Article Text

Abstract
Objective: To determine prospectively the relation between sexually transmitted infection (STI) diagnosis and depressive symptomatology.
Methods: Secondary data analyses were performed on 175 sexually active African-American female adolescents, who were recruited from high risk neighbourhoods in Birmingham, Alabama, United States.
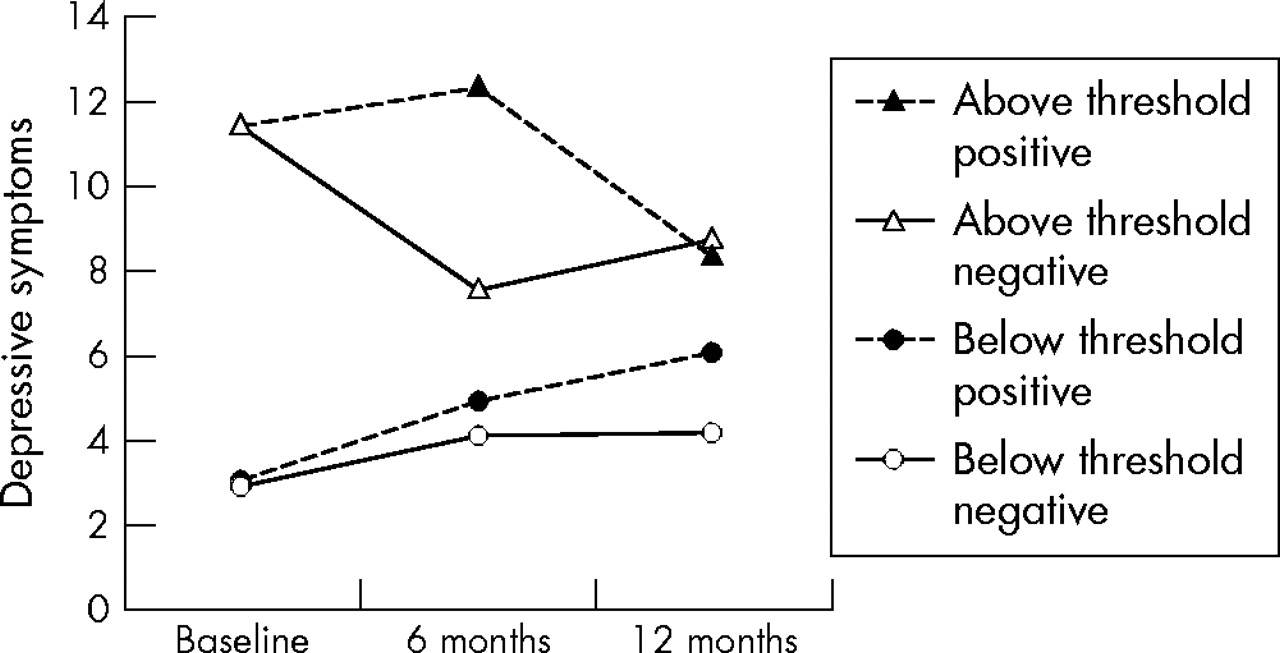
Results: ANCOVA was used to compare adolescents who tested positive with adolescents who tested negative on three waves of depressive symptom scores, controlling for age. The STI positive group had higher depressive symptom levels at 6 months relative to the STI negative group. This result was moderated by baseline depressive symptom levels: for adolescents above the clinical threshold, the STI negative group experienced a decrease in symptoms at 6 months whereas the STI positive group maintained the same level. For adolescents below the clinical threshold, there were no changes in depressive symptom levels regardless of diagnosis.
Conclusions: Receiving an STI diagnosis may affect depressive symptomatology for those at risk for depression. Screening for depression in settings that provide STI testing and treatment may be warranted for this population.
