Article Text

Abstract
Objectives:Chlamydia trachomatis (Chlamydia) is the most prevalent sexually transmitted bacterial infection and can cause considerable reproductive morbidity in women. Chlamydia screening programmes have been considered but policy recommendations are hampered by the lack of population based data. This paper describes the prevalence of Chlamydia in 15–29 year old women and men in rural and urban areas, as determined through systematic population based screening organised by the Municipal Public Health Services (MHS), and discusses the implications of this screening strategy for routine implementation.
Methods: Stratified national probability survey according to “area address density” (AAD). 21 000 randomly selected women and men in four regions, aged 15–29 years received a home sampling kit. Urine samples were returned by mail and tested by polymerase chain reaction (PCR). Treatment was via the general practitioner, STI clinic, or MHS clinic.
Results: 41% (8383) responded by sending in urine and questionnaire. 11% (2227) returned a refusal card. Non-responders included both higher and lower risk categories. Chlamydia prevalence was significantly lower in rural areas (0.6%, 95% CI 0.1 to 1.1) compared with very highly urbanised areas (3.2%, 95% CI 2.4 to 4.0). Overall prevalence was 2.0% (95% CI 1.7 to 2.3): 2.5% (95% CI 2.0 to 3.0%) in women and 1.5% (95% CI 1.1 to 1.8) in men. Of all cases 91% were treated. Infection was associated with degree of urbanisation, ethnicity, number of sex partners, and symptoms.
Conclusion: This large, population based study found very low prevalence in rural populations, suggesting that nationwide systematic screening is not indicated in the Netherlands and that targeted approaches are a better option. Further analysis of risk profiles will contribute to determine how selective screening can be done.
- AAD, area address density
- MHS, Municipal Public Health Services
- PCR, polymerase chain reaction
- PID, pelvic inflammatory disease
- PPV, positive predictive value
- chlamydia
- chlamydia trachomatis
- screening
- prevalence
- population based
- the Netherlands
Statistics from Altmetric.com
- AAD, area address density
- MHS, Municipal Public Health Services
- PCR, polymerase chain reaction
- PID, pelvic inflammatory disease
- PPV, positive predictive value
Chlamydia (Chlamydia trachomatis) is the most prevalent sexually transmitted bacterial infection. WHO estimates that 92 million new infections occur annually, of which five million occur in Western Europe.1 In women, chlamydial infections are an important cause of pelvic inflammatory disease (PID), ectopic pregnancy, tubal infertility, and chronic abdominal pain. In men infections can cause prostatitis and epididymitis.2 Vertical transmission from mother to infant can lead to conjunctivitis and pneumonia. Chlamydial infection increases HIV infectiousness and susceptibility.3 Approximately 70% of the infections in women and 50% in men are asymptomatic or subclinical.
Active case finding and early treatment are strategies to prevent the development of sequelae and to reduce transmission. Screening initiatives undertaken in Sweden showed a steep decrease in prevalence of chlamydial infections followed by decreasing incidence of reported PID and ectopic pregnancy.4,5 In the United States, annual screening of sexually active young women is recommended and screening programmes reduced prevalence in areas where this intervention has been in place for several years.6 In two randomised controlled trials, screening women reduced the risk of developing PID by half.7,8 Economic and human costs attributed to chlamydial infections are considerable. Modellers suggest that screening is cost saving if prevalence exceeds 3%9 and there is strong advocacy to scale up screening activities.10–14 However, the strength of the evidence surrounding the range of probabilities of sequelae of untreated asymptomatic infection is still limited, generating wide confidence intervals in cost effectiveness estimates15,16 and fuelling the discussion of whether Wilson and Jungner screening criteria for chlamydia are fulfilled completely.17,18
If a screening programme is considered on a national scale, insight into the burden of disease is required. High prevalence of up to 18% has been reported throughout Europe, but most studies have been conducted in STI clinics, youth clinics, sexual health clinics, or in selected general practices (“opportunistic screening”).19,20 Many studies focus on women, and are carried out in highly urbanised areas. Surprisingly, rural populations have rarely been the subject of study. Yet, unlike gonorrhoea and syphilis, which are usually found in well defined risk groups, chlamydial infection is more dispersed among young people in general. Novel approaches to the laboratory diagnosis of C trachomatis, like nucleic acid amplification tests (NAAT) using first void urine or vaginal swabs, created expanding opportunities for home based postal screening, targeting both women and men (“systematic” or home based screening).8,17,22 However in the Netherlands, population based data are not available except for the capital city of Amsterdam.
