Article Text

Abstract
Objective To determine the diagnostic accuracy of tests developed for use at the point of care for Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG) and syphilis in women having symptoms of lower urinary tract infection.
Methods Cross-sectional study involving sexually active 14–49-year-old women with lower urinary tract infection symptoms consulting during 2010 at a private health clinic and at two public hospitals in Bogotá, Colombia. Pregnant women, those with a previous hysterectomy or those who received antibiotics during the previous 7 days were excluded. Sequential sampling was used; sample size: 1500 women. The ACON NG and CT duo test combo and the ACON individual test plates for NG and separately for CT were used. The QuickVue Chlamydia rapid test (RT) was also used. All of them were compared with nucleic acid amplification methods. The SD Bioline 3.0 and ACON test for syphilis were evaluated and compared with serological tests. Sensitivity and specificity were estimated.
Results CT RTs had a sensitivity that ranged between 22.7% and 37.7% and specificity between 99.3% and 100%. Sensitivity for NG with ACON Duo was 12.5% and specificity 99.8%. Tests for syphilis had a sensitivity of 91.6–100% and a specificity of 99.7–97.8%.
Conclusions The RTs studied are not useful for screening for NG at the point of care. In case of CT a recommendation about their use in routine care should be supported by a cost-effectiveness analysis. In screening populations at high risk of sexually transmitted infections or pregnant women, the RTs for syphilis should be used.
- CHLAMYDIA TRACHOMATIS
- DIAGNOSIS
- NEISSERIA GONORRHOEA
- SYPHILIS
- TESTING
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG) and Treponema pallidum (TP) are infections importantly affecting women in low income and middle income countries. WHO estimated that worldwide prevalence in 2008 in adults between 15 years and 49 years was: 100.4 million cases for CT, 36.4 million for NG and 36.4 million for syphilis.1 Prevention, early diagnosis and suitable management of cases and contacts must be ensured for reducing the burden from sexually transmitted infections (STIs) globally.2 In Colombia the National Institute of Health reported in 2000 an incidence of STI other than HIV, of 70 cases per 100 000 inhabitants, mainly caused by NG (31.8 per 100 000 inhabitants).3 A study using PCR techniques in women aged 15–24 years, in 10 areas of 4 continents, reported that Colombia had the second highest prevalence of CT, 7.2% (95% CI 4.4% to 10.9%) and the fourth highest prevalence of NG.4 The rate of syphilis in Colombia was estimated at 7.1 per 100 000 in 2006.5
Nucleic acid amplification tests (NAATs) are currently used for detection of CT and NG on cervical swabs. A sensitivity of 88.6% for CT6 and 91.3% for NG has been reported for NAAT, in cervical swabs.7 NAAT tests are costly and require laboratories that have advanced technology; on the other hand the gold standard for syphilis is based on non-treponemal (Venereal Disease Research Laboratory, rapid plasma reagin (RPR)) and treponemal (Treponema pallidum particle agglutination, Treponema pallidum haemagglutination assay (TPHA)) tests.2 All of these tests require a second clinic appointment for patients to inform the results and to prescribe therapy.8 Given that CT and NG infections are often asymptomatic,9 or their symptoms and signs are non-specific with frequent presence of other STIs, there is growing interest in using rapid tests (RTs) at the point of care (POC) site to have a result available during the consultation, as they could improve performance of syndromic diagnosis.10
The diagnostic performance of RTs for CT and NG has shown inconsistent results. Accuracy varies depending on the type of population being studied (high risk vs low risk for STIs),9 the setting where the RTs are done, infection prevalence, the type of pathogen to be detected and the diagnostic technology being used.10
The aim of this study was to determine the diagnostic accuracy of commercially available POC rapid diagnostic tests for CT, NG and syphilis in women having symptoms of lower urinary tract infection (LUTI), compared with NAAT for CT and NG and non-treponemal and treponemal tests for syphilis.
