Article Text

Abstract
Objectives We evaluated the relationship of sexually transmitted infections (STIs) and genital infections during pregnancy and subsequent risk for infant mortality and stillbirth.
Methods This was a nested longitudinal analysis using data from a study of peripartum HIV acquisition in Kenya. In the parent study, HIV-uninfected women were enrolled during pregnancy and followed until 9 months postpartum. For this analysis, women who tested positive for HIV at any point, had a non-singleton pregnancy or a spontaneous abortion <20 weeks were excluded. At enrolment, laboratory methods were used to screen for bacterial vaginosis (BV), vaginal yeast, Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG) and Trichomonas vaginalis (TV). Syphilis was diagnosed using rapid plasma reagin testing and genital ulcer disease (GUD) identified by clinical examination. Treatment of laboratory-confirmed STIs and syndromic management was provided per Kenyan national guidelines. Predictors of stillbirth and infant mortality were determined using logistic regression and Cox proportional hazards models.
Results Overall, among 1221 women, 55% had STIs or genital infections detected: vaginal yeast (25%), BV (22%), TV (6%), CT (5%), NG (2%) and syphilis (1%). Among women with STIs/genital infections (n=592), 34% had symptoms. Overall, 19/1221 (2%) women experienced stillbirths. Among 1202 live births, 34 infant deaths occurred (incidence 4.0 deaths per 100 person-years, 95% CI 2.8 to 5.5). After adjustment for maternal age, education and study site, stillbirth was associated with maternal GUD (adjusted OR=9.19, 95% CI1.91 to 44.35, p=0.006). Maternal NG was associated with infant mortality (adjusted HR=3.83, 95% CI1.16 to 12.68, p=0.028); there was some evidence that maternal CT was associated with infant mortality. Stillbirth or infant mortality were not associated with other genital infections.
Conclusions STIs and genital infections were common, frequently asymptomatic and some associated with stillbirth or infant mortality. Expediting diagnosis and treatment of STIs in pregnancy may improve infant outcomes.
- sexually transmitted diseases
- Africa
- neisseria gonorrhoeae
- pregnancy
- stillbirth
- infant mortality
Statistics from Altmetric.com
Introduction
Sexually transmitted infections (STIs) contribute substantially to the global burden of reproductive disease and maternal-child health consequences. Non-HIV STIs have been implicated in adverse pregnancy outcomes including spontaneous abortion, stillbirth, preterm birth and low birth weight.1 Over 90% of the global burden of STIs occurs in low-income and middle-income countries,2 though data are few on the impact of STIs in pregnancy on perinatal and infant outcomes in these settings.3 A global action plan for the elimination of mother-to-child transmission of syphilis was launched in 2007 with the aim of 95% coverage of syphilis testing and treatment among pregnant women.4 Since then, several countries have adopted universal antenatal syphilis screening programmes using rapid on-site syphilis testing to accelerate maternal treatment and prevention of newborn complications of syphilis.4 5 However, similar efforts to scale up treatment and prevention of other STIs during pregnancy have not been implemented and STIs among pregnant women persist as a global maternal-child health challenge.6 7
Several individual studies and one systematic review estimate prevalence rates for individual STIs from 2.7% to 50.8% among pregnant women in sub-Saharan Africa.8 To date, most studies evaluating maternal STIs and perinatal outcomes in African settings have been retrospective in design, with STI data collected at or after delivery. Few longitudinal studies have evaluated the association of STIs during pregnancy on perinatal and infant outcomes among African cohorts.6 9–12 The combined high prevalence of STIs during pregnancy8 and high risk of stillbirth and infant mortality in sub-Saharan Africa warrants additional investigation.
We evaluated the relationship of several STIs and genital infections (Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), Trichomonas vaginalis (TV), bacterial vaginosis (BV), vaginal yeast, syphilis and genital ulcer disease (GUD)) diagnosed during pregnancy and stillbirth and infant mortality among a cohort of HIV-uninfected women in Western Kenya.