- ANCOVA, analysis of covariance
- CES-D, Center for Epidemiologic Studies-Depression Scale
- STI, sexually transmitted infection
- TANF, temporary assistance for needy families
- African-Americans
- adolescents
- sexually transmitted infections
- depression
Statistics from Altmetric.com
- ANCOVA, analysis of covariance
- CES-D, Center for Epidemiologic Studies-Depression Scale
- STI, sexually transmitted infection
- TANF, temporary assistance for needy families
Prevalence rates of depressive disorders in adolescents have been estimated to be between 15% and 20%, indicating depression is the most prevalent psychiatric disorder in the age group.1 Data also indicate that adolescent females experience disproportionate rates of depression relative to males,1–6 which may be attributable to changes in adolescent females’ bodies during puberty resulting in poor body image,5,7 cognitive predispositions,5,8,9 or the experience of more stressful life events.2,3,5 Further, socioeconomic status has been linked to depression among adolescents, suggesting that a minority of adolescent females may be at even greater risk for depression because of their marginalised socioeconomic status.3,6,10
The integrative theory of depression can be used as a framework to understand how these factors place adolescent females at heightened risk. The theory posits that an event occurs in a person’s life that leads to a heightened focus on self, which may result in changes to affective, cognitive, and/or behavioural structures. These transformations may subsequently act as precursors to dysphoria, thereby inducing a depressive episode.11 Investigators have examined the link between depressive illness and stressful life events such as divorce, loss, bereavement, natural disaster, child abuse, and victimisation.2,3,12–19 One specific clinical event, however, that may have a role in depression is the diagnosis of a sexually transmitted infection (STI). For some adolescents, particularly females, being diagnosed with an STI could have negative psychological sequelae such as shame, stigma, and self blame.20,21
One study has provided empirical evidence for a temporal relation between depressive symptoms and history of STI where depressive symptoms were an outcome of self reported STI among adolescent females.22 Although informative, the study involved self report of STI, which may limit the validity of the findings. Because depression has been linked to negative outcomes,3 and given the high prevalence and incidence of STIs among adolescents especially minority females,23 identifying an association between positive STI diagnosis and depression is critical. Accordingly, the goal of this study was to determine whether clinical diagnosis of an STI was associated with depressive symptomatology among a community sample of African-American female adolescents. We hypothesised that receiving a positive diagnosis would be associated with significantly higher depressive symptoms at a 6 month and 12 month follow up. We also explored whether baseline depression level moderated any hypothesised changes in depressive symptoms.
METHODS
Sample
The present study was initiated as a secondary study to a larger longitudinal research project that evaluated a sexual risk reduction intervention among female African-American adolescents. The sample was intended to represent a cross section of female adolescents residing in low income neighbourhoods of Birmingham, Alabama. Recruitment sites were selected based on this criterion and comprised an adolescent medicine clinic, four public health clinics, and health classes from five high schools that served lower income African-Americans.
Eligibility criteria included being a female African-American, 14–18 years of age, and reporting sexual activity in the previous 6 months. Of 1130 adolescents initially screened, 609 were eligible. The study achieved a participation rate of 86% with 522 adolescent females completing baseline assessments.
From the original sample at baseline (n = 522), a subsample (n = 271) was selected for the present study (see fig 1). The subsample comprised adolescent girls who were randomly assigned to the non-intervention comparison group. Baseline assessment of sociodemographic variables showed no discernable differences between groups. The rationale for using participants from the non-intervention condition was that the intervention curriculum conveyed knowledge about STIs, which could potentially influence depressive symptoms related to STI diagnosis. Additionally, because we were interested in documenting changes in depression over a 12 month time frame that were related to a specific event at baseline (that is, positive STI), we excluded adolescents who tested positive for any STI at the 6 month follow up (n = 57) and for whom data were missing (n = 39). Thus, our final sample size was 175. All participants were required to provide written informed consent. The study protocol was approved by University of Alabama’s institutional review board committee on human research before implementation.

Sampling procedure and participation rate.
