Article Text

Abstract
Objective: To present, describe, and assess trends in gonorrhoea in western Europe between 1991 and 1996.
Methods: A European Union concerted action was initiated in 1990 to monitor the prevalence of HIV among patients with a sexually transmitted infection in sentinel networks in western Europe. Data from this concerted action were used to assess trends in gonorrhoea between 1991 and 1996. Where possible, the trends were validated by comparing them with national laboratory reports or data from more extensive sexually transmitted infection surveillance networks.
Results: 7192 episodes of gonorrhoea were recorded at 38 sentinel sites in nine countries between 1991 and 1996. In most networks, there was a decline in the number of cases of gonorrhoea among heterosexual men and women. The decline was most marked in the Scandinavian countries. Decreases were also observed among men having sex with men, but in some networks—England and Wales, Netherlands, and Scotland—an increase was observed in more recent years. This increase was mainly the result of an increase in cases among the older age group (25 years and above). The trends observed in six of the sentinel networks were confirmed by trends in national laboratory reports or data from more extensive sexual transmitted infection surveillance systems.
Conclusions: These data indicate that, overall, there was a decline in the number of gonorrhoeal cases in western Europe between 1991 and 1996. The results, however, also indicate that in more recent years there was an increase in the number of gonorrhoea cases among men having sex with men in some countries. Further investigations are necessary to determine if this observation is due to an increase in risky sexual behaviours in this population group.
- gonorrhoea
- western Europe
Statistics from Altmetric.com
Introduction
Sexually transmitted infections are a well recognised public health problem.1 The importance of these diseases is not only limited to their high incidence and the acute effects of infection but also to the complications they may cause and their now well established capacity to facilitate the transmission of HIV.2, 3 Trends in the incidence of sexually transmitted infections may reflect temporal changes in sexual activity within the population. For this reason, monitoring the incidence of sexually transmitted infections has been proposed as a means of evaluating the effectiveness of AIDS prevention programmes.4 Gonorrhoea is particularly well suited to the purpose of monitoring trends in risky sexual behaviours because the risk of infection from a single exposure is high, treatment eliminates the infection, and long term immunity is not acquired.5
Even though many European countries have established sexually transmitted infection surveillance systems,6 the comparison of surveillance data—for example, data on gonorrhoea across European borders has been conspicuous by its absence. No formal European body collects data on sexually transmitted infections at a European level, as is the case with HIV/AIDS or tuberculosis. Between 1990 and 1996, a concerted action of the European communities monitored the prevalence of HIV in STI patients attending clinics in 17 sentinel networks across 15 European countries.7 The main results have been presented and discussed previously.8, 9 This paper presents and assesses the concerted action data on trends in gonorrhoea between 1991 and 1996 in nine western European countries.
Methods
The concerted action collected standardised information on patients attending sentinel network clinics with one or more episodes of a sexually transmitted infection between June 1990 and December 1996. A detailed description of the methodology and study design has been published previously.7 The list of selected sexually transmitted infections is presented in table 1.
List of 12 sexually transmitted infections with minimum methods of diagnosis for selection of patients
This list of diseases was adopted by consensus between the participating networks as representing infections that were likely to have been acquired through recent sexual contact, and that could be diagnosed through standardised widely available methods. A standard questionnaire was completed for each selected episode. The following items were recorded: age, sex, country of birth and residence, education, diagnosis of the sexually transmitted infection(s), method(s) of diagnosis, current sexual orientation (in previous 6 months, as stated by the patient), number of sexual partners during the previous 6 months, injecting drug use since 1978, previous and present HIV antibody testing. Each national coordinator was responsible for establishing and running his or her network. The networks consisted of clinics for sexually transmitted infections, dermatovenereology clinics, or gynaecology clinics. One network (Belgium) consisted mainly of sentinel general practitioners. A list of the networks and the number of sexually transmitted infection episodes per network is presented in table 2.
Number of sexually transmitted infection episodes and episodes of gonorrhoea in the European union concerted action programme and number of sites and gonorrhoea episodes included in the trend analysis
This paper presents trends in diagnoses of gonorrhoea. The case definition used in the study protocol included infections identified by culture or, where appropriate, microscopy, in the cervix, urethra, rectum, or throat. Information on the anatomical site of the gonorrhoeal infection was not available in all networks and was therefore not included in the analyses.