The routine implementation of a chlamydia screening programme is another critical issue. General practitioners (GPs) play a major role as providers of sexual healthcare in the Netherlands.21 Mainstreaming a new and large scale screening programme via GPs, who practise mainly curative care, is considered a major challenge.14 We investigated the feasibility of a screening programme organised not through general practice, but also by the Municipal Public Health Service (MHS), with referral of positive cases to the regular care providers. This paper describes the prevalence of chlamydial infection among 15–29 year old men and women in rural and urban areas and discusses the implications of this screening strategy for routine implementation.
METHODS
Population size and sampling method
The study population consisted of 21 000 men and women from the general population aged 15–29 years, stratified into three five year age groups. Sample size calculation was based on an expected prevalence in the general population of 3%, with a confidence interval of 1% around the expected prevalence for each age group separately, and a response rate of 50% for females and 33% for males.30 Because complications of chlamydial infection are found primarily in females, taking a larger sample of females increased statistical power.
The sample was stratified according to “area address density” (AAD). Statistics Netherlands divides every municipality in the Netherlands into one of the following five AAD categories: (1) very highly urbanised (>2500 addresses/km2); (2) highly urbanised (1500–2500 addresses/km2); (3) moderate urbanised (1000–1500 addresses/km2); (4) low urbanisation (500–1000 addresses/km2); and (5) rural (<500 addresses/km2). The total sample of 21 000 was divided over these five strata according to the distribution of these areas in the Netherlands. AAD categories 1 and 5 were oversampled because of an expected lower response rate in very highly urbanised areas and an expected lower prevalence in rural areas. The study took place in four non-randomly selected Public Health regions in different parts in the Netherlands. Study areas were selected purposively from MHS that were willing to participate in the study in a major city outside Amsterdam, and areas covering the north, south, and central part of the country. For each region it was decided which AAD categories would be included, taking into account the AAD profiles of the municipalities in each region, and an equal distribution of the total sample over the four regions. In every AAD category, a random sample was taken from the civil registration of the municipalities involved, with respect to the required number of females and males in each age group. In effect, the sampling procedure reflects a national probability sampling, including four regions of the country, which together are considered to reflect the general population of the Netherlands.
Screening procedure and specimen collection
Between September 2002 and March 2003 the selected people received a package by mail containing an introductory letter, an information leaflet on chlamydia, a urine sampling kit with instructions, a 18 item questionnaire concerning demographic characteristics (age, sex, education, ethnic group), sexual behaviour, symptoms of STI, and history of STI. The urine sample and questionnaire could be returned by mail in a postage paid plastic envelope to the central laboratory. All subjects, whether sexually active or not, were invited to participate; any person not wishing to participate could indicate this on a refusal card. Non-respondents received a reminder after six weeks. All participants received their test result by mail within three weeks. For people who tested positive, treatment of both the participant and partner(s) was provided through the regular services (GP or STI/MHS clinic). The study was approved by the medical ethics committee of the Free University Amsterdam, the Netherlands. Fifteen year old participants needed to add an informed consent form signed by their parent or guardian.