Methods
Study population, design and procedures
Data from a prospective cohort study (Mama Salama Study) of HIV-uninfected pregnant and postpartum women in the Nyanza region of Kenya were used for this analysis.13 Study procedures have previously been described.13 Briefly, HIV-uninfected pregnant women were enrolled during pregnancy and followed during pregnancy (visits at 20, 24, 28, 32, 36 weeks gestation) and through the postpartum period (visits at 2, 6, 10, 14 weeks; 6 and 9 months). Gestational age was determined by study nurses by ascertainment of last menstrual period (LMP) and fundal height. If there was disagreement of >3 weeks between LMP and fundal height estimates, ultrasound was performed. Study clinicians diagnosed and treated women with malaria. All women with malaria were treated per Kenya Ministry of Health's national treatment guidelines.14
Women self-collected vaginal swabs and had physical examinations at each study visit apart from 2 weeks postdelivery. Pelvic examinations were performed at enrolment, 28 weeks gestation, 6 weeks postpartum and 6 months postpartum. Women were assessed for signs and symptoms of genital infections (abnormal vaginal discharge and/or vaginal itching or burning) at every visit and managed with syndromic treatment. In addition, women diagnosed with a laboratory-confirmed STI or genital infection, and who had not received syndromic treatment, were treated per Kenya Ministry of Health's treatment guidelines for genital infections in pregnancy.15 Antimicrobials were administered at no cost as part of the study following receipt of results. Women were counselled to have their partner come to the study clinic for complete STI testing and treatment and a subset of women delivered treatment to their partners.16 Infant outcomes were assessed at all postpartum visits.
Laboratory methods
CT and NG were assessed at the Mombasa HIV/STD Research Laboratory using clinician collected endocervical samples for nucleic acid amplification tests (NAAT) with the APTIMA Combo 2 Assay (HOLOGIC/GEN-PROBE, San Diego, California, USA). Syphilis serology was based on rapid plasma reagin (RPR) tests conducted as part of routine antenatal care (ANC) and abstracted from maternal child health booklets or conducted by study staff if test results were unavailable. TV, vaginal yeast and BV were assessed at every study visit. BV was defined using Nugent score. TV was detected by wet mount microscopy and vaginal yeast by direct microscopy after addition of 10% KOH. TV and vaginal yeast results were available on the same day as sample collection and other results were returned to women at their next study visit.
Definition of outcomes
Women completed a questionnaire at the first postpartum study visit about their delivery and pregnancy outcomes were abstracted from medical records when available. In the event of an infant death, medical records were abstracted. If cause of death information was incomplete, a verbal autopsy was performed by study nurses with the mother or caregiver when possible. Stillbirth was defined as fetal death at ≥20 weeks gestation and included births without signs of life. Infant mortality was defined as a death prior to study exit at 9 months of age following a documented live birth; neonatal deaths occurred day 0–27 and postneonatal deaths occurred >27 days since a live birth up until 9 months of age.
Statistical methods
The size of the current study population was determined by the size of the parent study. Women who tested positive for HIV at any point during the study or had a spontaneous abortion <20 weeks were excluded from this analysis. Only women with singleton pregnancy and pregnancy outcome information available were included in the analysis. Logistic regression was conducted to evaluate potential cofactors of stillbirth (compared with live births). Cox proportional hazards models were used to determine correlates of time-to-infant mortality among pregnancies that had a documented live birth. All models used robust SEs.
We evaluated potential correlates of stillbirth and infant mortality including having an STI or genital infection (CT, NG, TV, BV, vaginal yeast, syphilis or GUD) at enrolment, being unmarried, having crowded living conditions (≥3 people per room), having a travel time >1 hour to clinic, being primigravida, having a short birth interval (delivering <2 years since last pregnancy ended among women who were previously pregnant), delivering preterm (<37 weeks) and malaria diagnosis during pregnancy. Variables associated with stillbirth or infant mortality (alpha=0.10) in univariate analyses were included in the respective multivariate models. All multivariate models were adjusted a priori for maternal age and education due to the known association of these factors with perinatal and infant outcomes.17–19 Clinic site was also adjusted for a priori to account for potential geographical differences in underlying STI prevalence, stillbirth or infant mortality. P≤0.05 were considered statistically significant. Statistical analysis was performed using Stata (V.13, College Station, Texas, USA).
