Article Text

Abstract
Objectives: The number of cases of infectious syphilis is increasing rapidly across England and Wales. Concern has been expressed about diagnostic delay and its potential impact on patient care. A standard operating procedure for the serological diagnosis of syphilis has recently been developed by the Health Protection Agency. This study aimed to audit clinical and laboratory practice in England and Wales against this standard.
Methods: All microbiology departments, genitourinary medicine (GUM) clinics and antenatal clinics in England and Wales were invited to complete a web-based questionnaire.
Results: The overall response rate was 76%. Practices varied between laboratories. The proportion of microbiology departments performing enzyme immunoassay (EIA), Treponema pallidum particle agglutination assay/T pallidum haemagglutination assay, rapid plasma reagin/Venereal Disease Reference Laboratory and EIA IgM were 94%, 34%, 41% and 10%, respectively. Of these, 57% only perform a single screening assay. The turnaround time for negative results was less than 1 week for 84% of microbiology departments. For positive samples, turnaround times varied from less than 1 week to 6–8 weeks, with 19% of GUM clinics reporting turnaround times of over 3 weeks. Notably, 26% of GUM clinics and 6% of antenatal clinics reported that delays in turnaround time had adversely affected patient management in the past year.
Conclusion: This study suggests that there is significant room to improve laboratory turnaround times for the diagnosis of syphilis in England and Wales, and such improvements would be a positive step in limiting the spread of infection and of congenital syphilis.
Statistics from Altmetric.com
The number of cases of infectious syphilis is increasing rapidly across England and Wales.1 The recent epidemiology of syphilis has been partly driven by outbreaks in men who have sex with men and other at-risk populations, but occurs against a background of a general increase in the incidence of sexually transmitted infections.2–4 Syphilis is mainly a sexually transmitted infection, but due to the risk of vertical transmission, all pregnant women seen in antenatal clinics in England and Wales are offered a syphilis test.5–7
The increase in numbers of cases of syphilis has followed a period in the early 1990s in which very few positive cases were seen. At this time, many primary diagnostic laboratories provided only a single screening test, referring positive samples to the regional reference laboratory for further testing. Both clinicians and microbiologists have recently expressed concerns that this may lead to delays in providing patients and requesting clinicians with timely results, and may therefore adversely affect patient care as a result of delays in counselling, treatment and contact tracing. With well-documented difficulties in the management of syphilis both in genitourinary medicine (GUM) clinics8 as well as antenatal clinics,9 such delays need to be minimised as much as possible. A national standard method for the serological diagnosis of syphilis was developed in 2007 by the National Standards Working Group for Clinical Virology,10 with the aim of addressing these concerns by ensuring a minimum level of testing by primary laboratories and standardisation of the referral of samples to reference laboratories. There was previously no national standard operating procedure for the serological diagnosis of syphilis.
The laboratory diagnosis of syphilis is usually made by serology, although the direct detection of treponemes in material from lesions can also be accomplished by darkground microscopy (DGM) or PCR. Both antitreponemal and non-specific (cardiolipin) antibodies are produced during infection and both types of antibodies can be tested for. Treponemal antibody tests include enzyme immunoassays (EIA), the Treponema pallidum particle agglutination (TPPA) assay and the T pallidum haemagglutination (TPHA) assay. Non-treponemal tests include the rapid plasma reagin (RPR) and the Venereal Disease Reference Laboratory (VDRL) tests. These serological tests and their applications have been reviewed previously.11
The objective of this study was to describe syphilis testing in primary diagnostic laboratories in England and Wales in 2007, including the timeline of result reporting, the referral process to regional and reference laboratories, as well as the experience of users in GUM clinics and antenatal clinics. The implications of the findings are discussed and recommendations suggested.