Diagnostics
Nucleic acid amplification tests, such as polymerase chain reaction (PCR), are currently advised for C trachomatis testing.23 As a pooling strategy was estimated to reduce the laboratory costs by half,24 urine samples were pooled by five (based on an expected prevalence of 3%) and tested for the presence of chlamydial DNA by means of polymerase chain reaction (PCR Roche Diagnostic Corp, Indianapolis, IN, USA). From positive pools (OD >0.8), all individual samples were tested to identify the C trachomatis positive person. Samples of pools in the grey zone (OD 0.2–0.8) and “inhibited” pools were retested individually by PCR. If an inhibited sample or a result in the grey zone could not be confirmed by dilution/specimen preparation and/or discrepant analysis, a new urine sample was asked from the participant. A positive result of both pool and individual specimen was labelled as a positive test. Results were communicated to the MHS, who in turn informed the participants by mail.
Treatment of cases
In case of a positive result, people were advised to be treated by a regular care provider, being GP or STI/MHS clinic. A letter was included to give to their care provider, containing information on the findings, current standard of care for treatment of index and partner(s), and a return slip for the MHS to monitor treatment. Upon arrival of the return slip with information on (partner) treatment, the GP received €22, the price of a standard consultation.
Non-response
Possible selection bias between participants and non-participants were studied in three different ways: (1) by comparing basic demographic variables from the civil registration available for all invited people (age, sex, residence, country of birth, and AAD) between participants (who returned urine and questionnaire) and non-participants (those who returned a refusal card and non-respondents); (2) by studying reasons for non-participation, as indicated on the refusal cards; and (3) by telephone interview with a structured questionnaire of a random sample of 700 non-respondents 12 weeks after the initial invitation. Contacted non-respondents were asked to answer questions about most important reason for non-response, demographic characteristics, sexual behaviour, symptoms of STI, and history of STI. People could stop this interview at each step. General and specific characteristics of this group were compared with those of the participants.
Statistical analysis
Analysis was performed with the SPSS package version 10.0 (SPSS Inc, Chicago, IL, USA). Prevalence rates were calculated with 95% confidence intervals. Adjusted prevalence rates were computed by using specific weights according to sex, age group, and AAD, calculated by inverse probability weighting25 based on national figures for 2002 as provided by Statistics Netherlands. Unless otherwise specified, weighted prevalence data are given.