Procedures
Project staff recruited adolescents from December 1996 through April 1999. All follow up assessments were completed by February 2001. Data collection was conducted at the family medicine clinic and consisted of a self administered survey, a face to face interview, and specimen collection. The self administered survey was conducted in a large room in which two chairs were placed between participants to assure confidentiality of responses. Two monitors stood at the front of the room and instructed participants to raise their hand if they needed assistance with the questions. Participants who raised their hand more than twice during the assessment were escorted to a private room where the monitor answered questions. Trained African-American female interviewers conducted the face to face interview, which assessed sexual risk behaviours, in private examination rooms. Adolescents were then asked to provide two self collected vaginal swabs. The first swab was placed in a specimen transport tube and evaluated for Chlamydia trachomatis and Neisseria gonorrhoeae by ligase chain reaction assay using DNA amplification technology (Abbott LCx Probe System). The second swab was used to inoculate culture medium for Trichomonas vaginalis (In Pouch TV test; BioMEd Diagnositics Inc, Santa Clara, CA, USA). This culture was incubated at 37°C and examined daily by light microscopy (magnification ×100) for 5 days for the presence of motile trichomonads. None of the adolescents refused to provide a vaginal swab.
After the initial assessment, participants returned 1 week later for the first session where they were informed of their STI results, and for those who tested positive, single dose drug therapy was provided. At the 6 month and 12 month follow up periods, adolescents were contacted and asked to return to the clinic and completed assessments identical to those at baseline.
Primary outcome measures
Depressive symptoms
The Center for Epidemiologic Studies-Depression Scale (CES-D) was developed for use in studies of depressive symptoms in general population samples.24 The original scale consists of 20 items that assess the presence of depressive symptoms during the past 7 days. The CES-D has been widely used with diverse populations of varying socioeconomic characteristics and has been shown to be valid for African-Americans.25,26 In this study we used a brief eight item version of the CES-D that had a four point response format ranging from 0 to 3.27 A total scale score was obtained by summing the numeric values for each item for a total score range of 0 to 24. The internal consistency of the scale with the present sample was 0.82. A CES-D score of seven or higher on the brief scale is the recommended indicator or “threshold” of depressive symptomatology.27 Adolescent participants whose scores were seven or higher may be at risk for depression. Several studies have reported a relation between the CES-D and clinical diagnoses of depression as well as with other diagnoses, such as anxiety disorder.28,29 Therefore, the CES-D is considered useful as a general screening instrument.
STI diagnosis
STI diagnosis was defined as testing positive to at least one of the following STIs: chlamydia, trichomoniasis, or gonorrhoea.
Covariates
Sociodemographic variables
Age, education level, family structure (that is, living arrangements), and receiving temporary assistance for needy families (TANF) were collected in the self administered questionnaire.
History of STI infection
Participants were asked during the personal interview whether they had ever been told that they had one of the following sexually transmitted infections: gonorrhoea, syphilis, chlamydia, herpes, genital warts, pelvic inflammatory disease, trichomoniasis, and crabs. If they indicated yes to any, then they were asked the number of times “ever” and “within the last 6 months.” They were also asked the number of times they received treatment for each STI.
Data analysis
Firstly, adolescents were categorised into one of two groups: those testing positive for an STI at baseline and those testing negative for an STI. These groups were compared on study and sociodemographic variables using parametric (t test) and non-parametric (χ2) analyses as appropriate. Results from these analyses were used to identify covariates in subsequent multivariate analyses. A two factor repeated measures analysis of covariance (ANCOVA) examined differences in depressive symptoms between groups at three time periods: baseline, 6 months, and 12 months. Univariate ANCOVAs were employed to determine at which time points groups differed. Several assumptions of the data were tested and found to meet statistical criteria for performing repeated measures ANCOVA.30 A second set of analyses was used to determine whether the hypothesised effect of STI diagnosis on depressive symptoms was moderated by baseline depression threshold level.
RESULTS
Sample characteristics
Participants ranged in age from 14–18 years (mean 15.8 (SD 1.18)). Most (93%) were in school. Slightly more than half (53%) stated that they lived with their mother, with 26% living with both parents, and 16% living with another relative. Some (19%) indicated that anyone they were currently living with was receiving public assistance, and the same percentage (19%) indicated that they currently held a paying job. The majority (85%) reported that they had never been told they had an STI.