Results
Among 1304 pregnant women enrolled in the parent study, 1221 (94%) met inclusion criteria for this analysis (figure 1). Median maternal age was 22 years (IQR 19–27), median gestational age at enrolment was 27 weeks (IQR 22–31), most women were married (79%) and had a median of 8 years of education (IQR 7–10); 31% were primigravida (table 1).
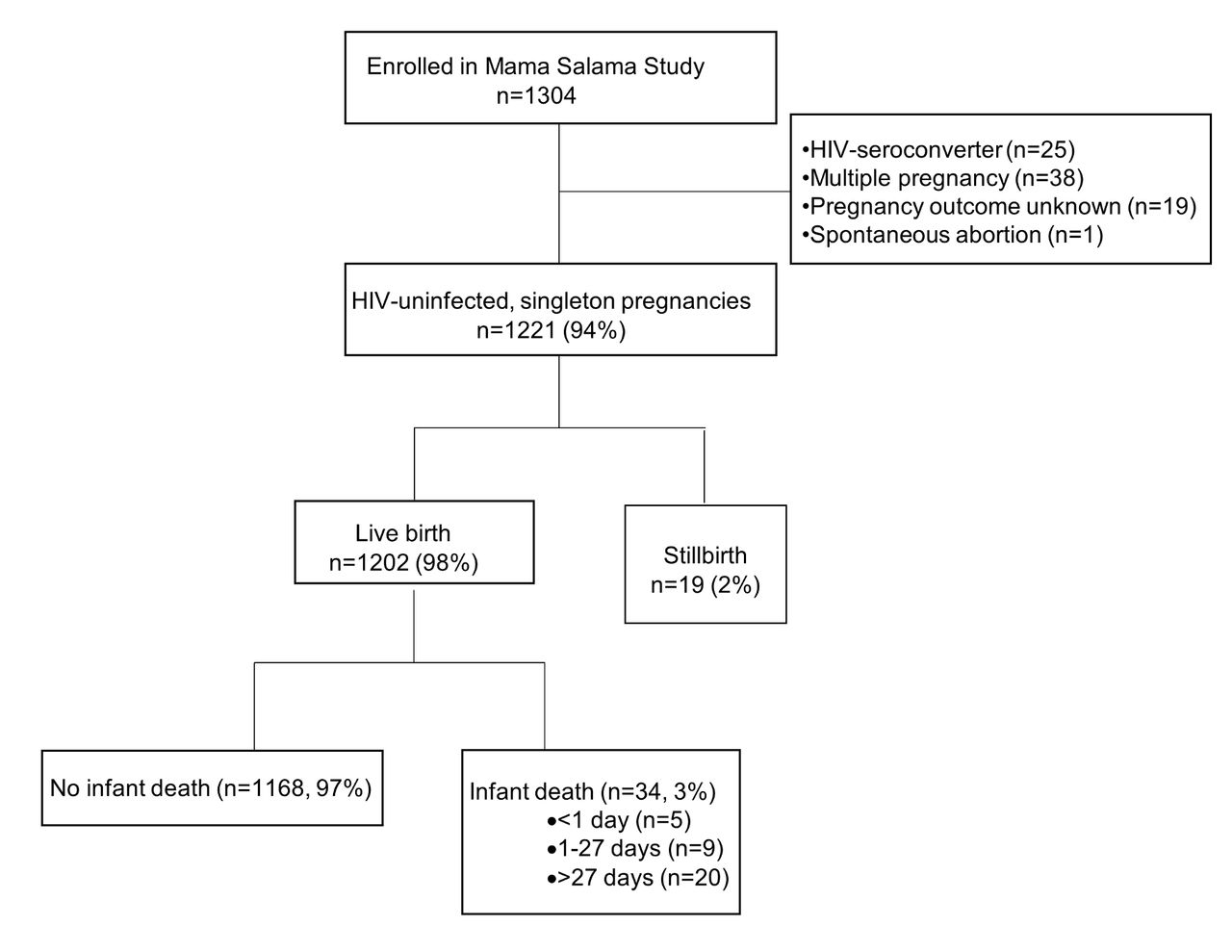
{kind=link}
Flow diagram of inclusion.
