Article Text

Abstract
Screening programmes to identify and treat young women with chlamydial infection have been developed in several countries. The goals of these screening programmes are, for the individual, to reduce a woman’s likelihood of experiencing important reproductive health complications, and, for the population, to reduce the incidence and prevalence of chlamydial infection in the population at risk. The primary objective of this commentary is to address whether we are losing ground in our efforts to prevent chlamydial infection and its complications.
Statistics from Altmetric.com
Screening programmes to identify and treat young women with chlamydial infection have been developed in several countries. The goals of these screening programs may be conceptualised at two complementary levels.1 For the individual, screening is intended to reduce a woman’s likelihood of experiencing important reproductive health complications, such as pelvic inflammatory diseases (PID), tubal infertility and ectopic pregnancy. For the population, screening programmes may reduce the incidence and prevalence of chlamydial infection in the population at risk. Reducing prevalence and incidence should also reduce transmission, preventing additional cases of reproductive complications.
How do we gauge the success or failure of a screening programme for chlamydial infection? Screening programmes should decrease the incidence of PID, infertility and ectopic pregnancy.2 Although randomised clinical trials suggest screening can be successful,3 demonstrating efficacy through surveillance is extremely challenging. PID, infertility and ectopic pregnancy have multiple potential aetiologies. Consequently, changes in rates over time may not be attributable solely to changes in the epidemiology of chlamydial infection.
At first glance, surveillance estimates of the prevalence and incidence of chlamydial infection appear to provide direct measures of the effectiveness of chlamydial screening programmes.4–7 Indeed, recent increases in the incidence and prevalence of chlamydial infection despite ongoing screening has raised questions about screening programmes’ effectiveness and the effects of screening on immunological responses.7 8 However, surveillance data must be interpreted cautiously. The primary objective of this commentary is to address whether we are losing ground in our efforts to prevent chlamydial infection and its complications.
DETERMINANTS OF INCIDENCE AND PREVALENCE
Unlike non-transmissible diseases, the incidence of infectious diseases is influenced by the prevalence of the disease.9 Because acquisition of Chlamydia requires contact with an infected sexual partner, the prevalence of chlamydial infection in the pool of potential partners is a key determinant of the incidence. If the partner is not infected, transmission is impossible. The incidence is also influenced by the rate of sexual partner change and other sexual behaviours, such as condom use. The duration of infection influences the likelihood of transmission and, thereby, also influences the incidence.9 Screening programmes, in theory, should reduce incidence through reductions in the duration of the infection. Similarly, prevalence is a function of the incidence and duration.10
For surveillance purposes, incidence and prevalence are often estimated through cases reported to a central health authority. The annual incidence rate and the prevalence are calculated as follows:


For estimation of the IR, the denominator is usually derived from census estimates of the population. In contrast, estimation of the prevalence is usually based on specific populations, such as women attending family planning clinics. In the calculation of the IR, it is not possible to distinguish from new cases and existing cases with routine surveillance data. In addition, clinic prevalence is often used as an estimate of population prevalence, a problem we will address below.
The observed IR and prevalence are influenced by several factors, creating uncertainty in these estimates. Potentially important biases affecting the estimates include reporting by clinicians, coverage of the population, case (or risk) mix of the population tested and the performance of the diagnostic tests used to identify cases. Healthcare seeking behaviour (who chooses to seek health care) will also influence the estimates over time. The magnitude of the bias associated with these factors can influence the IR and prevalence estimates differentially, so we will consider the IR and prevalence separately.
POTENTIAL BIAS IN THE ANNUAL INCIDENCE RATE
Reporting bias
Although reporting of chlamydial infection is mandated in each of the 50 US states, compliance with reporting is variable. Generally, private physicians may report less consistently than publicly funded clinics,11 causing underestimation of cases. Reporting bias may also distort rates in subpopulations. For example, racial/ethnic groups that are more likely to use publicly funded clinics will have more complete reporting than groups that use private physicians. This differential can exaggerate disparities in rates.
Reporting for chlamydial infection was not required in all 50 states and the District of Columbia until the year 2000.12 As of 1988, only 26 states required reporting.13 Although the denominators of calculated IR were adjusted to represent only the states reporting, as additional states required reporting, the observed prevalence and incidence would have changed over time simply because the rates in the new states were varied. Such changes could mask or exaggerate any true changes in national rates over time.