METHODS
A web-based questionnaire was designed, which incorporated feedback from an initial consultation process. The questions required tick-box answers with space for free text for each response if needed. The questions that were asked of microbiology laboratories (fig 1) included the type of hospital, the volume of syphilis diagnosis performed in 2006, the tests used, the process of referral of samples, the time for issuing negative and positive results and whether or not delayed diagnosis had affected patient management in the past year. GUM and antenatal clinics were sent modified versions of the questionnaire, which included only the relevant questions for those settings.
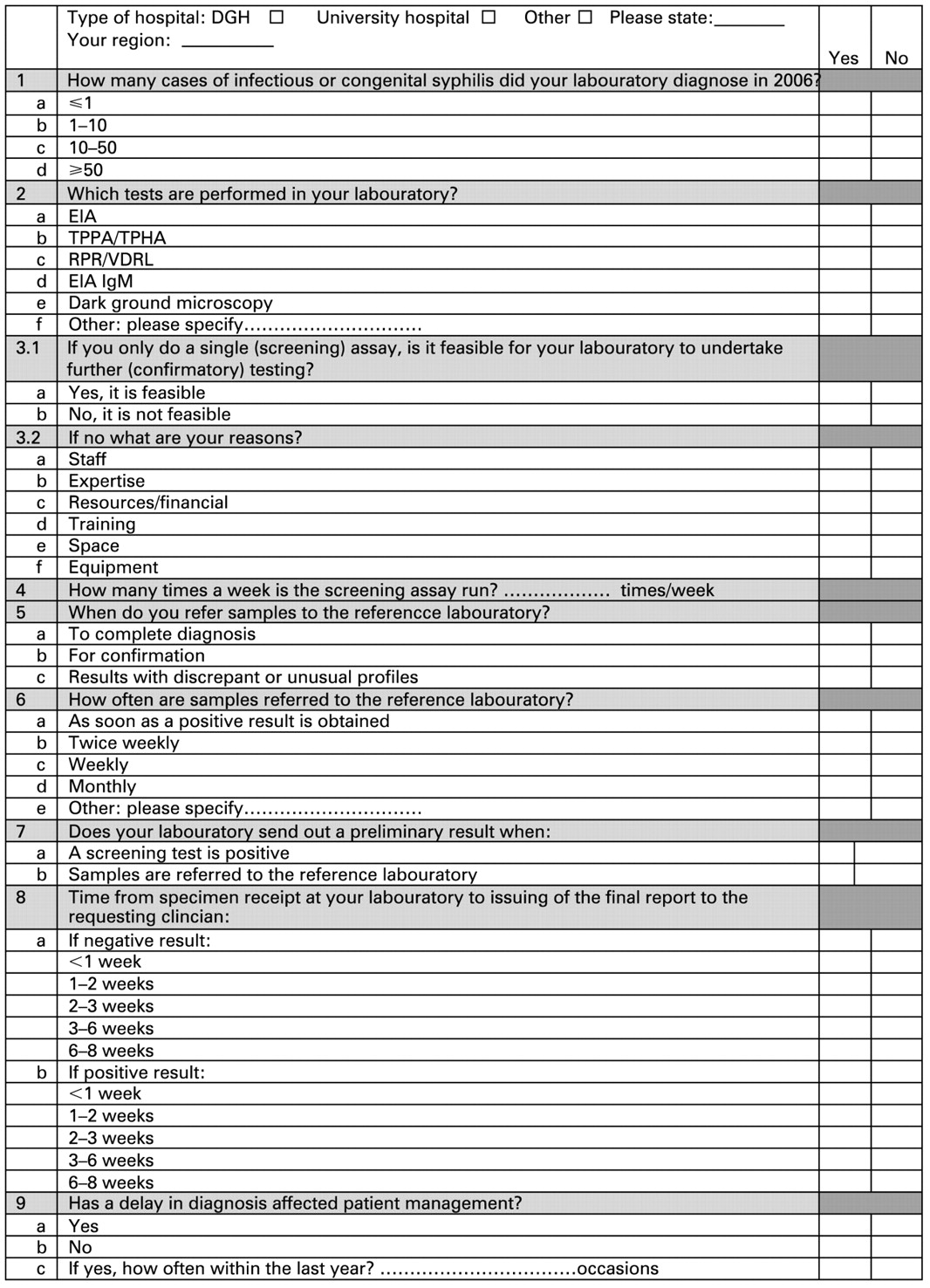
Audit questionnaire sent to microbiology laboratories.