Characteristics of HIV-uninfected mothers*
Overall, 55% of women had ≥1 STI or genital infection. Vaginal yeast was the most frequent (25%) infection, followed by BV (22%). Less than 10% of women had CT, NG, TV, syphilis or GUD, respectively (table 1). Among women with STIs and/or genital infections (n=592), 34% had any symptoms and frequency of symptoms varied by infection: vaginal yeast (39%), BV (29%), CT (43%), NG (25%), TV (53%) and syphilis (20%). Of the 10 women who had GUD at enrolment, none had syphilis and no other aetiological testing was performed. Laboratory results for NG and CT diagnosis had a median turnaround time of 22 days (IQR 15–28); all other results were available the same day.
Stillbirth and neonatal mortality
In total, 19 (2%) women experienced stillbirth (rate 15.6 per 1000 live births). The median gestational age for stillbirths was 39 weeks (IQR 35–41 weeks). Compared with women who had live births, women who had stillbirths were more likely to be primigravida (76% vs 26%, p=0.022) and have GUD (11% vs 1%, p=0.004). After adjustment for maternal age, education and study site, stillbirth was associated with being primigravida (adjusted OR (aOR)=3.39, 95% CI 1.21 to 13.32, p=0.021) and having GUD at enrolment (aOR=9.19, 95% CI 1.91 to 44.35, p=0.006); there was some evidence for an association with having preterm birth (aOR=2.41, 95% CI 0.84 to 6.92, p=0.103) (table 2).
Correlates of stillbirth among HIV-uninfected mothers
Neonatal mortality occurred among 14/1202 (1%) infants following live birth. Women who had crowded living situations and short birth intervals were more likely to have an infant die ≤27 days in univariate models (OR=3.40, 95% CI 1.16 to 9.88, p=0.025 and OR=3.46, 95% CI 0.92 to 13.04, p=0.067, respectively). We did not detect an association between neonatal mortality and STIs or any other characteristic.
Infant mortality
During 859.7 person-years of follow-up after live birth, 34 infant deaths occurred (figure 1), resulting in an overall incidence of 4.0 infant deaths per 100 person-years; 5 deaths occurred at <1 day, 9 occurred on days 1–27 and 20 occurred >27 days. Approximately one-fourth (24%) of infants were hospitalised at the time of death, and cause of death was captured for 44% of infant deaths. Among the deaths with known causes (n=15), birth complications were the most frequent cause (n=5, 30%) followed by pneumonia (n=4, 27%); confirmed malaria (n=2, 13%), suspected malaria (n=2, 13%) and gastrointestinal disease (n=2, 13%). Infants were not examined specifically for ophthalmia neonatorum.
Maternal CT (HR=2.38, 95% CI 0.86 to 6.57, p=0.093) and NG (HR=4.14, 95% CI 1.28 to 13.35, p=0.017) were both associated with higher incidence of infant mortality (table 3). Incidence of infant mortality was higher among women who delivered preterm compared with women who delivered ≥37 weeks (7.5 vs 2.7 per 100 person-years, HR=2.86, 95% CI 1.37 to 5.96, p=0.004). All cases of infant mortality among women with NG also had preterm birth (3/3) and 3/4 cases of infant mortality among women with CT had preterm birth. Women who had either NG or CT (n=85) had some evidence for increased risk of infant mortality (HR=2.71, 95% CI 0.84 to 5.62, p=0.102). Women coinfected with NG and CT had a 26-fold increased risk of infant mortality compared with women with neither infection (HR=25.84, 95% CI 6.85 to 97.58, p<0.001). We did not detect statistically significant associations between other genital infections and infant mortality; however, syphilis trended towards an association with higher infant mortality. Additionally, there was evidence for an association between infant mortality and travel time to clinic ≥1 hour (HR=2.24, 95% CI 0.94 to 5.33, p=0.069). Malaria during pregnancy was associated with increased infant mortality (HR=2.70, 95% CI 1.12 to 6.50, p=0.027). Among women with malaria diagnosed during pregnancy, 89% had documented treatment; incidence of infant mortality did not differ between those who received treatment compared with those without treatment (7% vs 11%, respectively; p=0.634). Among multigravidas, women with a short birth interval had a 3-fold higher incidence of infant mortality compared with women who delivered ≥2 years since their last pregnancy (HR=3.19, 95% CI 1.29 to 7.90, p=0.012).
