Article Text

Abstract
Objectives To determine the prevalence of pharyngeal and rectal Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) infections among men who have sex with men (MSM) in Germany and describe associations between these infections, sexual practices and other factors to provide an evidence base for screening recommendations.
Methods We conducted a cross-sectional study in 22 sentinel sites of sexually transmitted infections across Germany. Pharyngeal and rectal swabs were collected and tested for CT and NG with a nucleic acid amplification test (NAAT). Information on HIV status, number of sex partners and sexual practices was collected and linked to NAAT results.
Results Overall, 2247 MSM were screened for pharyngeal or rectal CT and NG infections; median age was 34 years (range 16–83). Prevalence of CT was 1.5% in pharyngeal and 8.0% in rectal specimens. Prevalence of NG was 5.5% in pharyngeal and 4.6% in rectal specimens. Local symptoms were reported in 5.1% of pharyngeal and 11.9% of rectal infections. Altogether 90.8% of rectal or pharyngeal infections would remain undetected if only symptomatic cases were tested. Rectal infection was significantly more likely in men reporting multiple partners (2–5 partners, OR=1.85; 6–10 partners, OR=2.10; >11 partners, OR=2.95), men diagnosed with HIV (OR=1.60) and men practising receptive anal intercourse without a condom (OR=1.54). Pharyngeal infection was more likely in men reporting multiple partners (6–10 partners, OR=2.88; >11 partners, OR=4.96), and men diagnosed with HIV (OR=1.78).
Conclusions Pharyngeal and rectal infections in sexually active MSM can remain undetected and thus transmissible if swabbing is not offered routinely. Screening should be offered particularly to MSM diagnosed with HIV and MSM reporting multiple partners.
- INFECTION
- SEXUAL HEALTH
- SCREENING
- HIV
- EPIDEMIOLOGY (GENERAL)
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) infections are the two most common bacterial sexually transmitted infections (STI) worldwide. Both infections are currently not reportable in Germany and national data on prevalence and incidence of these infections are limited.1
Since pharyngeal and rectal infections with CT and NG are often asymptomatic, they may remain undetected and serve as a reservoir for further spread.2–6 Furthermore, untreated NG infection might contribute to the development and transmission of antibiotic resistant NG.7 Additionally, since rectal and urethral CT and NG infections enhance HIV transmission and susceptibility, screening for these infections in populations at increased risk for HIV is warranted.3 ,8 ,9
Among men who have sex with men (MSM), particularly among men diagnosed with HIV, HIV serosorting is commonly used as a risk management approach.10–12 HIV serosorting, in combination with high numbers of partners, favours the spread of other STI.
Studies from Europe, North America and Australia report prevalence of pharyngeal CT and NG infection of 1–2% and 2–8%, respectively, and prevalence of rectal CT and NG infection of 6–9% and 2–7%, respectively among MSM.4 ,5 ,7 ,13–16 There are no systematically collected and published data about prevalence of rectal and pharyngeal CT and NG infection among MSM in Germany.
Testing for urethral infection reveals only up to 30% of all prevalent CT and NG infections in MSM.4 ,7 ,15 According to the existing evidence, strategies such as guidelines on STI screening and a computer alert on an electronic medical record increase screening rates for respective infections.17–18 Guidelines in Germany, last updated in the year 2000, suggest that individuals reporting oral or anal intercourse should be tested for rectal or pharyngeal CT and NG infections. However, in Germany, for men not complaining about suspect symptoms or not being directly referred as a sexual contact of a patient diagnosed with an infection, rectal, pharyngeal and urethral testing is currently not reimbursed by the health insurance companies. Furthermore, sexual history is rarely taken by primary healthcare providers.
Our aim was to determine the prevalence of pharyngeal and rectal CT and NG infections among MSM in Germany and describe associations between these infections, sexual practices and other factors in order to provide an evidence base for screening recommendations.
