Article Text

Abstract
Background Given that the human papillomavirus (HPV) vaccine types have different durations of infectiousness and infectivity, the population-level vaccine effectiveness of these types may differ even if vaccine efficacy is identical.
Objective To compare the type-specific effectiveness of vaccination against HPV types 16, 18, 6 and 11.
Methods An individual-based stochastic model of HPV transmission (18 HPV-types) in a population stratified by age, gender and sexual activity was developed. Multiple parameter sets were identified by fitting the model to sexual behaviour data and age- and type-specific HPV prevalence.
Results Under base case assumptions (70% coverage, 99% vaccine efficacy per act and 20 years' duration of protection), vaccinating 12-year-old girls is predicted to reduce HPV-16, HPV-18 and HPV-6/11 prevalence by 61% (80% uncertainty interval (UI) 53–77), 92% (80% UI 65–100) and 100% (80% UI 97–100), respectively, 50 years after the start of the vaccination programme. Differences in type-specific vaccine effectiveness increased over time, and decreased with improved vaccine efficacy characteristics.
Conclusions For the same vaccine efficacy, the population-level impact of HPV vaccination will most likely be different, with HPV-16, the most oncogenic type, having the lowest effectiveness. These results should be taken into account when designing and interpreting post-vaccination surveillance studies.
- Human papillomavirus (HPV)
- vaccine
- mathematical model
- cervical cancer
- genital warts
Statistics from Altmetric.com
Introduction
Human papillomavirus (HPV) genotypes are classified as high oncogenic risk (HR) or low oncogenic risk (LR),1 according to their association with cervical cancer. Approximately 70% of cervical cancers can be attributed to HR types, HPV-16/18,1 and approximately 90% of genital warts are associated with LR types, HPV-6/11.2 Two prophylactic HPV vaccines are currently licensed in many countries across the world: the bivalent and quadrivalent vaccines that protect against types HPV-16/18 and HPV-16/18/6/11, respectively.
The potential for control and elimination of an infectious disease depends on (1) contact patterns between individuals, (2) infectivity/transmissibility, (3) duration of infectiousness and (4) duration of natural immunity.3 Pathogens with longer durations of infectiousness and/or higher transmissibility (ie, higher basic reproductive number, R0) are more difficult to eliminate and control through vaccination because they produce smaller herd immunity effects.3 Given that the duration of infection and transmission probability vary across the different HPV vaccine types,4 5 the population-level impact of vaccination against these types may be different even if vaccine efficacy is identical at an individual level. The aim of this study is to illustrate and compare the population-level impact of each vaccine type (ie, HPV-16, HPV-18, HPV-6 and HPV-11).
Methods
We used a stochastic individual-based transmission-dynamic model of sequential partnership formation and dissolution, and natural history of HPV.6 The modelled population is heterosexual, open and stable. Individuals are attributed two risk factors: gender and level of sexual activity. HPV transmission is assumed to be dependent on sexual behaviour, probability of transmission, duration of infectiousness and natural immunity. Eighteen HPV types are modelled individually, including types 16, 18, 6 and 11. These HPV types are assumed to be independent with respect to their natural history of infection and disease. For model predictions, we identified multiple parameter sets that fit simultaneously sexual behaviour data and HPV prevalence7–9 (details on the calibration method in Van de Velde et al6). Forty-four parameter sets produced results within the pre-specified targets of the data.6 Model predictions are based on these 44 parameter sets. Parameter uncertainty surrounding model predictions is presented as the median, 10th and 90th centiles of results from the posterior parameter sets, referred to as the 80% uncertainty intervals (80% UI). The median probability of transmission per act is estimated to be 0.7 (80% UI 0.5–0.9), 0.4 (80% UI 0.1–0.7) and 0.5 (80% UI 0.2–0.7) for HPV-16, HPV-18 and HPV-6/11, respectively. The median duration of infection for HPV-16, HPV-18 and HPV-6/11 is 12 months (80% UI 9–15), 9 months (80% UI 7–12) and 7 months (80% UI 5–8), respectively.