Materials and methods
This is a planned secondary analysis of a study to evaluate the use of syndromic diagnosis of LUTIs.11 The design was a cross-sectional study involving sexually active women aged between 14 years and 49 years, having LUTI symptoms, such as vaginal discharge, foul odour or itching, who consulted at a private sexual and reproductive health clinic (PROFAMILIA) and at the ambulatory services of two public general hospitals: Engativá and Fontibón Hospitals, in Bogotá, Colombia, during 2010. The institutions were selected by convenience, as they care for women seeking care in the public sector (hospitals) and the private clinic as it belongs to the best private organisation providing sexual and reproductive health services to the general population in Colombia. Pregnant women, those suffering medical conditions requiring hospitalisation, those hysterectomised or those who had received systemic or local antibiotic treatment for the urinary tract during the previous 7 days, were excluded. To estimate the sample size in the main study, a prevalence of 2% for NG was assumed, therefore in order to have at least 30 positives cases for NG infection a sample size of 1500 participants was estimated. This prevalence of NG was assumed based on the lack of up to date data on the frequency of NG infection in the international literature. With this number of patients would be included the necessary sample size for evaluating the RT accuracy for syphilis and CT infection, according to the available data of their prevalence in Colombia for syphilis 7% (sample size 98 patients) and for CT 6% (sample size 72 patients)12 Consecutive sampling was used. Due to non-availability of all the RTs for the total population during the study, three different diagnostic tests for CT and two for NG were used sequentially, depending on availability.
Procedure
At each site, a previously trained nurse interviewed women fulfilling the inclusion criteria, obtained signed informed consent and completed a structured interview. Sociodemographic variables investigated were: age, socioeconomic level, education level, type of healthcare system and marital status. A general practitioner (GP), evaluated the associated symptomatology, performed gynaecological examination and took samples using an unlubricated disposable speculum. The physician was experienced in the use of syndromic management of urinary tract infections.
Three endocervical samples were obtained:
The first endocervical sample was used to perform PCR with the COBAS AMPLICOR CT/NG system (Roche). These samples were transported in the AMPLICOR (specimen transport medium) transport medium to the Bogotá District Public Health Reference Laboratory, where one certified bacteriologist performed the analysis following the manufacturer's recommendations within the next 10 days.
The second sample was for a RT for NG (NG ACON Plate test or ACON NG and CT Duo test combo (ACON Laboratories, San Diego, California, USA)).
The third sample was for a RT for CT (ACON Plate CT RT or QuickVue Chlamydia RT (Quidel Corporation, San Diego, California, USA)). When the Duo test combo was used, only two samples were necessary.
A blood sample (5 mL) was obtained from the antecubital vein for the rapid syphilis tests at the laboratory of each centre. The study did not use finger prick because a sample was also taken for HIV testing, and for non-treponemal tests (RPR); in this sense any additional puncture could represent extra discomfort for the participant. The instructions of the RTs included total blood or serum for the procedure. The ACON syphilis ultra RT (ACON Laboratories, San Diego, California, USA) and the SD Bioline syphilis 3.0 RT (Standard Diagnostics, South Korea) were used in all participants. These are immunochromatographic assays for qualitative detection of antibodies against TP.
Once the samples were obtained, the GP established a syndromic diagnosis and provided treatment when appropriate, according to recommendations of WHO.13 The GP was blinded to the results of the RTs.
The NG and CT samples were transported immediately to the laboratory of each centre, in the dry tube provided by the manufacturer. The RTs were processed into the immunoassay device by a trained bacteriologist and interpreted (following manufacturer's indications) within 10 min of sampling. The bacteriologists were blinded to the clinical diagnosis. A result was interpreted as being positive when two lines appeared, one in the control region band (C) and the other in the test region band (T), and as being invalid when the control line could not be observed.
For amplifying nucleic acids, CP24 and CP27 primers (around 207 nucleotides long), were used for CT and SS01, and SS02 primers (about 201 nucleotides long) for NG, included in the AMPLICOR CT/NG system. Amplified DNA was hybridised and detected by colorimetry. Absorbance values at 660 nm used for interpretation were: ≥2.0 being confirmatory for CT and ≥3.5 for NG. Samples having inhibited or inconclusive results were repeated; if such result persisted the sample was excluded from analysis. The bacteriologists performing confirmatory tests were blinded to the POC test results.
Syphilis: The serum obtained by centrifugation was used for the two syphilis tests studied. The ACON RT was processed at the laboratory of each site following the recommendations of the manufacturer. The remaining serum sample was refrigerated and sent to the reference laboratory, where it was frozen. The frozen serum was thawed and used for the RPR test within the next 8 days. The Bioline syphilis test was performed at the end of the recruitment, following the manufacturer's recommendations. The syphilis RPR test (Human Gesellschaft für Biochemica und Diagnostica mbH, Wiesbaden, Germany) was initially used for diagnosing syphilis and the TPHA test (Human Gesellschaft für Biochemica und Diagnostica mbH, Wiesbaden, Germany) for confirming all reactive samples. All tests were carried out following the manufacturer's recommendations. A reactive RPR result ≥1:2 dilution plus a positive TPHA was considered diagnostic for active syphilis, a non-reactive RPR/positive TPHA was considered as treated or resolved syphilis, and a reactive RPR/negative TPHA was considered as a false positive result.