Coverage
Coverage is one of the most important factors responsible for an observed increase in the annual incidence rate of chlamydial infection. Coverage reflects the proportion of the population that is reached with screening activities. Because the incidence rate denominator is relatively constant, increases in coverage will generally lead to more cases being identified. Consequently, the observed IR increases. These observed increases may occur in the face of an unchanging, increasing or even declining true incidence rate.
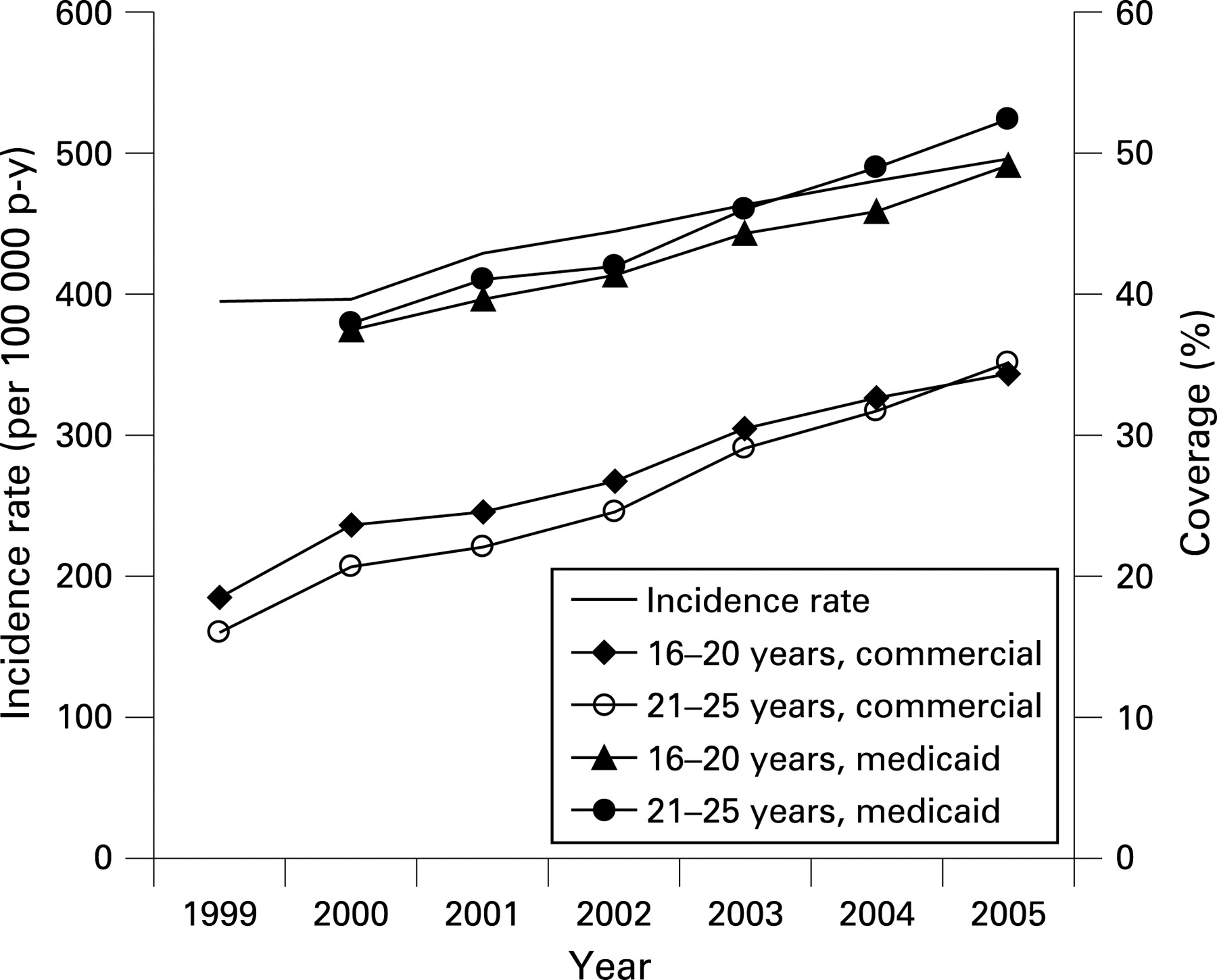
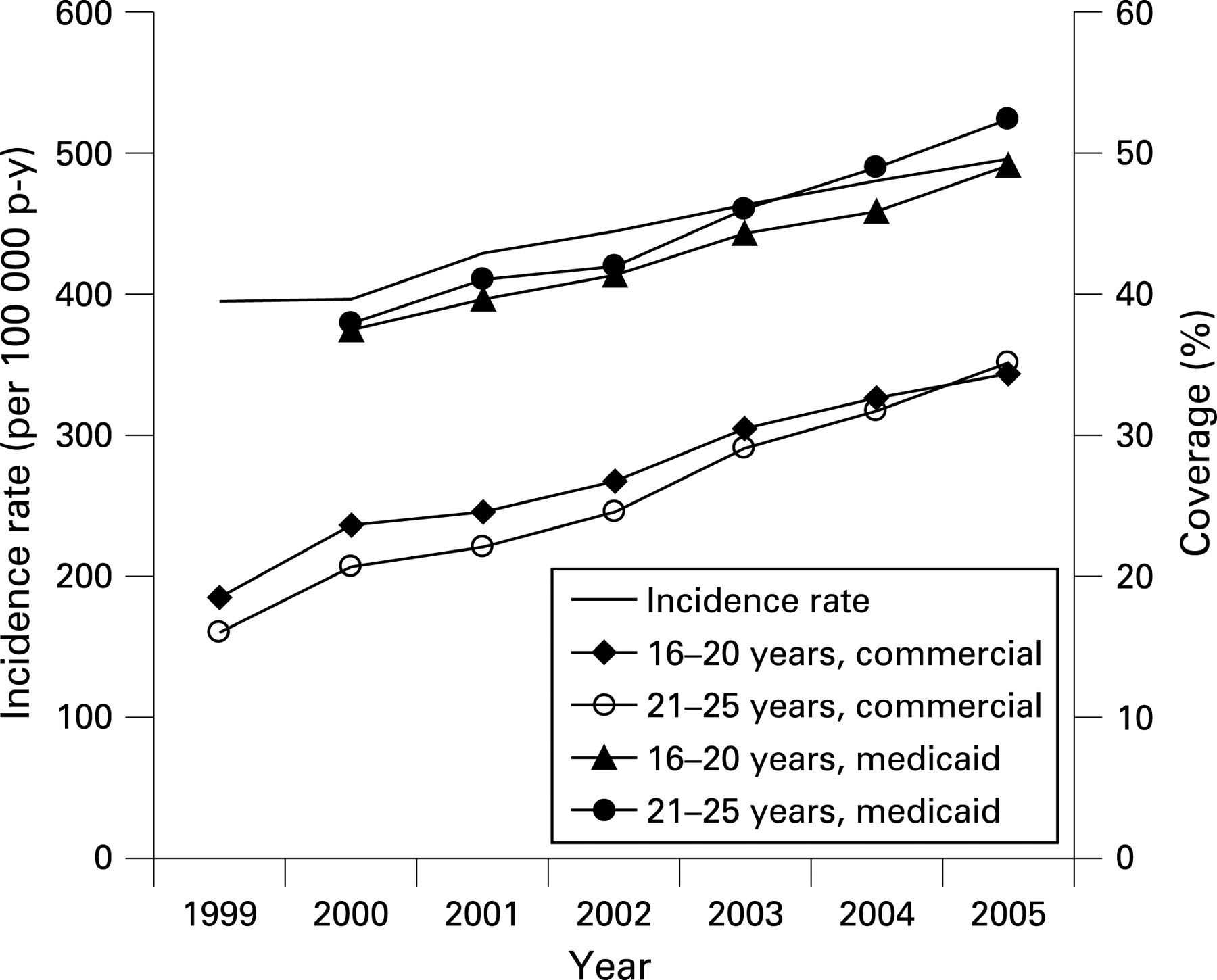
In 1999, screening for chlamydial infection in young women was included as a Healthcare Effectiveness Data and Information Set (HEDIS) measure for insurance companies in the USA.14 Consequently, coverage was monitored to assess the proportion of the population of young women who were tested for chlamydial infection. Comparing the reported coverage among Medicaid and privately insured women for the period 1999–2005 reveals a striking relationship (fig 1; data were obtained from14 15). The coverage and incidence rates rise in parallel. Using simple linear regression to investigate the relationships further, we see a strong and significant relationship with R2 values between 0.926 and 0.966 (corresponding to correlation coefficients of 0.962 to 0.983), indicating a large proportion of the variance in the IR is explained by coverage.
Case mix and diagnostic test performance
The risk-related composition of the population being tested, or case mix, and the diagnostic test accuracy can have substantial effects on the observed IR over time. As these effects are similar for the IR and prevalence, I will describe their potential influence in detail when discussing effects on prevalence.
