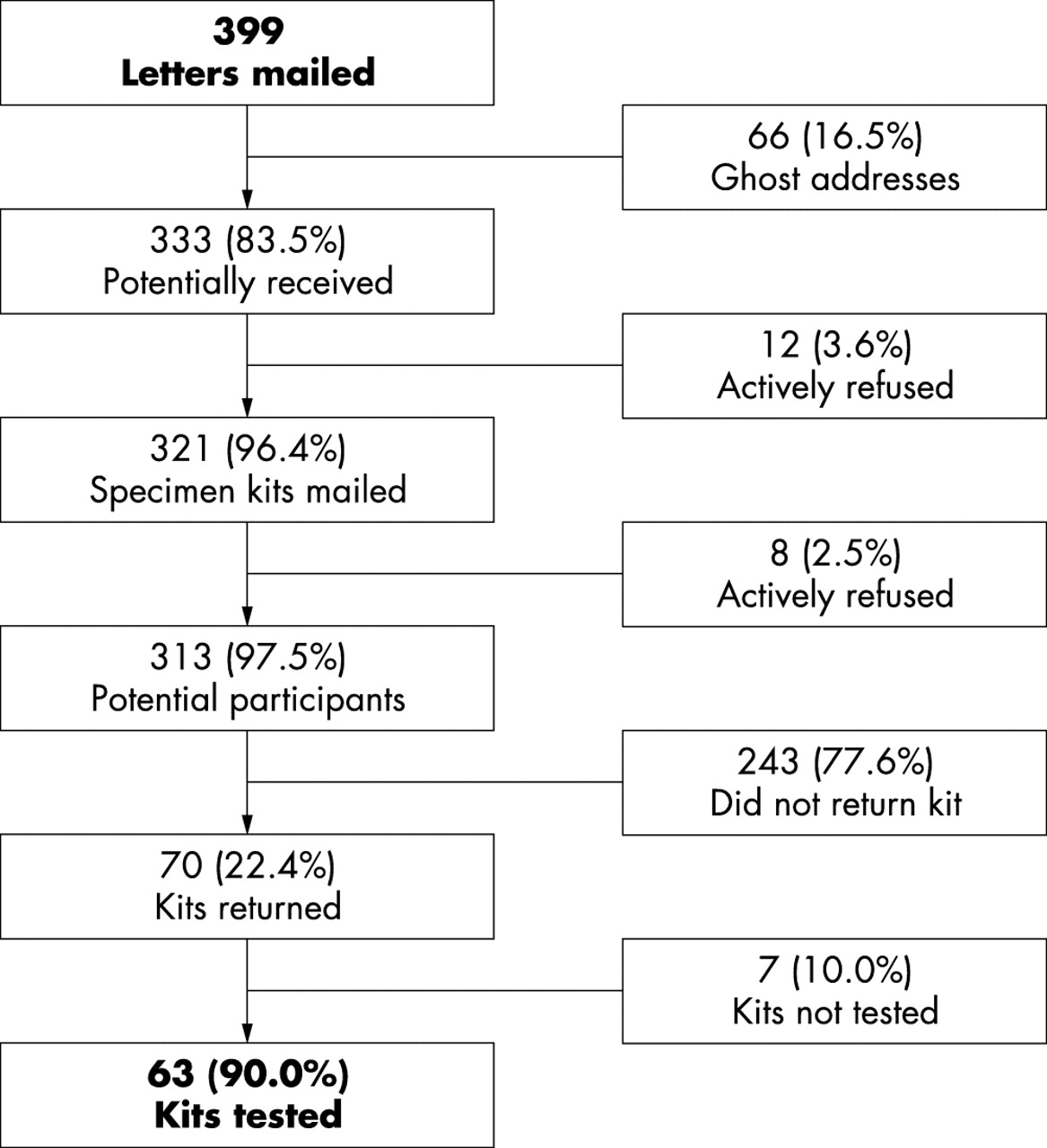
Figure 1 depicts the outcomes of our mailings to 399 people previously diagnosed with chlamydia. Sixty six (16.5%) letters did not reach the addressee (ghost addresses); 20 (5.0%) people declined with six providing comments (four negative and two positive); and, of the 70 kits returned, seven (10.0%) could not be tested because of specimen problems.
{kind=link}
Outcome of mailing to 399 previously diagnosed cases of chlamydia.