At baseline, before STI diagnosis, 44% (n = 77) of participants were at or above the clinical threshold for depressive symptomatology (a composite score ⩾7) with a mean of 6.69 (SD 5.03). Overall, 27% (n = 48) of adolescents tested positive for at least one of the three STIs. Chlamydia was the most prevalent (17%), followed by trichomoniasis (13%), and gonorrhoea (3%). A small percentage of adolescents tested positive for multiple infections.
Comparisons between STI positive and STI negative groups at baseline
An analysis of baseline depressive symptomatology scores by STI diagnosis group showed no significant differences (p = 0.87) where 41% (n = 52) of participants who tested negative (n = 127) and 40% (n = 19) of participants who tested positive (n = 48) were at or above the threshold. Comparisons made between STI diagnosis groups on the baseline assessment of study variables and potential covariates showed significant differences for age (p = 0.003). Participants who received a positive diagnosis were slightly older. No differences were seen for education level, family structure, receiving TANF, or positive STI history (table 1).
Comparability of STI positive and STI negative groups at baseline
Trajectory of depressive symptoms by STI diagnosis
The results of the repeated measures ANCOVA, with age as a covariate, revealed a significant multivariate test (Pillai’s trace), F (2, 171) = 4.74, p = 0.01, indicating differences between groups on three waves of depressive symptoms. Mauchly’s test of sphericity was significant (p = 0.005), indicating appropriate adjustments were needed to the degrees of freedom for tests of significance. The adjusted tests supported the multivariate test and identified a significant within group interaction effect, F (1.896, 326.137) = 3.36, p = 0.039. Within subject main effect for time (p = 0.34) and between subject main effect for group (p = 0.13) were not supported.
Results for the univariate ANCOVA (controlling for age) showed that before STI diagnosis (at baseline), groups did not differ with respect to depressive symptoms, F (1, 172) = 0.08, p = 0.77. At 6 month follow up, controlling for age and baseline depression scores, the group who tested positive for at least one STI at baseline had significantly higher depressive symptoms than the group who tested negative, F (1, 171) = 10.36, p = 0.002. At 12 month follow up, the effects of STI diagnosis dissipated to the extent that there were no significant differences in depressive symptoms between groups (controlling for age, baseline, and 6 month depression scores), F (1, 170) = 0.63, p = 0.43. Adjusted means for the three time periods by STI diagnosis are presented in figure 2.

Depressive trajectories of African-American female adolescents by STI. Points represent adjusted mean depressive symptom levels: Baseline adjusted for age only; 6 months adjusted for age and baseline depressive symptom levels; 12 months adjusted for age, baseline depressive symptom levels, and 6 month depressive symptom levels.
Baseline depression as a moderator of STI diagnosis effect
Results for the repeated measures ANCOVA showed a significant multivariate three way interaction effect (Pillai’s trace), F (2, 169) = 4.58, p = 0.01, which was consistent with the within subject three way interaction effect (Greenhouse-Geisser), F (1.82, 310.148) = 4.382, p = 0.016 indicating that the effect of STI diagnosis on depressive symptoms over time depended upon baseline depression threshold level. To determine the nature of the interaction effect, several ANCOVAs were performed. Results of the ANCOVAs for the first group (below the threshold) indicated no significant main effect for STI diagnosis at baseline, (p = 0.90), 6 months (p = 033), or at 12 months (p = 0.080); however, for the second group (at or above the threshold), there was a significant main effect at 6 months, F (1, 73) = 13.07, p = 0.001, but not at baseline (p = 0.92) or at 12 months (p = 0.054). Adjusted means by STI diagnosis for both depression groups are presented in figure 3.

{kind=link}
{kind=link}
{kind=link}
Depressive trajectories of African-American female adolescents for negative STI diagnosis and positive STI diagnosis groups by baseline depression threshold level. Points represent adjusted mean depressive symptom levels: baseline adjusted for age only; 6 months adjusted for age and baseline depressive symptom levels; 12 months adjusted for age, baseline depressive symptom levels, and 6 month depressive symptom levels.