Methods
Study design
We conducted a cross-sectional study in 22 STI sentinel and MSM counselling sites in 16 cities across Germany between August 2009 and December 2010. The nationwide STI sentinel network consisted of local health offices, STI clinics and private practitioners.1 For the study we recruited a convenience sample of sites that are visited by MSM and had an interest to participate. The majority of these sites were community HIV and STI testing sites that are predominantly visited by HIV negative and untested persons. To measure factors associated with HIV status, we also contacted sites providing HIV care (n=7) to increase enrolment. Assuming that twice as many HIV-negative than HIV-positive persons will participate, with α=0.05, power 80%, and estimated prevalence of CT and NG of 5% among HIV-negative and 10% among HIV-positive persons, a study population of 341 HIV-positive and 682 HIV-negative participants was needed. Assuming that around one half of all questionnaires would provide a sufficient amount of information for further analysis, a total sample of 2046 was required.
MSM, who attended the study sites, were invited to participate regardless of symptoms. We included MSM who reported at least one male sexual partner within the previous 6 months, agreed to provide a rectal and/or pharyngeal swab and had not participated in the study before.
We collected information on demographics, sexual practices and symptoms by using a standardised self-administered questionnaire that was designed based on previous surveys in Germany and on questionnaires used by some of the study sites.19 Information on HIV status was either self-reported through the questionnaire or obtained from healthcare providers in the respective testing site. The healthcare provider either reported the result of HIV testing or the information from the case notes. For all participants with missing questionnaires, information on HIV status was acquired from the healthcare provider. Participants with self-reported or healthcare provider-reported positive HIV status were counted as HIV-positive. Other participants were counted as not known to be HIV-positive and included those with a recent HIV-negative test, those whose HIV test was not recent and those who had never been tested for HIV. All data were checked for plausibility and corrected, set to missing or excluded if corrections were not possible.
Rectal and pharyngeal specimens were collected and tested for CT and NG. The specimens were collected mainly by medical staff and in some cases by participants themselves according to standard procedures. Urine testing or taking of urethral swabs were optional and were performed by some of the sites in addition to the study protocol. If performed, results were reported. In addition, it was possible to undergo HIV testing, as routinely done.
The study protocol was approved by the ethical review committee of Charité University Hospital in Berlin. According to the protocol, written patient consent was taken, participation was voluntary, no personal identifiers were collected and no financial incentives were provided for the study participants or the study sites.
Laboratory procedures
All specimens were sent to Laboratoriumsmedizin Koeln, using APTIMA swab specimen transport tubes. The transport solutions in these tubes release the rRNA targets and protect them from degradation during storage. Specimens were then tested for CT and NG using a commercial nucleic acid amplification test based on transcription mediated amplification of a specific region of the 23S rRNA from CT (GenProbe APTIMA Combo2, GenProbe, San Diego, California, USA). CT and NG positives were confirmed using the CT and NG single analyte Aptima assays. A subsample of the CT-positive specimen was typed to distinguish lymphogranuloma venereum (LGV) subtypes (results published elsewhere).20
Statistical analysis
All data analyses were performed using Stata, V.12. We calculated prevalence together with 95% CIs of pharyngeal, recta, and urethral infections with CT and NG. For categorical variables we calculated frequencies and proportions. For continuous variables we calculated median and IQR. We used χ2 and the Wilcoxon–Mann–Whitney test to detect differences between groups, where applicable.
We determined the most frequent manifestations of CT or NG infection by analysing the subsample of those tested for all three infection sites—pharyngeal, rectal and urethral.
To describe factors associated with either pharyngeal or rectal infection, irrespective if it was caused by CT or NG infection, we performed a univariable and multivariable logistic regression analysis and calculated ORs. In the regression analysis we included data from participants who had filled in questionnaires and investigated the effect of age, number of sex partners, insertive and receptive anal intercourse with and without condoms, insertive and receptive oral intercourse, ejaculate in the mouth, passive and active anilingus, receptive and insertive fisting, and partner using saliva as lubricant on each of the two outcome variables—tested positive for rectal infection and tested positive for pharyngeal infection. Variables significantly associated with outcome at p<0.2 in univariable analysis were tested for association in multivariable analysis. The multivariable model was selected in forward stepwise fashion. Overall significance was set at p<0.05.
Results
Characteristics of study population
Overall 2247 MSM were included in the study; 1943 filled in a questionnaire, 2050 provided a rectal sample, 2197 a pharyngeal sample and 685 an additional urethral or urine sample. All three samples were available from 590 participants. Median age was 34 years (IQR 28–43). Among those who provided information to respective questions, 19% (355/1884) had migrated to Germany a median of 7 years ago (IQR 2–14). The majority of the study participants (85%, 1325/1552) had completed vocational training or higher education. Altogether 31% (692/2247) of the participants were HIV-positive; in 664 of these cases HIV infection was already known, and in 28 cases HIV infection was newly diagnosed.