Differences in characteristics between participants and non-responders were analysed using the χ2 or Fischer’s exact test. Associations between prevalence and several characteristics were assessed by univariate logistic regression analyses.
Role of funding source
The study was financed by a grant from ZonMw (the Netherlands Organisation for Health Research and Development), which has no commercial interest and had no role in study design, organisation of the study, and/or writing of the report.
RESULTS
Response rates
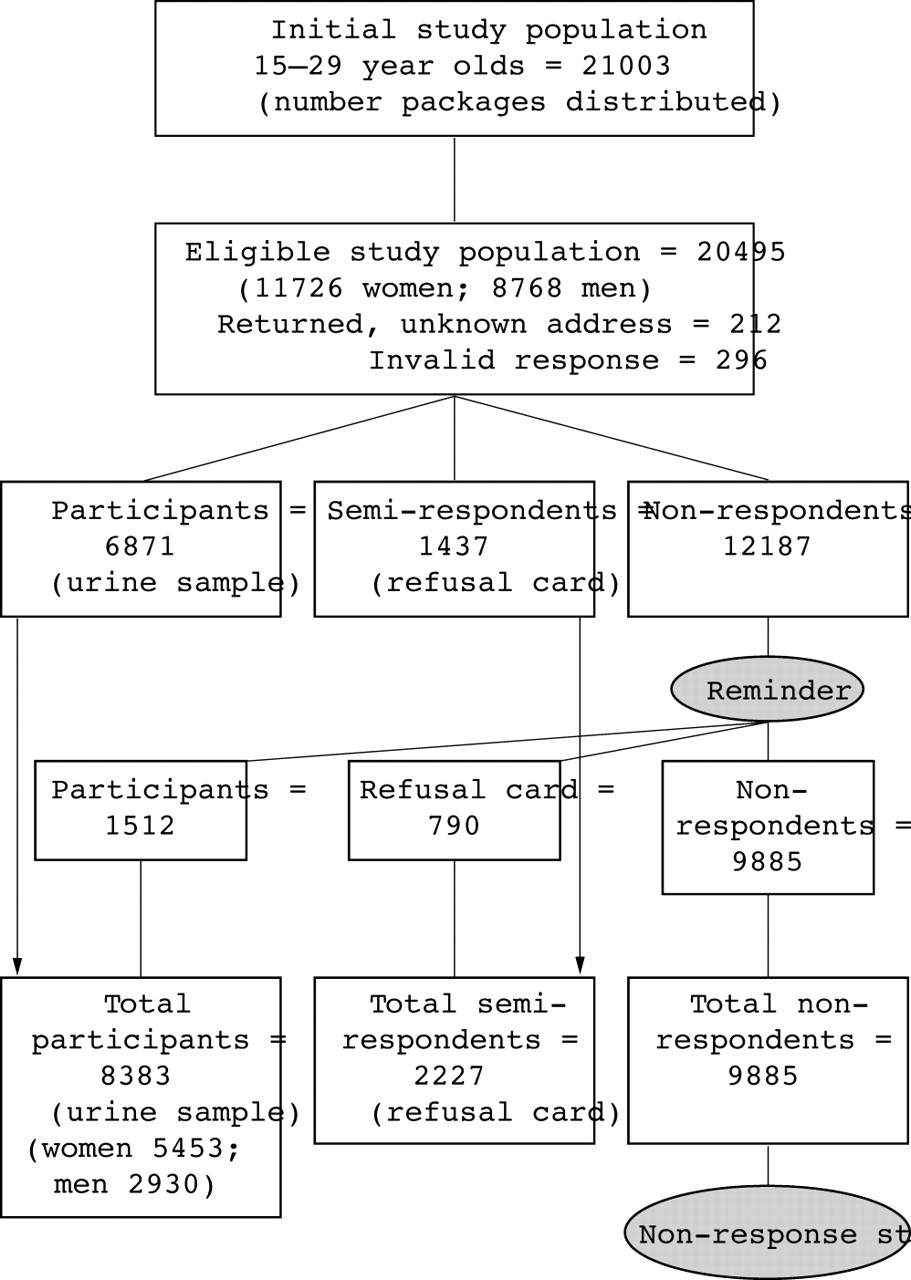
Of all 21 003 packages distributed, 212 (1%) were returned by post because of unknown address. These people were excluded from analysis. A further 296 participants (1.4%) were excluded because of invalid responses, mainly due to inconsistencies in age and sex as reported on the questionnaire and as documented in the civil registry. Of the 20 495 remaining people, 8383 sent in urine (41% participants), 2227 sent in a refusal card (11% refusals), and 9885 did not respond (48%) (fig 1). Participation was lowest in very highly urbanised areas (AAD 1, 37%; AAD range 1–5, 37%–46%; p<0.001). Reminders contributed 1512 of 8383 participants (18%). Women participated more often than men (47% v 33%; p<0.001). Participation was 38% in 15–19 year olds and 43% in 20–24 and 25–29 year olds (p<0.001). People born in the Netherlands participated more often than those born abroad (42% v 31%; p<0.001). Response rate among people born in Surinam was 32.5%, Antilles 30.1%, Turkey 25.8%, Morocco 22.9%, other countries 30.4%.

{kind=link}
Flowchart, PILOT CT study.
The reasons for non-participation mentioned on the refusal cards are given in table 1; 32% reported that the main reason was “never had sex”. Of the random sample of 700 non-responders, 410 could not be reached due to missing telephone numbers or no contact after five different attempts in three consecutive days in daytime and evening hours. Of the 290 remaining non-responders, 40% gave as main reason for non-participation no interest or no time. Two hundred and thirty eight were willing to answer the structured questionnaire in more detail. Compared with the participants, non-responders more often had an intermediate level of education. Non-responders reported fewer STI related symptoms (p<0.001) and reported “never had sex” more often (p = 0.002). Among sexually experienced non-responders, the number of lifetime partners was quite similar to the participants, but they reported less STI in the past and more condom use during their last act (table 2).