Results
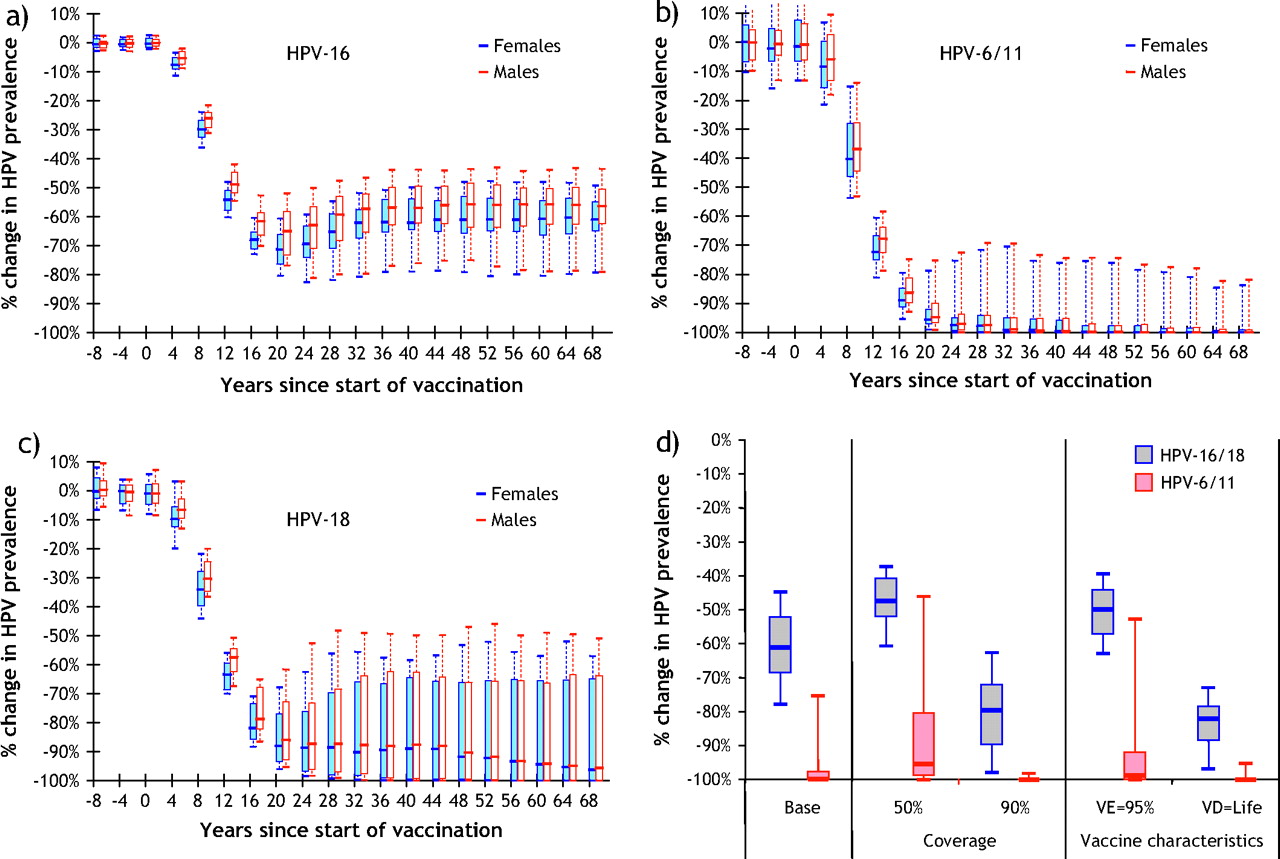
Model results suggest that HPV vaccination will lead to a rapid and significant decline in vaccine type-specific prevalence (figure 1A–C). Under baseline vaccine assumptions (coverage=70%, per-act vaccine efficacy=99%, duration of protection=20 years), vaccinating 12-year-old girls is predicted to reduce HPV-16, HPV-18, HPV-6/11 prevalence by 61% (80% UI 53–77), 92% (80% UI 65–100) and 100% (80% UI 97–100), respectively, 50 years after the start of the vaccination programme (figure 1A–C). These results clearly show that the type-specific vaccine effectiveness and the likelihood of elimination (ie, proportion of parameter sets predicting elimination) are significantly higher for HPV-6, 11 and HPV-18 than for HPV-16 (figure 1A–C). This is because HPV-16 has a higher probability of transmission and a lower clearance rate. Finally, differences in type-specific vaccine effectiveness increase over time and decrease with improved vaccine efficacy characteristics (figure 1D).