Prevalence of pharyngeal and rectal CT and NG infections
Altogether, 6.7% (95% CI 5.6% to 7.7%) of pharyngeal and 11.6% (95% CI 10.2% to 13.0%) of rectal swabs tested positive for CT or NG infection. In the subsample of participants tested for urethral infection, 5.0% (95% CI 3.3% to 6.6%) tested positive. The prevalence of CT and NG infection by anatomical location is shown in table 1. Pharyngeal, rectal and urethral CT and NG co-infection was detected in 0.3%, 1.0% and 0.3% of the respective specimens.
Frequency and Prevalence of Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) infection by location
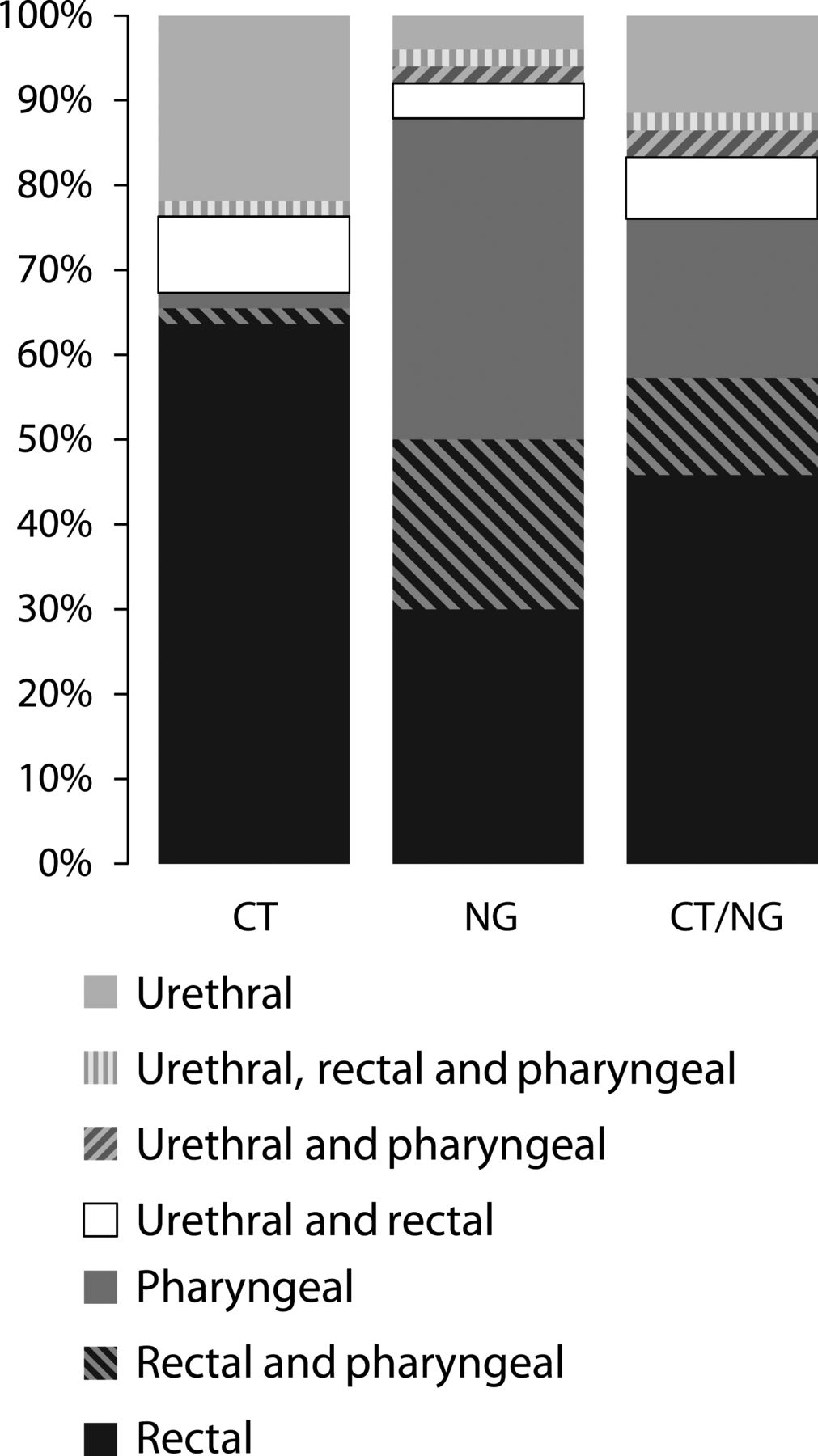
The CT or NG infection manifestations from the subgroup of participants tested at all three locations are shown in figure 1. Seventy-five per cent of CT infections were exclusively rectal. NG infections were in 30% exclusively rectal, in 38% exclusively pharyngeal, and in 20% rectal and pharyngeal co-manifestations. A rectal test alone would reveal 67% (64/96) of the infections, while a pharyngeal test would reveal 35% (34/96), and a urethral/urine test 24% (23/96) of the infections. A rectal and a pharyngeal test together would reveal 89% (85/96) of the prevalent infections.