Analysis
Descriptive statistics were used for the analysis of data collected during the interview. Results are reported as specific prevalence of infection and diagnostic performance characteristics of RTs. STATA V.9.0 software (Texas, USA) was used for statistical analysis. Sensitivity, specificity and respective 95% CIs, and positive and negative likelihood ratios (LRs) were estimated for each test.
Results
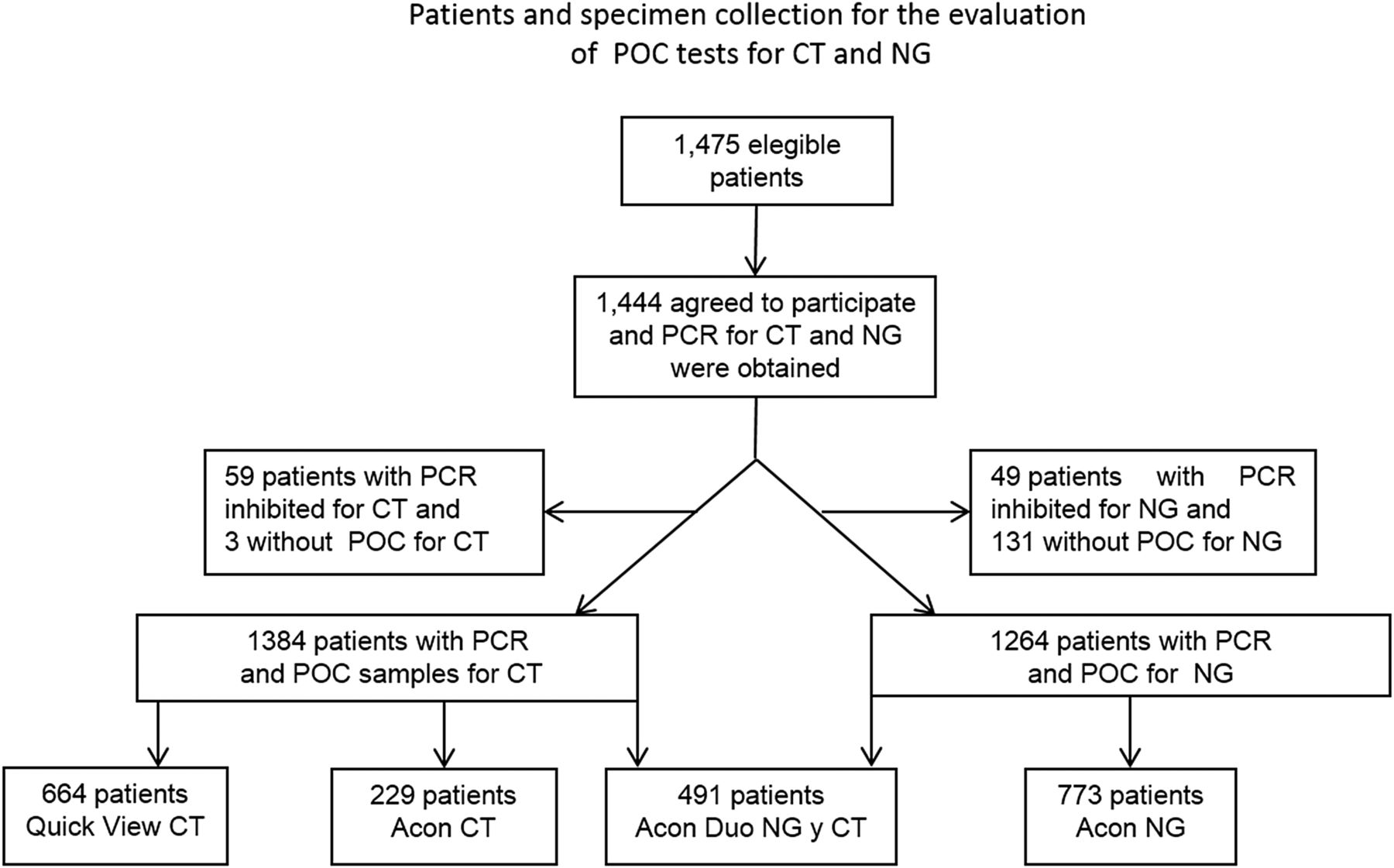
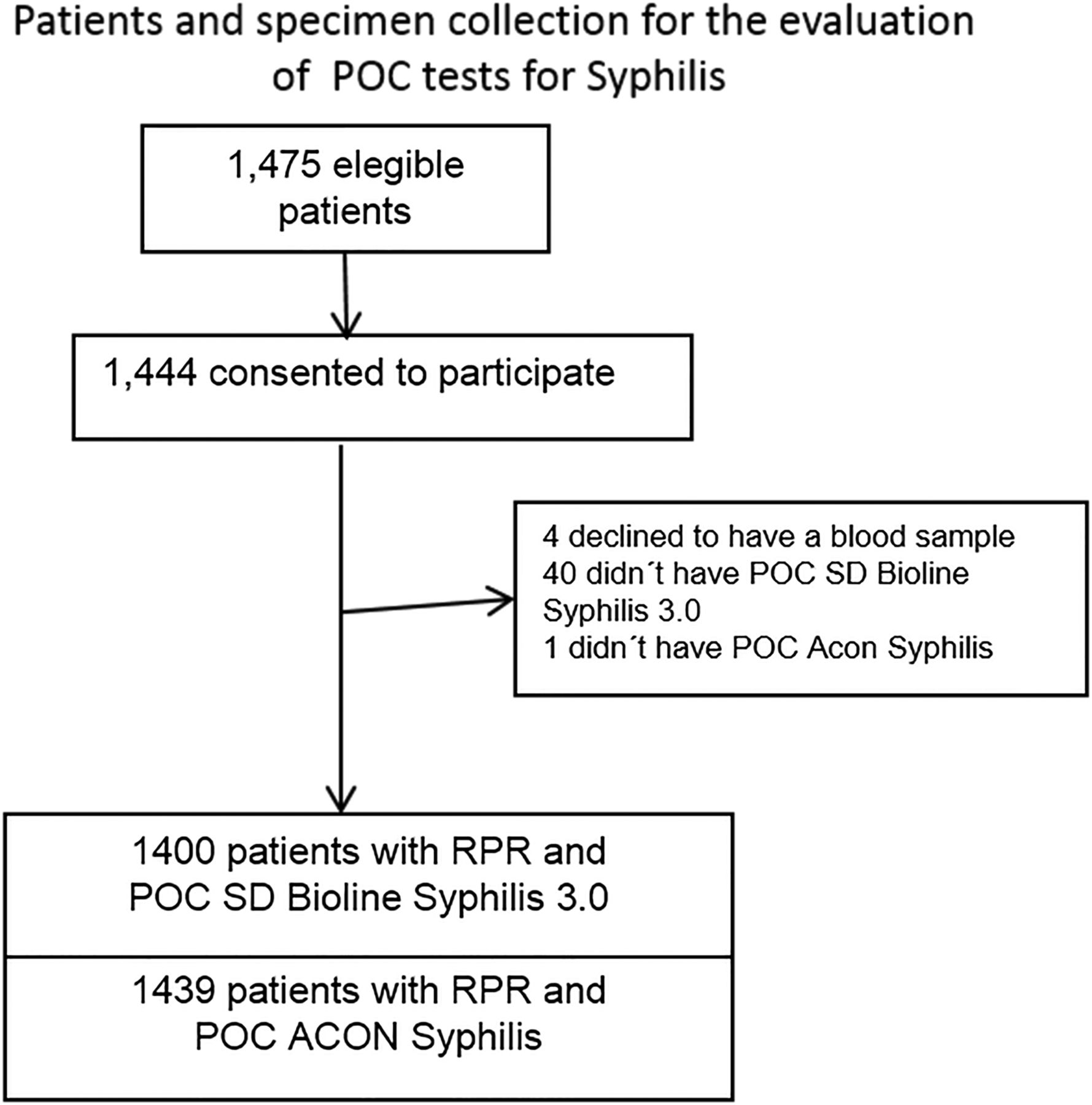
A total of 1475 patients fulfilled the inclusion criteria of which 1444 (98%) consented to participate in the study. PCR test inhibition occurred in 59 samples (3.9%), complete confirmatory tests were available in 1385 (96%). RTs for CT were done in 1384 (95.8%) women and for NG in 1264 (87.5%) women. Processing time for RT was 14 min for NG and CT, 11 min for syphilis ACON and between 6 min and 21 min for syphilis SD BIOLINE, after the serum was ready.