Correlates of all infant mortality among HIV-uninfected mothers
After adjustment for maternal age, maternal education, study site and preterm birth, multivariate results were similar to univariate models (table 3). Results were similar when excluding infant death occurring <1 day (data not shown). In restricted analysis with postneonatal mortality as the outcome, correlates remained the same as the overall infant mortality analysis (data not shown) with the exception that CT at enrolment was not associated with postneonatal mortality and there was a trend towards an association with syphilis (HR=6.45, 95% CI 0.85 to 49.16, p=0.072).
Discussion
In this large prospective study among HIV-uninfected pregnant women in Western Kenya, STIs and genital infections were common and often asymptomatic. Stillbirth was associated with being primigravida and with GUD during pregnancy. Infant mortality was associated with maternal NG, CT and malaria during pregnancy; preterm delivery and short birth intervals. Maternal NG, preterm delivery and short birth intervals remained significantly associated with infant mortality in multivariate models. Current global STI control is hampered by a large proportion of asymptomatic infections, lack of feasible diagnostic tests, antimicrobial resistance and barriers to intervention access, availability and scale-up.20 21 Our findings suggest that the burden of STIs and genital infections is high among pregnant women and that STI treatment and prevention programmes should be implemented in maternal child health (MCH) settings to decrease infant morbidity and mortality. We found associations between NG and infant mortality despite providing syndromic treatment and medication for diagnosed STIs, suggesting need for more prompt STI diagnosis and treatment.
Maternal NG was associated with increased infant mortality in our study and all infant deaths with NG exposure were preterm infants. To our knowledge, this is the first study to evaluate the relationship of maternal NG infection during pregnancy and infant mortality among HIV-uninfected African women. Previous studies have shown associations between maternal NG and premature rupture of membranes, low birth weight, preterm birth and postpartum endometritis.22–24 Neonatal gonococcal infection can result in systemic infections including septic arthritis, septicemia and meningitis, in addition to blindness.25 A recent study among HIV-exposed infants from Brazil, South Africa, Argentina and the USA did not detect an association between maternal NG infection during pregnancy and infant mortality; however, overall infant mortality rates were low.3 In our study, 36% of all mothers with NG had preterm birth and all cases of infant mortality following maternal NG were preterm. NG is a curable STI, although there are recent concerns regarding drug resistance.26
Currently diagnosis and treatment of maternal STIs relies on syndromic management in most MCH clinics in Africa.27–30 Our study included syndromic management for STIs; however, women with NG in pregnancy are often asymptomatic. In our study population, 75% of women with NG had no symptoms. Syndromic management can be effective for urethral discharge in men and for GUD.27–29 However, more robust approaches are needed to control cervical infections in women, especially CT and NG, because vaginal discharge is a poor proxy for endocervical infection.27–29 For CT, NG and TV, affordable point-of-care tests are needed.web reference (w) 1 Future studies on cost-effective approaches for STI screening and treatment for pregnant women, including rapid point of care testing, will be critical to address the burden of adverse infant outcomes attributed to STIs.