{kind=link}
Manifestation of Chlamydia trachomatis (CT) (n=63) and Neisseria gonorrhoeae (NG) infections (n=49) in persons tested on all three locations (n=590).
Prevalence of local symptoms
The most frequently reported local pharyngeal symptoms were sore throat (65%), swollen mandibular glands (16%) and inflammation in the oral cavity (10%). The most frequently reported local rectal symptoms were itching (36%), anal discharge (17%), burning (13%), inflammation (11%), pain (11%) and redness of the skin around the anus (6%). The two most frequently reported urethral symptoms were burning (40%), mainly accompanied by urethral discharge (39%). Local symptoms possibly associated with infection, were reported only in 5.1% of pharyngeal, 11.9% of all rectal and 32.4% of all urethral infections. Presence of pharyngeal symptoms did not differ between those with pharyngeal infection and those tested negative (5.1% vs 3.0%, p=0.201), whereas local symptoms possibly associated with infection were reported more frequently by the participants tested positive than by those tested negative for rectal (11.9% vs 1.8%, p<0.001) and urethral (42.9% vs 4.8%, p<0.001) infection. Altogether 90.8% of rectal or pharyngeal CT or NG infections would have been missed if only participants reporting symptoms had been tested.
Number of sexual partners and sexual practices
Altogether 1826 participants provided information on the number of sex partners in the previous 6 months. The median number of male sex partners was 4 (IQR 2–10). Unprotected anal intercourse was reported with a median of 1 partner (IQR 1–2). Sex with female partners was reported by 6% (112/1826) of the respondents. Information on sexual practices with the last three partners within the last 6 months was provided by 1860 participants. Frequency of sexual practices together with number of sex partners stratified by HIV status is shown in table 2. Prevalence of CT and NG infection stratified by HIV status, number of sex partners and sexual practices is shown in supplementary table A. Information on condom use in oral intercourse was reported by 1107 participants. Oral intercourse was without condoms in 98% (1079/1197).
Frequency and proportion of number of sex partners, all reported sexual practices with up to three last partners in last 6 months by HIV status
Logistic regression analysis
The final model for rectal infection contained age, number of sex partners, receptive anal intercourse without condom, saliva as lubricant, and HIV status (table 3). The final model for pharyngeal infection contained age, number of sex partners and HIV status (table 3). Results of univariable and multivariable logistic regression are summarised in table 3. The associated factors did not differ significantly between CT and NG infection (analysis not shown).