DISCUSSION
We found that overall having a biologically confirmed STI was associated with subsequent depressive symptoms among African-American female adolescents. Six months following a positive STI diagnosis, the female adolescents had significantly higher levels of depressive symptomatology compared with those who tested negative. Although these differences did not persist at the 12 month follow up, adolescents in the positive STI group, on average, still maintained high depressive symptom levels indicating a clinically significant trend.
Although we cannot determine causality, these results are consistent with previous research22 and provide support for depressive trajectories associated with STI diagnosis; however, these results must be viewed together with our results from subsequent analyses where baseline threshold depression level acted as a moderator of this effect. In other words, the effect of STI diagnosis on subsequent depressive symptomatology depends on whether adolescents were at or above the threshold for depression before receiving STI diagnosis. For those adolescents who were below the threshold, we found that STI diagnosis did not have a significant effect on depressive symptoms at 6 months or at 12 months. In contrast, for those adolescents who were at or above the threshold, a negative STI diagnosis was associated with an attenuation of depressive symptomatology at 6 months, whereas a positive STI diagnosis was associated with a continuance of clinical levels.
These findings hold implications for the integrative theory of depression, which posits a stressor such as receiving a positive diagnosis for an STI might lead to a depressive episode depending upon personal predisposing factors. Our results indicate that this conceptualisation of testing positive to an STI as a stressful life event that could elicit a depressive episode was not supported among this population. We found that receiving a positive diagnosis for one of three bacterial STIs did not necessarily lead to depressive symptoms nor exacerbate already present depressive symptoms; however, receiving a negative diagnosis was associated with an amelioration of symptoms. More research is needed that examines potential individual predisposing factors to depression among this population and how these factors may interact with having an STI.
Another important finding from this study is the proportion of adolescents, who before their diagnosis, had scores on the CES-D at or above the threshold (44%). The percentage of adolescents who were above the cut-off score is much higher than the rate in the general adolescent female population,3 and is consistent with the assertion that African-American adolescent girls are at an increased risk for depression. It is possible that the variability in prevalence rates between this study and others could be attributed to variation in stringency regarding threshold. Consequently, there may be a high number of false positives indicating the percentage at risk for depression could have been overestimated in this sample because of instrumentation. None the less, it is plausible that African-American adolescent girls residing in low income neighbourhoods may be exposed to other environmental stressors and represent a population at increased risk for depression.
Further compounding a potential heightened risk for depression is the high prevalence of STI among African-American adolescent females.23 In our study, 27% of adolescents tested positive for at least one of three bacterial STIs; a prevalence rate markedly greater than the general adolescent female population.31 Moreover, we found that those at or above the clinical threshold for depression at baseline maintained clinically high levels 6 months later (see fig 3). Taken together these two factors imply that disproportionately magnified depressive symptomatology may co-occur with disproportionately high rates of STI among African-American adolescent girls.