We found a higher rate of stillbirth (15.6 per 1000 live births) than previous studies in similar regions in Kenya (10 to 12 per 1000 live births).w2-w3 Stillbirths were associated with GUD and being primigravida in our study. No aetiological testing was conducted for GUD. However, none of the mothers with GUD were RPR-positive, suggesting that these cases may be due to herpes simplex virus (HSV-2) infections.w4 HSV-2 seropositivity alone has not been associated with adverse pregnancy outcomes, but primary HSV infection may manifest as GUD and is more likely to result in poor infant outcomes.w5-w6 There is limited evidence linking HSV-2 to stillbirths and further studies to better define associations between acute HSV-2 and stillbirth are needed. Associations between primigravida and stillbirths have been previously reported although underlying mechanisms are unclear.w7 No cases of stillbirth occurred among women with syphilis in our study, though cases of syphilis were few overall.
Among live births in our study, preterm birth was associated with a 2-fold increased risk of infant mortality, consistent with other studies.w8 Preterm birth and maternal STIs were linked; however, many infants with preterm birth were born to mothers without STIs. Systematic screening for bacterial STIs (NG, CT, syphilis) and malaria will be important both to decrease preterm birth and infant mortality. At the same time, research into other determinants of preterm labour and improved management of prematurity will be critical to decrease infant mortality. Research into new interventions for preventing preterm labour remains an urgent priority in combating child mortality. Identification of preterm infants and vigilant follow-up to prevent morbidity and mortality will be important for these infants.
Our study has strengths and limitations. Most women enrolled in our study during the later trimesters and we may have missed STIs or genital infections that occurred early in pregnancy. The cohort was large and prospective and included detailed characterisation of maternal STIs and infant outcomes. However, the parent study did not incorporate systematic verbal autopsy to determine cause of infant death. Gestational age measurements are problematic due to inaccurate recall of LMP, though fundal height and, in a smaller subset, ultrasound data, were included to estimate gestational age. While nearly all STIs were laboratory-confirmed, genital ulcer aetiology testing was not conducted and future studies that include aetiological testing for genital ulcers and HSV-2 testing are needed. Our sample size was determined by the parent study. The statistical power to detect associations was modest for some outcomes and exposures which were infrequent. Thus, findings from multivariate regression models should be interpreted with caution. We evaluated all infections independently which may cause erroneous inferences due to multiple testing and further studies will be useful to validate our results.
In conclusion, our study contributes to growing evidence that STIs and genital infections persist as a maternal-child health issue in resource-limited settings. Prioritising maternal STI diagnosis, treatment and prevention within ANC and improved management of preterm infants could substantially reduce the burden of stillbirth and infant mortality.
Key messages
Over half of HIV-uninfected Kenyan pregnant women had ≥1 genital infections and approximately two-thirds were asymptomatic.
Maternal Neisseria gonorrhoeae infection in pregnancy increased risk of infant mortality and all cases of infant death with N. gonorrhoeae exposure were born preterm.
Genital ulcer disease in pregnancy may increase risk of stillbirth and warrants further investigation.
References
Footnotes
AJW and JP contributed equally.
Handling editor Jackie A Cassell
Correction notice This paper has been corrected since it was published Online First. In the original version some of the references were not styled properly.
Contributors AJW, JP and GJ-S conceived the question and designed the study. GJ-S obtained funding for the study. ALD, JK, JAU, DM, RSM and GJ-S participated in data collection. AJW, JP and GJ-S conducted the data analyses. All authors participated in preparation of the manuscript and approved the final draft for submission.
Funding Medical Student Research Training Program, University of Washington School of Medicine. This study was funded through National Institutes of Health grant (P01 HSD 064915; T32 T32AI07140 to JP; K01 AI116298 to ALD; K24 HD054314 to GJ-S) and received assistance from the University of Washington Center for AIDS Research (P30 AI27757). The Mama Salama Study Team was supported by the University of Washington’s Global Center for Integrated Health of Women Adolescents and Children (Global WACh).
Competing interests None declared.
Patient consent Obtained.
Ethics approval All study procedures were approved by the Kenyatta National Hospital/University of Nairobi Ethical Research Committee (#P11/4/2010) and the University of Washington Institutional Review Board (#38472A) prior to study initiation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Detailed information on study data is available from GJ-S on request at gjohn@uw.edu.