Results of univariable and multivariable logistic regression for outcome
Discussion
This was the first multicentre study in Germany to investigate prevalence of pharyngeal and rectal CT and NG infections among MSM. We were able to identify a large number of infections that would have remained undiagnosed if testing were only based on the presence of symptoms, complaints or screening for urethral infection. The pharyngeal and rectal infection prevalence findings from our study are in line with data reported by other studies from Europe, North America and Australia.3–5 13–16 ,21
In a subsample of participants we were able to determine the most frequent manifestations of CT and NG infections. Urethral swabbing or urine testing would detect an insufficient proportion of prevalent infections. Rectal swabbing alone or in combination with pharyngeal screening would identify the majority of prevalent infections. Other studies confirm that among MSM, testing for urethral infections only reveals a minority of prevalent infections, and rectal manifestations are the most frequent.3–5 ,15 ,21
Rectal and pharyngeal CT and NG infections are frequently asymptomatic.3–5 ,14 Other studies report proportions of symptomatic rectal infections twice as high and symptomatic pharyngeal infections three to five times higher compared to our study.3 ,5 ,22 ,23 These differences can be explained by the differences in data collection. In our study we collected the data predominantly in settings visited by study participants primarily in order to test for HIV or receive routine HIV care, not to receive care for symptomatic STI. Furthermore, information on symptoms was collected via a self-administered questionnaire, in which participants were asked if they had symptoms, and in case they did, they were asked to report these symptoms in a free text format. The proportion of symptomatic patients was higher among those tested positive for LGV (results published elsewhere).20
Similarly to other studies we observed that rectal symptoms were reported more frequently by those with rectal infection than by those without, while the presence of symptoms did not differ between those with or without pharyngeal infection.3 ,5 ,22 ,23 In our setting a large proportion of infections would remain undetected if only those reporting any symptoms would be tested.
Pharyngeal symptoms, like sore throat, swollen glands, inflammation and changes in oral mucosa are common and very non-specific, and can be perceived differently by the patients themselves. Rectal symptoms, like itching, inflammation, burning, pain, redness of skin and mucus discharge are more specific, however less common, and can still be associated with a range of different diagnoses. In contrast to rectal and pharyngeal infection, urethral infections are much more likely to be symptomatic.3 Because of high rates of asymptomatic pharyngeal and rectal infections, and because most of the respective symptoms are non-specific, testing for pharyngeal and rectal CT and NG infections should be performed in all sexually active non-monogamous MSM, regardless of presence of symptoms.
We identified factors that were associated with higher odds to test positive for rectal or pharyngeal infection. For both manifestations increasing age was protective, while higher number of partners and positive HIV status increased the likelihood of being infected. Furthermore, those practising receptive anal intercourse without a condom also had higher odds for rectal infection. Interestingly, not remembering partner using saliva as lubricant was also associated with higher odds for rectal infection, while remembering partner using saliva was not associated in multivariable analysis. A possible explanation could be that those not remembering partner using saliva were also more likely not to remember (or not paying attention) whether a condom was used in receptive anal intercourse. Note, however, that this is applicable only to a small group of participants (6.5%). HIV status as an independent risk factor for pharyngeal and rectal infection could be either due to the increased prevalence of these infections in sexual networks of HIV-positive men, or due to increased susceptibility or infection persistence as a direct consequence of HIV-induced mucosal immune deficiency.3 ,8 ,10 Higher odds to be tested positive among younger men can be explained with behaviour factors, like higher number of sex partners and higher frequency of unsafe sex, as well as with higher prevalence of these infections among younger men.24–27 Younger age, higher numbers of sex partners, as well as HIV status are known risk factors for STI and are associated with high risk sexual behaviour.23–25 ,28 An association between pharyngeal infection and respective sexual practices, like receptive oral intercourse or active anilingus, has been reported in some studies.22 ,23 However, we, as in several other studies, did not detect such associations.29 We believe that this is due to differences in numbers of observations as well as the study designs.
Unprotected genito-anal and oro-anal sex was reported by at least half of the participants, while oro-genital sex was reported by more than 80% of the participants. Transmission is more likely per genito-anal than per oro-anal exposure.23 ,30 Oro-genital sex, however, is more often practised without a condom. Therefore, pharyngeal and rectal screening is important to identify and treat CT and NG infections among MSM.
Our analysis is restricted by several limitations. First, current HIV status was derived from self-report by the respondents or information was acquired from the healthcare provider. Therefore participants not known to be HIV-positive include those recently tested negative and those with unknown HIV status. Our finding that positive HIV status is associated with increased STI susceptibility could be due to the impact of either HIV infection on immunological susceptibility or HIV diagnosis on behaviour. If the first is true, lack of awareness of positive HIV status would result in an underestimation of the measure of association with HIV status— that is, in reality the association might be stronger as currently calculated.