Demographic characteristics of individuals mailed a specimen collection kit are summarised in table 1. The proportion of people returning a kit was significantly higher in men who have sex with men (MSM) than women and other men (38.6%, 22.8%, 14.8%; p<0.01); people 35 and older than those aged 25–34 and less than 25 (34.3%, 17.4%, 20.4%; p<0.05), and white people than Hispanic, African-American, or Asian/Pacific Islander (34.6%, 21.5%, 18.0%, 7.9%, p<0.01).
Predictors of return among 313 people receiving chlamydia testing kits
Two (3.2%) of the 63 kits tested were positive for chlamydia; both were heterosexual women younger than 25 years. The female positivity rate was 8.0% (2/25) overall and 13.3% (2/15) among women 18–25 years.
Sixty seven individuals returned questionnaires. More respondents were concerned about confidentiality (51.5%, 34/66) than about privacy (44.6%, 29/65) or safety (42.9%, 27/63). MSM were least likely to be concerned, followed by women and other men, with respect to confidentiality (31.8%, 56.0%, 68.4%, p =0.123), privacy (27.3%, 45.8%, 63.2%, p=0.042), and safety (18.2%, 52.2%, 61.1%, p=0.003). People initially identified through the STD clinic were also significantly less likely to be concerned about confidentiality, privacy, and safety than people identified elsewhere (data not shown).
Eighteen respondents gave additional comments: 15 (83%) were positive about the mail-in screening method. Only three (17%) were negative comments: two reported difficulty in using the test kit and one preferred in-person testing.
The cost of this project included initial letters and postage ($0.40 each), tamper proof specimen cups and shipping boxes ($1.46 each), kit postage ($0.99 each way), educational materials ($0.57 per kit), and staff time assembling the kits ($0.83 per kit). The cost per kit mailed was $5.24, excluding laboratory costs. The total programme cost, excluding laboratory costs, was $1757.49, or $25.11 per specimen returned. The cost per infection detected was $878.75.
DISCUSSION
The primary goal of this pilot project was to assess the feasibility of rescreening for chlamydia by mailing individuals testing kits. Although the response rate (22.4%) was low, this does not necessarily imply low acceptability since kits may not have reached the intended addressee. Participation might increase if patients were educated at the time of visit about the high risk for reinfection and agreed to be rescreened through the mail within 3–4 months of initial infection.
Of the kits that were returned, 90% were successfully tested. Self collection of urine specimens in the home environment, coupled with mail delivery, can be used as a convenient, time saving method for rescreening individuals for chlamydia. The proportion of specimens that could not be tested (10%) might decrease with better instructions on specimen collection and handling.
Another goal of this project was to assess the acceptability of urine based postal chlamydia screening. Although a few negative comments were received, questionnaire data demonstrated that this type of screening was most accepted by homosexual and bisexual men, followed by women and heterosexual men. As with other screening programmes, acceptability and participation are likely to be highest among the “worried well.” A more targeted approach, such as offering postal screening to those at highest risk for reinfection, would decrease the cost per specimen received and high cost per infection detected.
Women are probably the best candidates for postal chlamydia rescreening as they have higher rates of reinfection and worse sequelae. Females younger than 25 years might benefit especially as they have the highest rates of reinfection, and account for a large proportion of all repeat infections.3 Acceptability of postal screening among adolescents is not known since they were not offered postal screening. MSM, who had the highest response rates, could also benefit from urine postal screening if there were evidence of high rates of reinfection. However, urine tests alone would miss other potential sites of infection (for example, rectal infection).
In conclusion, we found that postal screening was both feasible and acceptable as a method of rescreening individuals who have previously tested positive for chlamydia. Postal screening is probably best targeted towards women because of their higher rates of reinfection and risk for sequelae. Further evaluation may elucidate the potential role of postal screening in STD control in high risk populations, such as adolescents and people who do not regularly access medical care.
Acknowledgments
We thank Sally Liska for overseeing the receipt and testing of specimens and Janice Chaw and Bob Kohn for their assistance with data management.
Conflicts of interest: none.
CONTRIBUTORS PB was responsible for the study implementation, data collection, and the first draft of the paper; KS conducted the statistical analysis and contributed to the results and discussion sections; CK guided the data analysis and edited all drafts of the manuscript; JK designed the protocol, questionnaire, and edited the final draft of the manuscript.
Supplementary materials
. Web-only Questionnaire
Available as PDF (printer-friendly file)Files in this Data Supplement:
- [View PDF] - Postal Screening Project