Routine screening for depression as a precursor or follow up to initial diagnosis may be warranted for this population for several reasons. Firstly, a heightened level of depressive symptoms coupled with a positive diagnosis may place female adolescents at an increased risk for subsequent STIs, acquiring HIV, or unintended pregnancy.32 Secondly, the morbidity and mortality costs of mental health problems such as depression are prohibitive.3 Also, depression may serve as a marker of other mental health problems related to having an STI (that is, low self esteem, poor body image). The CES-D short version can be easily incorporated into clinical protocols, either as a self administered instrument or interview during the intake procedure or comprehensive medical history. The clinical setting, therefore, represents an occasion for clinicians and healthcare providers to screen and treat not only for STI, but also for other indicators of mental health. At best, clinicians and healthcare providers could provide special attention to the manner in which adolescent females are informed of their STI diagnoses. Current CDC guidelines recommend clinicians and healthcare providers who counsel adolescents for STIs to receive basic training in prevention counselling.33
Although we found an association between diagnosis and depressive symptoms that was moderated by baseline depressive symptom levels, this study did not examine specifically the mechanism through which these phenomena occur. Clearly, more research is needed to better understand the links between having an STI and being informed of a positive STI diagnosis with subsequent effects on depressive symptomatology. It is difficult to determine from this study whether receiving the diagnosis was the contributing factor or some other related factor. The sample of African-American girls in this study reflect a group who are at risk for engaging in sexual risk behaviour and may also have other issues related to depressive symptomatology. For example, plausible explanations include the influence of other mediating variables (for example, the presence of other environmental stressors, sexual abuse, low self esteem, or substance use). Moreover, the overall clinical experience (that is, how the diagnosis is conveyed to the patient), feelings of stigma and shame associated with the disease, or psychosocial ramifications such as partner notification and perceived or real adverse partner reactions (that is, anger, violence) may have had some effect as well. Future studies should elucidate how some or all of these possibilities relate to depressive symptomatology within this population.
This study had a number of limitations. Firstly, this study was limited by the use of a self reported depressive symptom instrument (CES-D) versus the use of a clinical assessment instrument. The former is a screening tool that serves as an indicator of depressive symptomatology; it is not a substitute for a clinical diagnostic assessment of depressive disorder. Although the CES-D has shown adequate reliability when compared to clinical assessments of depression,28,29 we cannot exclude the possibility that the overall prevalence of depressive symptomatology may be significantly lower than described. Another issue may be generalisability, where these results may not be supported by other populations of adolescents. Also, generalisability may be affected because the analyses were secondary in nature and were conducted among a smaller subsample of girls comprising the non-intervention arm of a randomised, controlled trial. These results may also differ by type of STI. We tested for three treatable STIs, but the sample sizes were too small to test for differences by type of STI.
CONCLUSION
African-American female adolescents from low income neighbourhoods exhibit high prevalence rates of depressive symptomatology and STIs. This dual risk creates unique challenges for clinicians and healthcare providers who come into contact with this population, and also policy makers. As such, routine screening for depression as a precursor or follow up to STI diagnosis may be appropriate and necessary. Furthermore, the measured differences between STI diagnosis and subsequent depression levels may be explained by myriad factors present in their environment. Consequently, these results indicate future studies are needed to investigate the role of other psychosocial factors in explaining these measured differences in depressive symptoms as they relate to STI diagnosis.
Key messages
-
This study provides evidence to support a dual risk for STI and depression among female African-American adolescents
-
This study suggests that there is an association between positive STI and depressive symptomatology, which is moderated by previous depression level
-
The findings indicate that for adolescent African-American females who are below the clinical threshold for depression, there is no relation between STI diagnosis and depressive symptoms; for those who are above the threshold, a negative STI diagnosis was associated with an attenuation of depressive symptomatology, whereas a positive STI diagnosis was associated with the maintenance of clinical levels
-
The findings from this study should serve as a springboard for future studies to investigate the mechanism through which these associations occur
Acknowledgments
The authors thank Dr Jane R Schwebke for provision of cultures for Trichomonas vaginalis and Kim Smith MT (ASCP) for assistance and oversight of testing for Neisseria gonorrhoeae and Chlamydia trachomatis.
CONTRIBUTORS LFS, conceptualisation of research issues, development of the manuscript, synthesis of relevant literature, and data analysis; RJDiC, conceptualisation of research issues, development of the manuscript, and synthesis of relevant literature; GMW, conceptualisation of research issues and development of the manuscript; RAC, conceptualisation of research issues, development of the manuscript, synthesis of relevant literature, and data analysis; DLL, synthesis of relevant literature, development of the manuscript, and data analysis; KH, data collection, interviews, conceptualisation of the research issues, and development of the manuscript.
REFERENCES
Footnotes
-
This study was supported by a grant from the Center for Mental Health Research on AIDS, National Institute of Mental Health to the second author (1R01 MH54412).