Second, the analysis of the most frequent manifestations is restricted first by the smaller sample size of participants who in addition to pharyngeal and rectal swabbing were tested for urethral infection. Furthermore, we cannot rule out that the group of participants tested for urethral infections was more likely to be selected based on symptoms or reported sexual behaviours compared to the group of participants tested only for rectal or pharyngeal infection. This means that in our analysis the proportion of infections that can be diagnosed with urethral or urine testing may be overestimated.
Third, we cannot extrapolate our results to the total MSM population in Germany as we did not recruit a representative sample of the MSM population. As the total MSM population reached by all STI sentinel sites in Germany is unknown, we cannot extrapolate the proportion of the total MSM population visiting these sites reached in our study. Furthermore, as the STI sentinel and MSM counselling sites volunteered to participate in the study, the selected sites are not representative for the whole STI sentinel network. A selection bias was introduced by recruiting participants in HIV and STI testing sites, which may attract a part of the MSM population with increased sexual risk behaviour. Therefore, the prevalence of CT and NG infections might be overestimated. Due to insufficient information on non-respondents we were not able to compare respondents to non-respondents. However, this limitation does not restrict our results regarding the most frequent manifestations or association analysis. On the contrary, our study demonstrates how many undiagnosed infections could be diagnosed and treated if rectal and pharyngeal screening were to be introduced in Germany.
We conclude that a substantial proportion of rectal and pharyngeal CT and NG infections in sexually active MSM remain undetected in the absence of rectal and pharyngeal swabbing. Screening for pharyngeal and rectal infections is particularly indicated for HIV-positive MSM and those who had multiple partners in the months before the screening visit. We recommend offering pharyngeal and rectal screening for CT and NG as part of comprehensive routine STI screening for MSM. The STI testing guidelines and reimbursement rules for diagnostic procedures in Germany should be adopted accordingly.
Key messages
-
A substantial proportion of Chlamydia trachomatis and Neisseria gonorrhoeae infections in sexually active men who have sex with men (MSM) remain undetected in the absence of rectal and pharyngeal swabbing.
-
Screening for pharyngeal and rectal infections should be part of a comprehensive routine sexually transmitted infections (STI) screening for MSM.
-
Screening is particularly important for HIV-positive MSM.
-
The STI testing guidelines and reimbursement rules for diagnostic procedures in Germany should be adopted accordingly.
Acknowledgments
We thank the members of the PARIS (Pharyngeal And Rectal Infection Screening) study group for conducting data collection: Anja Potthoff, Bochum; Aspasia Manos, Leipzig; Gisela Hanf, Nürnberg; Norbert Kellermann, Nürnberg; Petra Spornraft-Ragaller, Dresden; Andreas Klein, Dortmund; Ruth Hörnle, Berlin; Karin Rittner, Braunschweig; Kathrin Graefe, Hamburg; Gisela Walter, Hamburg; Esther Voigt, Köln; Vera Pawassarat, Kiel; Heiko Jessen, Berlin; Carmen Zedlack, Berlin; Werner Becker, München; Corinna Becker, Bremerhaven; Manuela Buttelmann, Bremerhaven; Felix Laue, Köln; Marc Grenz, Hamburg; Gaby Knecht, Frankfurt am Main; Gert Hartmann, München; Peter Wiesel, Berlin; Heribert Knechten, Aachen; Petra Panstruga, Aachen; Albert Mayer, Böblingen; Florian Zinke, Mannheim; Torben Schultes, Nürnberg.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Handling editor Jackie Cassell
-
Contributors SDV, KH, HW and UM collaborated in the writing of the manuscript. SDV, KH, AS and UM were involved in the design and conducting of the study. HW and FW performed laboratory procedures and provided laboratory results. SDV and UM performed statistical analysis of the study. SDV, KH, AS, HW, FW and UM revised the manuscript before submission, and complemented it with contextual data.
-
Funding This work was supported by the research funds of the Robert Koch Institute. Test kits for detection of Chlamydia trachomatis and Neisseria gonorrhoea infection were provided free of charge by the manufacturer.
-
Competing interests None.
-
Ethics approval Ethical review committee of Charité University Hospital in Berlin.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement A subsample (from shorter time frame and not including all specimens) of the specimens tested positive to Chlamydia trachomatis was further genotyped. Genotyping data were analysed separately by author collective from Robert Koch Institute.