Main reason for non-participation among men and women as reported on refusal cards
Specific characteristics of participants and a subset of non-responders (non-response study)
Prevalence
Urine samples were available from 8383 respondents. Inhibition occurred in less than 0.5% of the samples. For 44 participants (0.5%), urine test results were not available (missing second urine sample in case of inhibition in the first sample or missing parental informed consent). Thus, prevalence was based on urine test results of 8339 participants. 165 tested positive. Adjusted prevalence did not differ much from the unweighted prevalence in our national probability sample. Overall (inverse probability weighted) prevalence was 2.0% (95% CI 1.7 to 2.3); higher in women (2.5% (2.0–3.0)) compared with men (1.5% (1.1–1.8)). Age group specific prevalence was 1.7% (1.2–2.2) in 15–19 year olds, 1.6% (1.1–2.1) in 20–24 years, and 2.5% (1.9–3.1) in 25–29 year olds. Prevalence was significantly lower in rural areas: (0.6% (0.1–1.1)) compared with very highly urbanised areas (3.2% (2.4–4.0)) (table 3). The highest prevalence was found in very highly urbanised areas in 15–19 year old women (4.3%) and in 25–29 year old men (4.1%). In all age groups, prevalence was higher among women compared with men.
Adjusted* chlamydia prevalence (%) according to age group, sex, and urbanisation (area address density)
In univariable logistic regression analysis prevalence was dependent of (high) urbanisation, (low) education, non-Dutch ethnicity (especially belonging to Surinamese or Antillean population), STI symptoms, and sexual behaviour (table 4). For sexually active participants we developed a risk factor model by multivariable logistic regression analysis. Degree of urbanisation, age group, ethnicity, education, symptoms (for women, postcoital bleeding; for men, frequent urination), no condom use at last sexual contact, number of sex partners, and recent partner change were independent risk factors. Prediction rules for selective screening could be developed (see p 24, this issue).38
Adjusted* chlamydia prevalence (%) among participants according to selected variables
Treatment
For 150/165 (91%) positive index cases, information that they were treated was available. Eighty two per cent of the 150 cases visited the GP; the others were treated by STI/MHS clinic. For all these cases, on the return slip was indicated that partner treatment was discussed.
DISCUSSION
This study is the first nationwide study in the Netherlands and internationally one of the largest population based studies, covering both women and men, and focussing not only on urban but also on rural populations. Fifty two per cent of those invited responded: 41% participated by returning urine and a questionnaire, and 11% returned a refusal card. The overall prevalence was 2%. A striking finding was the remarkably low chlamydia prevalence in rural areas (0.6%). In very highly urbanised areas the prevalence rate was 3.2% and participation 37%, compared with 44% in rural areas. We demonstrated that organising a home based screening through the MHS, referring screen positives to regular care providers, was feasible, and that 91% of screen positives were treated.
Remarkably, we found that the prevalence of chlamydia did not decline in those aged 25–29 years. This is consistent with the results of recent studies from Belgium and Finland.26,27 Chlamydia screening is considered for women aged 15–25 years because high prevalence is reported in this young age group. Although our finding might reflect persistent infections detected in a first screening round, epidemiological patterns may differ between and within countries and algorithms for age selective screening need local validation. The highest prevalence was found in very highly urbanised areas in 15–19 year old women (4.3%) and in 25–29 year old men (4.1%). Although women suffer the major burden of disease, evidence is growing that men need to be targeted as well, making them rather part of the solution instead of the problem.18,28
Even though our study was population and not clinic based, 26% of the participants reported possible STI related symptoms and chlamydia prevalence was significantly higher among them (4.0% v 1.4%; p<0.001). This warrants more attention to healthcare seeking behaviour and for diagnostic testing in primary care.