{kind=link}
Type-specific human papillomavirus (HPV) vaccine effectiveness. Estimated percentage change after vaccination in the prevalence of (A) HPV-16, (B) HPV-6/11 and (C) HPV-18, and (D) estimated percentage change in HPV type-specific prevalence 50 years after start of vaccination. Baseline vaccination assumptions: vaccination strategy=girls only, age at vaccination=12 years, vaccine coverage=70%, per-act vaccine efficacy (VE)=99%, vaccine duration (VD)=20 years. In the univariate sensitivity analyses, vaccine characteristics were varied one at a time, holding other parameter values at the baseline level. Box plots represent the medians, and 10, 25, 75 and 90 centiles of the predictions generated by the posterior parameter sets.
Discussion
Our model predictions have considerable uncertainty partly because data on type-specific duration of infectiousness and transmissibility are scarce, especially for HPV types 18, 6 and 11. Despite uncertainty in the precise value of our predictions and the relative impact of vaccination against the less prevalent types (eg, 18, 6 and 11), our main conclusion that the population-level vaccine effectiveness will vary across HPV vaccine types is robust as long as the duration of infectiousness and transmissibility/infectivity are sufficiently different across types and duration of natural immunity is similar. Our conclusion is also robust to variations in sexual behaviour between countries, although this may have an impact on the magnitude of the population-level effectiveness (ie, herd immunity effects).
A limitation of our analysis is that, although we model HPV-6 and 11 infections separately and fit our model to aggregated HPV-6/11 data, we assume that these types have the same probability of transmission and duration of infectiousness. Given that HPV-6 has a higher prevalence than HPV-11, our model may slightly overestimate the predicted effectiveness of vaccinating against HPV-6 and underestimate the impact against HPV-11. However, our overall conclusion remains robust given that HPV-6 and HPV-11 have a much shorter duration of infection4 than HPV-16 and therefore will most likely have a higher vaccine effectiveness. Finally, we purposely chose to examine the impact of vaccination on HPV infection rather than on HPV disease end points (eg, cancer). This was done to isolate the type-specific impact of vaccination without the additional uncertainty related to the natural history of disease and to have a common outcome for comparison.
Our results have important policy implications. Firstly, HPV-16, the type producing the greatest worldwide burden of HPV-related disease, will be the most difficult to control and eliminate through vaccination. Secondly, our results highlight the need for post-vaccination surveillance data stratified by HPV type. Given that pre-invasive cervical lesions and cancer occur decades after infection, HPV type-specific prevalence data are required to closely monitor trends in population-level effectiveness following HPV vaccination (eg, potential waning effectiveness). As genital warts occur shortly after HPV-6/11 infection, surveillance of genital warts has been suggested as a feasible and relatively inexpensive alternative to population-based HPV-typing studies.10 However, our results suggest that great care should be taken when using post-vaccination trends in HPV-6/11 as a proxy for HPV-16/18 effectiveness, as this may overestimate the impact of vaccination.
In summary, for the same vaccine efficacy, the population-level impact will probably be different for the HPV vaccine types because of their different natural history of infection. These results have important implications for the design and interpretation of surveillance studies.
Key messages
HPV types with longer durations of infectiousness and/or higher transmissibility will be more difficult to eliminate and control through vaccination.
Our model suggests that vaccine effectiveness will probably be higher for HPV-6/11/18 than for HPV-16, the type producing the greatest burden of HPV-related diseases.
Differences in vaccine effectiveness across HPV types are predicted to increase over time after vaccination and to be smaller with improved vaccine efficacy characteristics.
The use of HPV-6/11-related disease trends as a proxy for likely change in HPV-16/18 may be misleading.
Acknowledgments
We thank Dr E Franco for providing us with type-specific prevalence stratified by age and sexual activity from CCAST, BCCR and the McGill/Concordia cohorts. We also thank Dr M Drolet for comments on the manuscript. Finally, we thank the Imperial College High Performance Computing Service (HPC) for providing us with the computing power necessary to run the simulations.
Footnotes
Funding This work was supported by the Canada Research Chairs program (support for MB).
Competing interests MB was an employee of Merck Frosst Canada Ltd from 2003 to 2006. Since 2006, he has held a Canada Research Chair in Mathematical Modeling and Health Economics of Infectious Disease and is assistant professor at Laval University. He has consulted for Merck Frosst, and has received reimbursement for travel expenses from Merck Frosst and GlaxoSmithKline. NVdeV has no conflicts of interest to declare. M-CB has an unrestricted grant from Merck Frosst Canada Ltd.
Provenance and peer review Not commissioned; externally peer reviewed.