Flow diagrams for the number of participants and diagnostic tests performed are shown in figures 1 and 2. The prevalence by PCR for CT was 9.7% (134/1385) and for NG was 1.4% (19/1385). The prevalence of syphilis was 0.9% (12/1385). Participants’ mean age was 31.3 years (SD 8.9); mean age at the beginning of sexual activity was 16.9 years (SD 3.08). One hundred and thirteen women stated that they were sex workers (8.9%). Regarding other risk factors, 27.1% stated having occasional sexual partners in the last year, 50.6% stated that the permanent partners never used a condom and 20.4% used it occasionally. The main symptoms were vaginal discharge (89%), pruritus (58.1%), bad smell (41.9%) and/or abdominal pain (44.2%) (table 1).
Sociodemographic characteristics of symptomatic women stratified by confirmed diagnosis of sexually transmitted infection (STI) in three institutions of Bogotá, Colombia, 2010

Diagram of patients and specimen collection for the evaluation of point of care (POC) tests for C. trachomatis (CT) and Neisseria gonorrhoeae (NG) in symptomatic women; AMPLICOR Roche.

{kind=link}
{kind=link}
Diagram of patients and specimen collection for the evaluation of POC tests for syphilis in symptomatic women. RPR, rapid plasma reagin; POC, point of care.
The sensitivity for the CT RTs ranged between 22.7% (95% CI 2.9% to 42.5%) and 33.7% (95% CI 17.9% to 43.1%) and the specificity from 99.4% ((95% CI 98.6% to 100%) to 100% (95% CI 99.7% to 100%); the LRs+ were 57.6 and 131.8 and the LRs− of the three RTs were 0.6, 0.7 and 0.8 The sensitivity of ACON Duo for NG was 12.5% (95% CI 0% to 41.7%) and the specificity was 99.8% (95% CI 99.3% to 100%); the LR+ was 60.4 and the LR− was 0.9. The sensitivity of the syphilis RTs ranged from 91.6% (95% CI 71.8% to 100%) to 100% (95% CI 95.8% to 100%) and the specificity was 98.8% (95% CI 98.2% to 99.4%), the LRs+ were 74.3 and 84.0 and the LR− was 0.1 (table 2).
Diagnostic accuracy characteristics for rapid tests for Chlamydia trachomatis, Neisseria gonorrhoeae and syphilis, compared with PCR and rapid plasma reagin (RPR) and Treponema pallidum haemagglutination assay (TPHA) tests for syphilis
Discussion
Our study to evaluate some RTs to be used at the POC showed a sensitivity of 22–37% for CT, 12% for NG and greater than 91% for syphilis. The specificity of the studied tests was greater than 91%.
Our results for the diagnostic performance of the RT for CT are similar to those reported by van Dommelen et al,14 van der Helm et al15 and Yin et al;16 the sensitivity was lower than that reported by Sabidó et al (62.9%),9 Mahilum-Tapay et al17 (83.5%) and Pate et al18 (92.9%). The differences in sensitivities cannot be explained by the prevalence or population studied, but could have depended on the technology being used (see online supplementary table S3A).
The RT for CT reported by Mahilum et al17 used a novel signal amplification system that maximises the visual test signal; they showed that self-collected vaginal samples performed as well as endocervical swabs and first void urine, across a range of NAATs. Confirmatory tests, different from NAAT, such as culture or immunofluorescence tests, may underestimate the true positives.18 ,19 Our study used PCR due to the high diagnostic accuracy reported; with a mean sensitivity of 90%, PCR is 20–30% more sensitive than culture and has a specificity between 99% and 100%.20 Using a sample site different from the endocervical smear could change the results of the operational characteristics of the diagnostic tests.6
Another aspect that could affect the performance of the tests is the quality of the sample in terms of bacterial load and number of cells containing CT. The sensitivity of CT RTs has been reported to be higher in samples with a high bacterial load, although the clinical relevance of the level of organism load is debated.19
The results of our study for NG revealed a lower sensitivity than that reported by Watchirs et al10 in a systematic review of RT diagnostic performance, where mean leucocyte esterase dipstick sensitivity was 71% (23% to 85%) and mean specificity was 70% (33% to 99%). Mean immunochromatographic test sensitivity was 70% (60% to 94%) and mean specificity 96% (89% to 97%). The differences with our data might be explained by factors such as small amount of antigen, and/or low prevalence of NG in this population. Additionally, our results were not consistent with those reported in the inserts by the manufacturers: sensitivity of 71–97% and specificity of 90–99% for CT,21 ,22 and sensitivity of 82–96% and specificity of 88.9–99% for NG in endocervical samples,22 compared with culture for NG and PCR and culture for CT, as gold standards.