Prevalence was found to be dependent on sexual risk behaviour, but was also independently associated with other risk factors such as degree of urbanisation and ethnicity. Prevalence among Surinamese/Antillean women was as high as 12%—a finding in line with previous studies29,30 and reflecting sexual risk behaviour, mixing patterns, and background prevalence within sexual networks. We describe a prediction rule for selective screening in a separate paper.38 Further research on risk factors is warranted to determine prediction rules for selective screening that perform well in ongoing screening programmes based on prevalence.31
Limitations
One limitation of our study was the relatively low response rate. We did, however, collect demographic information on all non-respondents and details of sexual behaviour in a subset. We found evidence of participation bias that might influence our prevalence estimates in both directions. On one hand there was lower participation in people from minority ethnic groups and in highly urbanised areas, where prevalence was higher. On the other hand non-respondents reported fewer STI related symptoms, more frequent condom use, and were less likely to have a history of STI. This reflects the conflicting evidence about participation in screening programmes that high risk groups tend to decline screening, but on the other hand people make “informed” choices for non-participation if (they consider themselves) at lower risk. For instance, one third of the reasons mentioned on the refusal cards for not participating were “not being sexually active” or “having been tested recently”.
A second limitation is the fact that our study—like so many other published “screening” studies—was in fact a cross sectional prevalence study, at only one point in time. Response, participation of professionals, and prevalence is likely to change once screening becomes a routine programme. We reported that acceptability of future screening offered with regular intervals is significantly lower among screen negatives than in screen positives,32 suggesting that participation (of lower risk groups) would decrease in an ongoing programme. However, this limitation might be turned into a positive strategy, as has been proposed recently in screening for cardiovascular risk.33 Because many screening programmes harbour (negative) side effects, harms, and uncertainties,34,35 well informed choices can motivate those people to participate who are most likely to benefit. Thus, instead of perpetuating the public health imperative of maximising response, selective non-response in systematic screening based on informed choices may yield higher prevalence and offer client centred and more cost effective screening opportunities.
A third issue to be considered in screening studies is the use and possible abuse of screening tests. This issue was recently explored in depth.36 In low prevalence settings, even excellent tests have poor positive predictive value (PPV). The example was given of a “new” and excellent chlamydia test in a 3% prevalence setting, ending up with a PPV of 0.5, incorrectly labelling 50% of the positives. In our study we had chosen for a pooling strategy, a positive test result being based on two positive tests (a positive pool and a second positive sample). Further analysis of positive samples using another chlamydial genomic target (MOMP gene) showed that only two of 165 positive samples could not be confirmed with this different test. Thus, our testing strategy yielded a PPV of 0.99.
Pooling reduces cost substantially,24 but there is some concern that pooling might affect sensitivity and lead to a lower prevalence rate and untreated positives in the community. However, in contrast with pooling by 10, pooling by 5 (as we did in our study) appears to be as sensitive in identifying positive people compared with individual testing using the Roche PCR.39,40
Context and comparison
Internationally, our participation rates (women 47%, men 33%) compare favourably with the Danish in-home sampling (women 39%, men 27%)22 and the UK CLASS population based studies (women 34%, and men 25%),37 although higher prevalence rates are reported in these studies.
Our participation and prevalence rates in the very highly urbanised areas (AAD 1: response 42% in women and 30% in men, and a prevalence of 3.5% and 2.9% respectively) are similar to a previous systematic home based screening in the capital Amsterdam (AAD 1).30 In that survey, where the invitation letter and home sampling kit was sent by the GP, participation among 15–30 year olds was 47% in women and 30% in men, and prevalence 3.3% and 2.9% respectively.