A pilot study was performed in London, after which the lead consultant at all microbiology departments and GUM clinics and the screening coordinator for each antenatal clinic in England and Wales were invited to complete the questionnaires by the end of September 2007. An anonymous e-mail address was used (syphilis@hpa.org.uk) and data were collected automatically by the survey website, using survey monkey (http://www.surveymonkey.com/). Non-responders were sent a reminder e-mail in November 2007. They were asked to return a paper copy of the questionnaire as there had been some problems with the retrieval of data from the website. The deadline for the receipt of responses was extended to 31 January 2008, after which the results were extracted and analysed. All questionnaires that were returned were included in the results analysis, even if some questions had been left unanswered.
RESULTS
The overall response rate was 76%, with 66% (119/161) from microbiology laboratories, 69% (118/172) from GUM clinics and 83% (165/199) from antenatal clinics. Of the microbiology laboratories that responded, 18 did not perform any syphilis testing in-house, so only 101 laboratories were included in the analysis. Of these 101 respondents, 29 (29%) were from university teaching hospitals and 72 (71%) were from district general hospitals.
A total of 14 (14%) laboratories diagnosed more than 50 new cases of infectious or congenital syphilis in 2006, 35 (35%) diagnosed 11–50 and 36 (36%) diagnosed one to 10 cases. Five laboratories did not diagnose any cases of infectious or congenital syphilis in 2006. The remainder did not respond to this question or answered “not applicable”.
Responses from microbiology laboratories
The number of microbiology laboratories performing EIA, TPPA assay/TPHA assay, RPR/VDRL and EIA IgM were 95 (94%), 34 (34%), 41 (41%) and 10 (10%), respectively. These results are shown graphically in fig 2. DGM was performed in one (1%) microbiology laboratory. Fifty-eight of the laboratories (57%) only performed a single screening assay. The main reasons given for not being able to perform further testing included: resources or financial reasons (39 laboratories); staff (26 laboratories) and expertise (22 laboratories).

Tests performed in primary diagnostic laboratories. EIA, enzyme immunoassay; DGM, darkground microscopy; GUM, genitourinary medicine; RPR, rapid plasma reagin; TPHA, Treponema pallidum haemagglutination assay; TPPA, Treponema pallidum particle agglutination assay; VDRL, Venereal Disease Reference Laboratory.
There was considerable variation in the number of times per week that laboratories performed a run of the screening test, with 27 (27%) reporting that runs were performed daily, four (4%) reporting four times a week, 24 (24%) three times a week, 23 (23%) twice a week, 17 (17%) once a week and three (3%) as required.
The main reasons given for the referral of samples to a reference laboratory were: for confirmation (71 respondents, 70%); to complete the diagnosis (63 respondents, 62%) and for samples with discrepant or unusual result profiles (48 respondents, 48%). The majority of microbiology laboratories (70 respondents, 69%) reported referring samples to the reference laboratory as soon as a positive result was obtained, rather than batching samples before referral.
Only 57 (56%) laboratories reported that a preliminary result was issued when a screening assay was positive. Sixty-three (62%) laboratories issued a preliminary result when a sample was referred to the reference laboratory.
Responses from GUM and antenatal clinics
GUM clinics were asked which tests are performed by the primary laboratories that samples are sent to. The results were similar to those reported by the microbiology laboratories themselves, as shown in fig 2. DGM was performed in 40 (34%) GUM clinics.