POTENTIAL BIASES IN PREVALENCE ESTIMATES
Unlike the estimates of IR, prevalence estimates for surveillance purposes take the number of persons being tested into account. As a result, coverage does not directly influence the observed prevalence. However, the case mix, or the proportion of women at different risks, will affect the observed prevalence. Similarly, diagnostic test performance will also affect the observed prevalence.
Simulation methods
To demonstrate the effects of case mix and diagnostic test performance on the observed prevalence, a set of simple algebraic simulations were conducted using a hypothetical population of 30 000 women. This population comprised women in three age groups (n = 10 000 in each) with varying prevalences (age 16–20 years: prevalence = 10.0%; 21–25 years: prevalence = 4.0%; 26–30 years: prevalence = 1.0%). Given the high correlation of the risk of chlamydial infection with age, these three strata represent high, moderate and low risk. In all simulations, the overall true prevalence in the base population remained constant at 5.0%. To demonstrate the effect of case mix, the proportion of women being tested in three age categories was varied. In addition, the diagnostic test used to identify chlamydial infection was varied to simulate changes from culture to enzyme immunoassay (EIA) to nucleic acid amplification tests (NAATs).
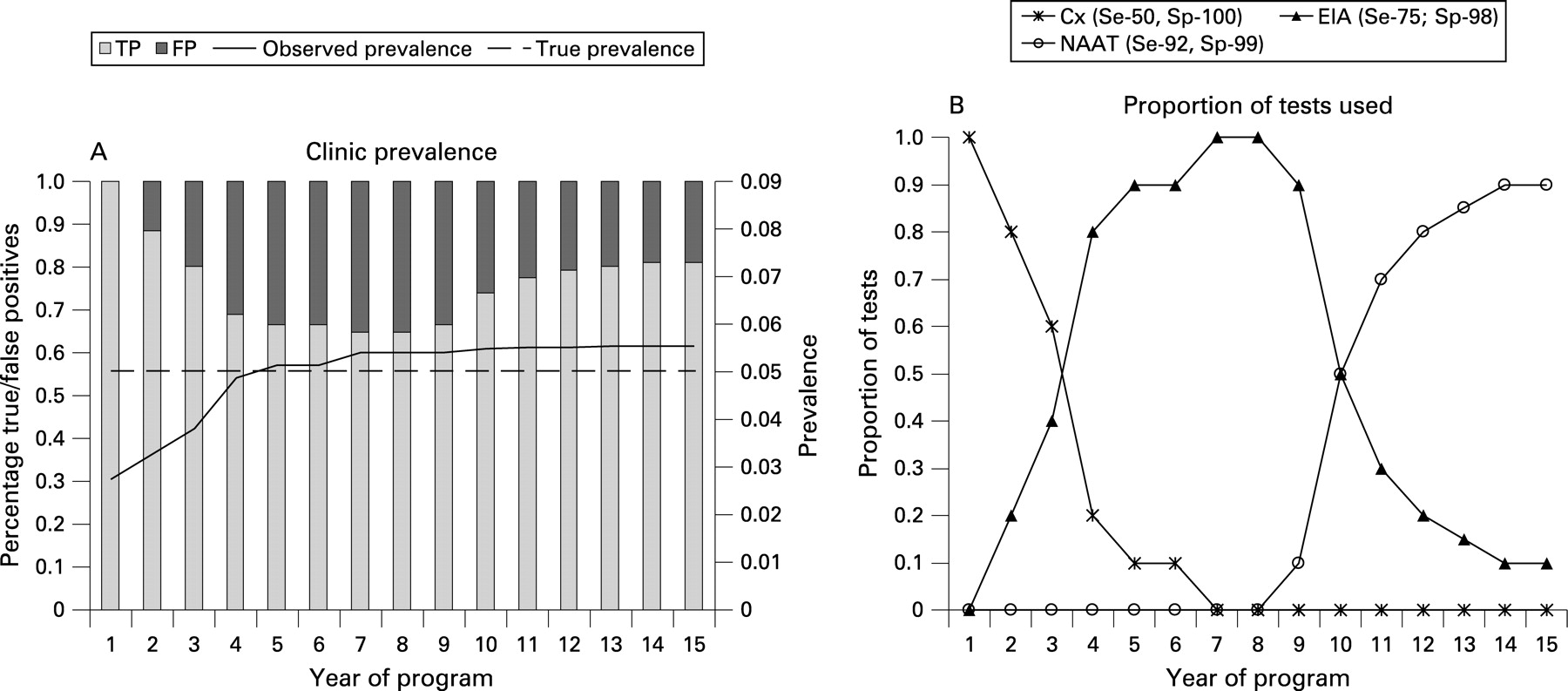
As the proportion of women at high versus low risk changes, the observed prevalence in the clinic population changes substantially (fig 2; panels A and B). In the early years of a hypothetical screening programme, relatively few women are screened (fig 2; panel B). In these initial years, the uptake of screening is rapid among the younger high risk women leading to an increase in the observed prevalence. As more moderate and low risk women are screened, the observed prevalence declines but remains above the true population prevalence (years 5–10). In the final years of the simulation, the number of women screened in the lowest risk (older) group is constant, while more high risk (younger) and moderate risk women are screened. Consequently, the observed prevalence increases slightly once again (fig 2; panel A).