In general, opportunistic screening has a higher yield than systematic screening. In an opportunistic screening pilot of women aged 16–24 years in the UK at venues such as family planning clinics, STI clinics, and general practices, prevalence ranged from 3.4%–17.6%, being approximately 9% in general practice.20 Opportunistic screening in several general practices in Amsterdam revealed a prevalence of 6.6% (15–29 year olds).29 Among sexually active women in Belgium, visiting their GP for routine gynaecological care, prevalence was 5%.26 If an opportunistic screening design is chosen, incorporating general practice is crucial, as impact on population prevalence will depend on reaching a substantial proportion of the at-risk population. Given financial constraints in healthcare, professional attitude and manpower deficiency in general practice, this is a major bottleneck. Organising prevalence based, selective chlamydia screening via the MHS, whose focus is on public health, is an alternative if cost effectiveness analysis proves to be favourable.
CONCLUSIONS
Population prevalence, also outside the big cities, is important to determine the burden of disease and to guide policy recommendations, especially if a new national programme is envisaged. We found very low prevalence rates in rural populations, suggesting targeted approaches and prioritising high risk areas in the enrolment of screening in the Netherlands. Our pilot study indicates that home based urine testing, organised by the MHS and in close cooperation with regular primary care providers for treatment of screen positives, is feasible, although participation problems clearly exist. There are still gaps in our knowledge regarding the issue of chlamydia screening and expanding the body of evidence is needed before a new nationwide screening programme is widely implemented in the Netherlands. Analysis of risk profiles and cost effectiveness will contribute to determining how selective screening can be used. Meanwhile more active case finding of chlamydial infections is warranted in high risk areas, in high risk groups, in cases of high risk sexual behaviour, and in cases of clinical suspicion (diagnostic testing).
Key messages
-
There is a lack of population based data for the development of policy recommendations for CT control. Most studies have been conducted in clinics related to sexual health or in selected general practices, mostly in (highly) urbanised areas. This limits the extent of evidence based recommendations for an entire country. This is the first population based study in the Netherlands on CT prevalence in both urban and rural areas.
-
Chlamydia prevalence among 15–29 year olds in very high urbanised areas was 3.2% compared to 0.6% in rural areas, suggesting that nationwide systematic screening is not indicated in the Netherlands and that targeted approaches are a better option.
-
In the Netherlands, GPs are the main providers of sexual healthcare. Implementing a new and large scale CT screening programme through GPs is considered a major challenge. We investigated the feasibility of a home based screening programme, organised by the Municipal Public Health Service (MHS), with referral of positive cases to primary care providers.
-
This pilot study indicates that home based urine testing, organised by the MHS and in close cooperation with regular primary care providers for the treatment of screen positives, is feasible.
CONTRIBUTORS
J E A M van Bergen was project leader, involved in conception, design, and organisation of the study, interpretation of data, and writing the first draft of the report. H M Götz, J H Richardus, C J P A Hoebe, J Broer, A J J Coenen, F de Groot, D T van Schaik, I K Veldhuijzen, and M J C Verhooren were all involved in conception, design, organisation, interpretation of the data, and drafting the final report. J H Richardus, I K Veldhuijzen, and H M Götz were responsible for statistical analysis. P J E Bindels provided feedback during implementation of the study, was involved in interpretation of data, critically reviewed the first draft, and assisted in the final report.
Acknowledgments
Professor P J E Bindels, A J P Boeke MD PhD, Professor J D F Habbema, J A R van den Hoek MD PhD, L Jacobi MSc, and S A Morré PhD were scientific advisors (scientific advisory board). This study was financed by a grant of ZonMw (the Netherlands Organisation for Health Research and Development).
REFERENCES
Footnotes
-
Conflict of interest: none declared
-
The PILOT CT study group are: J E A M van Bergen, J Broer, A J J Coenen, H M Götz, F de Groot, C J P A Hoebe, J H Richardus, D T van Schaik, I K Veldhuijzen, M Verhooren, Professor P J E Bindels.
Linked Articles
- Brief Encounters
- Chlamydia