There was considerable variation in reported turnaround times for both positive and negative results, which are summarised in fig 3. For both negative and positive results, microbiology laboratories generally reported shorter turnaround times than either GUM or antenatal clinics. For negative results, all laboratories reported turnaround times of less than 2 weeks, with 84% reporting turnaround times of less than 1 week. However, the majority of GUM and antenatal clinic respondents reported turnaround times longer than 1 week, with 24% of antenatal clinic respondents reporting times of more than 2 weeks. Turnaround times for positive results reported by laboratories were more varied, with 30 (30%) laboratories reporting turnaround times of 2–3 weeks and five (5%) reporting times of 3–6 weeks. This trend was even more noticeable in responses from GUM and antenatal clinics, with as many as one in five (22 respondents, 19%) GUM clinic respondents reporting turnaround times of more than 3 weeks.

{kind=link}
{kind=link}
{kind=link}
(A) Turnaround times for negative results. (B) Turnaround times for positive results. GUM, genitourinary medicine.
The occurrence of delays in diagnosis adversely affecting patient management are shown in table 1. As many as 31 (26%) GUM clinics, 10 (6%) antenatal clinics and four (4%) microbiology laboratories reported that delays in turnaround times had adversely affected patient management, with at least 33 such cases in GUM clinics and 12 in antenatal clinics.
Key messages
A standard operating procedure for the serological diagnosis of syphilis has recently been developed by the Health Protection Agency.
There is considerable variation in laboratory practice for the serological diagnosis of syphilis across England and Wales.
There is significant room to improve laboratory turnaround times for the diagnosis of syphilis in England and Wales.
DISCUSSION
The results provide some evidence to support the concerns that many laboratories do not yet provide the minimum testing recommended by the national standard operating procedure. At the time of this study, 57% of laboratories only provided a single screening assay, referring positive samples to a reference laboratory for further testing. Less than half (48%) of laboratories reported that samples with unusual or discrepant profiles were referred to a reference laboratory, whereas it is recommended that such samples should always be referred.
There was considerable variation in the turnaround times reported, particularly for positive results. Possible reasons that are suggested by the results include a variation in the frequency of screening assays performed by primary laboratories and a variation in the criteria for the referral of samples to the reference laboratory. Batching of samples for referral to a reference laboratory may be a significant cause of delay, as almost one third (31%) of laboratories reported doing this. It is of note that overall microbiology departments reported shorter turnaround times than their users. This may suggest that there are possible delays between the issuing of reports by the laboratory and the receipt of these reports by clinicians. However, with the use of electronic reporting, we would not have expected this factor to cause significant delays. Further local audits are needed to obtain a better understanding of the reasons for this.
Whatever the cause of these delays, it is worrying that as many as 19% of GUM clinics reported that positive results were received more than 3 weeks after a sample was taken. This delay may increase the risk of transmission of syphilis, through delays in the treatment of the patient, as well as in the identification and care of contacts. For surveillance and public health purposes, it may delay the identification and control measures for outbreaks.
Although this could deserve more in-depth case report review, it is concerning that as many as 26% of consultants responding from GUM clinics and 6% of the responders from antenatal clinics reported that patient management had been adversely affected by delayed diagnosis in the past year.
The results suggest that attention must be paid to optimising the process of syphilis diagnosis in England and Wales, both in terms of laboratory testing and in communicating results to clinics. It is to be hoped that improvements in diagnosis might assist in the control of syphilis transmission. A further audit is planned for early 2009, after implementation of the new national standard method VSOP4410 (http://www.hpa-standardmethods.org.uk/documents/vsop/pdf/vsop44.pdf) this year.
Acknowledgments
The authors would like to thank all microbiology laboratories, GUM clinics and antenatal clinics who participated in this study.
Footnotes
Competing interests: None.
Contributors: RJM and CAI initiated the study; AKA reviewed the literature and wrote the paper; RJM, CAI, HM, IG, JF and SHG contributed to the questionnaire design; AKA, RJM and RW organised the data collection and data management; IG and JF helped with data analyses; RJM closely supervised AKA; all commented on drafts; CAI, HM and SHG were indispensable in their support and promotion of the audit nationally.
Linked Articles
- Brief encounters