Changes in the diagnostic test can also lead to changes in the observed prevalence over time. If a diagnostic test is imperfect, the observed prevalence will be a function of the sensitivity and specificity expressed with two equivalent expressions below:
Observed prevalence = (prevalence * sensitivity) + ((1-prevalence)*(1-specificity))
Observed prevalence = (true positives + false positives)/number tested
We can use this relationship to derive an algebraic correction formula for the prevalence when the test used is imperfect:
“True” or corrected prevalence = (observed prevalence + specificity −1)/(sensitivity + specificity −1)
Varying only diagnostic test performance and assuming all women in the base population are tested, the prevalence increases rapidly in the early years (fig 3; panel A) as sensitivity of the tests improves (fig 3; panel B), followed by a levelling off at a slight overestimate (fig 3; panel A). Note that the overestimation occurs because of the imperfect specificity of the diagnostic tests. For example, if the population with prevalence of 5% was tested with NAAT alone (sensitivity = 0.92; specificity = 0.99), the observed prevalence would be 5.6%, based on the formula given above.

Clearly, changes in case mix or diagnostic test utilisation are unlikely to occur in isolation. To demonstrate the potential effects of changes in both case mix and diagnostic tests over time, a joint simulation was constructed using conditions similar to each of the previous individual simulations (fig 4). In this scenario, once again, the observed prevalence rises rapidly. This rise is due to the change in diagnostic test, as well as the testing of the younger (high risk) population. In the middle years, switching to the enzyme immune assay (EIA) over time tempers the decline that was evident in the case mix example. The decline is less because the lower risk women are more likely to be false positives using the imperfect EIA allowing the observed prevalence to remain elevated. The final years of the programme demonstrate an overestimation due to the combined effects of the case mix (proportionately more young women) and the imperfect specificity of the diagnostic tests.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The influence of the diagnostic test, and especially specificity, becomes even more important if the prevalence is very low. At the extreme, if one considers a population with a true prevalence of 0, any positive test is a false positive. Thus, the observed prevalence directly reflects the specificity (observed prevalence = 1-specificity if true prevalence = 0). As the prevalence increases from 0, the influence of the specificity predominates at low prevalence, but the effect gradually decreases as the infection becomes more common. The specific value of the observed prevalence can be predicted from the formulas given above.
ALTERNATIVES TO CLINIC-BASED PREVALENCE ESTIMATES BASED ON SURVEILLANCE
Use of clinic-based surveillance estimates of prevalence is clearly limited by potential changes in case-mix and imperfect diagnostic tests. Although the bias associated with the diagnostic test can be accounted for algebraically, biases due to case mix, and the many other factors that influence healthcare seeking behaviour, are considerably more difficult to correct.
Population-based surveys are the strongest way to demonstrate whether a programme is having a population level impact. Population-based surveys do not require persons to seek health care and consequently are not subject to biases of case mix, yielding the best possible estimates of the prevalence in the general population. In the USA, estimates of the prevalence of chlamydial infection among women have been obtained in NHANES16 and The National Longitudinal Study of Adolescent Health (Add Health).17 These studies have revealed a prevalence of chlamydial infection of 4.7% in women aged 18–2517 and 4.6% among women aged 14–19 years.16 Unfortunately, to assess the impact of screening, repeated surveys are needed and these data are not available to date.
Although population-based surveys provide the best data available, they are not perfect. Surveys are susceptible to bias from the diagnostic test, just as with clinic-based estimates. However, as a single test is typically used for the survey, this bias can be accounted for in analyses.17 Surveys also are dependent on participation. Furthermore, some persons at highest risk for chlamydial infection may be less likely to be located or agree to participation. Finally, surveys are also expensive to implement and this expense can limit sample size and precision.