Our results of RT for syphilis were better than those reported by Benzaken et al23 and Mishra et al,24 however those studies used finger prick whole blood samples, and similar to those reported by Mabey et al,25 whose study used whole blood and serum in the laboratory. That study mainly included non-pregnant women or men (see online supplementary table S3B). We used frozen serum at the reference laboratory because a better diagnostic performance for the test was described by Mabey et al25 and also by Jafari et al26 in a recent meta-analysis when serum is used in comparison with total blood.
The strengths of the present study include a low risk of misclassification, because recommended CT, NG and syphilis diagnostic gold standards were used and very few tests were inhibited for PCR analysis (3.9%). Performance or detection bias risk was low, as bacteriologists carrying out the gold standard diagnostic procedures were masked to the results of the RT results and the syndromic diagnosis.
Our study has some limitations. The results may have been affected by the order in which the samples were obtained. Interobserver agreement was not evaluated. The estimated sample size was calculated to obtain 30 cases of NG as needed to evaluate the diagnostic performance of the test, but there were only 19 cases; this lower number could affect the precision of the estimation.
The tests for CT and NG used in this study did not reach the diagnostic characteristics necessary to be included in clinical practice, according the WHO criteria for RT.10 ,27 However, diagnostic performance of the new generations of RT for CT and NG should continue to be evaluated.
The diagnostic performance characteristics of the two syphilis tests evaluated in this study suggest that they could be used in the POC, considering that recent studies showed similar results when the sample is obtained using finger sticks.23 ,24
In Colombia, the national guidelines for STI recommend the syndromic approach for the management of STI,28 nevertheless, as was stated above, for syphilis and NG or CT infections, the performance of the syndromic approach could be low in terms of high false negative results. This study shows that RTs at POC for CT and syphilis could improve the diagnosis and timely treatment in STI high-risk patients. An economic evaluation of the use of RTs for CT could give more information for a better informed decision.
Conclusions
The RTs evaluated for CT and NG have low sensitivity and adequate specificity in symptomatic women. Syphilis tests show excellent diagnostic performance when used in venipuncture samples. The RTs studied are not useful for NG screening at the POC. In case of CT a recommendation about their use in routine care should be supported by a cost-effectiveness analysis. The RTs should be used for syphilis screening in populations at high risk for STIs or in pregnant women. In Colombia, where gold standard tests for STIs are expensive and are available only in high level centres, it is advisable to continue evaluating RTs. An economic evaluation of the use of RTs for CT could also give more information for a better informed decision in our country.
Key messages
There is growing interest in using rapid tests for the diagnosis of sexually transmitted infections in order to increase opportunity of treatment.
The rapid tests for syphilis screening using frozen serum showed high sensitivity and specificity.
The recommendation for the use of rapid test for C. trachomatis rapid test should be supported by a cost effectiveness analysis.
Acknowledgments
The authors thank Standard Diagnostics, South Korea, for donating the rapid tests for syphilis, SD Bioline Result 3.0, PROFAMILIA, and the ‘Hospital Engativá’ and ’Hospital de Fontibón’ for participating as sites in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online tables
Abstract in Spanish
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Abstract in Spanish - Online abstract
Footnotes
Handling editor Jackie A Cassell
Contributors LN-F and LM-A designed the protocol, carried out the laboratory tests, analysed and prepared the final elaboration document.
Funding This work was supported by Colciencias Grant 621/2009, Universidad Nacional de Colombia Bogotá Research Division; the Bogotá District Secretariat of Health and the Global Network for Perinatal & Reproductive Health, FUNDARED-MATERNA, Bogotá, Colombia.
Competing interests The corresponding author, HG-D, is an editorial board member of the Sexually Transmitted Diseases Journal. Preliminary results of this study were presented at: The XXVIII National Congress of Gynecology and Obstetrics, Cartagena, Colombia, May 2012 and the XX World Congress of Gynecology and Obstetrics, FIGO, Rome, Italy, October 2012.
Patient consent Obtained.
Ethics approval The Hospitals and the Universidad Nacional de Colombia's Faculty of Medicine's ethics committees.
Provenance and peer review Not commissioned; externally peer reviewed.