Prevalence can be monitored in “special” populations that are not actively seeking health care but are presenting for another purpose, such as a job programme or the military. An example of such an assessment is the routine screening of young women on entry to the Job Corps in the USA.18 Between 1990 and 1997, the prevalence in these women decreased from 14.9% to 10.0%.18 Between 1999 and 2005, the median state prevalence among women enrolling also declined (11.1% to 9.2%).15 These estimates of the prevalence over time may be slightly better than clinic-based estimates because the women are not presenting for health care. However, the potential biases are comparable to clinic-based estimates. Interpretation of these data requires careful identification of a target population, assessment of whether these women represent that target population and, finally, demonstration that the demographic and behavioural characteristics are stable over time.
ESTIMATING RATES OF REINFECTION
In addition to changes in the incidence rate and prevalence of chlamydial infection, reported rates of reinfection have increased in some settings.7 Reinfection represents women who have been screened or tested for chlamydial infection and then return after some period of time with another infection. The rise in reinfection has been hypothesised to be because of a reduction in the immune response brought about by the shortened duration of infection associated with screening.7 8 Although this hypothesis may have merit, estimating reinfection from routine data sources is problematic.
First, we must consider what is meant by the term “reinfection rate”. This term has occasionally been used to refer to the number of repeat infections (for example, second or third) divided by the population in the community.7 In other words, it is calculated like the annual incidence rate, but with the numerator, which usually reflects all cases replaced by those cases that are second infections. The problem with this formulation is that the denominator does not truly reflect the population at risk. When one considers “reinfections”, only those persons who have had a previous infection are at risk. If the denominator includes the entire population, the reinfection rate will increase simply because the number of persons previously diagnosed with chlamydial infection is increasing over time. In other words, the denominator is remaining relatively constant, but the pool of persons at risk for inclusion in the numerator is increasing.
Another uncertainty in the estimation of reinfection rates relates to undiagnosed infections. For example, a person with undiagnosed chlamydial infection may spontaneously clear their infection. If this person subsequently acquires a new infection and is diagnosed, the infection will be counted as a first infection even though it is actually a reinfection. As a consequence, if a screening programme is introduced into a population with a steady infection rate, the number of persons with reinfections will appear to increase because the pool of persons eligible to have a second infection is increasing as more first infections are diagnosed.
Finally, reinfection rates are difficult to assess from clinic data because follow up is not strictly controlled. A clinic setting is not a cohort study and persons may or may not return for subsequent testing. Changes in the proclivity of persons to return for subsequent evaluations will directly affect the observed rates of reinfection.
Testing frequency and incidence rates
As a final caution, it is important to recognise that testing frequency can influence observed incidence rates of overall infection or reinfection. In the simplest case, if we assume that a chlamydial infection would persist for about 1 year in a young woman,9 then testing and treating that woman’s infection during that year will give her the opportunity to be infected again. If she acquires another infection and the infection is detected, the incidence rate will increase, but this increase is brought about by her opportunity for infection created by the original screening and treatment. Because of the initial screening and treatment, followed by reinfection and repeat testing, she has contributed two cases rather than one.
IMPROVING SURVEILLANCE DATA
The best estimates of the prevalence of Chlamydia in the general population are based on repeated population-based surveys. In the USA, NHANES, an ongoing national survey, provides useful estimates, although the sample size in the appropriate age group is relatively small. Increasing the sample size among adolescents and young adults less than 30 years of age would improve precision of the estimates.
For clinic-based data, capturing the number of tests performed and the characteristics of the population tested would improve interpretation of IR and prevalence. Estimates could be presented in a format comparable to figs 2–4, and appropriately stratified and adjusted.
CONCLUSION
The premise of this debate was that national screening programmes might be causing a rise in chlamydial infection incidence, because of the potential effects on acquired immunity and resultant increased risk of reinfection.7 Determining whether we are losing ground in our prevention efforts is challenging using surveillance data, given the measurement issues described. However, one telling piece of information is the coverage of women eligible for screening. In the USA, the proportion of eligible women screened remains low—below 50%. Rises in the incidence rate correlate directly with rises in coverage (fig 1). However, despite the increases in coverage, I doubt that we are currently reaching enough women to have a substantial impact on the prevalence of chlamydial infection in the general population or the incidence of complications, especially given that men are not actively screened. In other words, I do not believe that our screening programmes have been successful enough to induce a reduction in acquired immunity. Rather, given our limited success to date, I believe we have much more ground to be gained.
REFERENCES
Footnotes
Competing interests: None.