Analyses were restricted to networks that reported at least 120 gonorrhoea cases during the whole study period and to sites that submitted data on a consistent basis and did not experience changes in their catchment population as a result of events such as the opening or closing of a nearby health facility. The latter was assessed through an evaluation study that was carried out between December 1996 and April 1997.9 The evaluation was based on a questionnaire that was sent to each network coordinator and the lead collaborator at each of the reporting clinics.
The sentinel populations were chosen as they represented a group at elevated risk of HIV infection through recent sexual contact, rather than being representative of the total population of all patients with a sexually transmitted infection in a country.
Because of the heterogeneity of the type, size, and catchment populations of the networks, it was decided that the data should not be aggregated but that differences and similarities across the networks would be explored. When possible, the observed trends were validated by comparing the data with laboratory reports or with more extensive clinical reporting or notification data on sexually transmitted infection in the same country. Parameter values used in the analyses were expressed relative to the relevant 1991 value.
Trends for all networks were presented for men having sex with men, heterosexual men, and all women. Men having sex with men were defined as “men who were homosexually active during the past 6 months, as stated by themselves.” If sufficient data were available, trends were also assessed for under 25s and over 25s, separately. Finally, some patient characteristics and the change of these characteristics over time were studied. This was performed by sex, sexual orientation among men, age, and being born or having normal residence in another country.
STATISTICAL METHODS
Within network trends were tested for significance by linear regression analysis. Statistically significant changes in the proportions of patient characteristics between 1991 and 1996 are reported by presenting the overall change, with 95% confidence intervals.
Results
NETWORKS
Ten networks were eligible for inclusion in the analyses (see table 2). The numbers of cases in the Swedish and Finnish networks were considerably smaller than in the other eligible networks. As the characteristics of the sites and the patients were similar in both networks, it was decided that data from these two networks should be aggregated together, resulting in a total of nine networks in the analyses.
Two clinics in Denmark and one clinic in Scotland reported changes in the opening times of their clinic during the study period, but the effects of these changes were considered as marginal and not likely to affect the overall trends.
Table 2 shows that the proportion of sexually transmitted infections accounted for by gonorrhoea varies considerably among the networks: from 2% (150/8325) in Sweden to 18% (1518/8277) in the Czech Republic. These differences may be partly explained by geographical differences in the incidence of gonorrhoea but are also due to differences in the composition of the catchment population. Table 3 specifies some differences among the networks in terms of type of included health facilities and their location.
Site characteristics of the networks selected in the analysis
A total of 7192 episodes of gonorrhoea from 38 sites, most of them sexually transmitted infection clinics, were included in the final analysis.
CHARACTERISTICS OF GONORRHOEA CASES
Some of the characteristics of the patients per network are described in table 4. Among the gonorrhoeal cases the proportion of men varied from 60.3% in Portugal to 95.1% in Italy. This variation is a reflection of the populations which are attracted to one or more of the clinics in some of the networks—for example, men having sex with men. The proportion of cases among patients aged less than 25 ranged from 16.3% in Switzerland to 44.3% in Scotland. An HIV seroprevalence of 10% or more was found in four networks, especially networks with a high proportion of men having sex with men. In the seven networks for which this information was available, the proportion of cases among patients with five or more sexual partners during the previous 6 months ranged from 23.2% in Sweden and Finland to 66.1% in Greece.
Characteristics of the gonorrhoea cases in the networks selected in the analysis
A significant increase in the proportion of cases that were male was observed between 1991 and 1996 in Denmark (+12.9%; 95% CI 0.6–25.2%), England and Wales (+ 7.8%; 95% CI 3.0–12.8%), Italy (+ 8.3%; 95% CI 1.9–14.7%), and Scotland (+ 9.1%; 95% CI 0.4–17.9%). In most networks this was due to an increasing proportion of men having sex with men. A significant increase in the proportion of men who reported having sex with men was indeed observed in Denmark (+23.2%; 95% CI 5.4–41.3%), England and Wales (+10.7%; 95% CI 4.1–17.4%), Netherlands (+22.7%; 95% CI 9.7–35.6%), Scotland (+17.8%; 95% CI 5.5–30.1%), and Sweden-Finland (+24.3%; 95% CI 1.7–46.9%). The proportion of cases among patients aged less than 25, the proportion of patients born or whose normal residence was in another country, the HIV seroprevalence among all cases and the proportion of cases among patients reporting five or more sex partners during the previous 6 months remained stable in most of the networks during the whole study period.
TRENDS IN THE NETWORKS
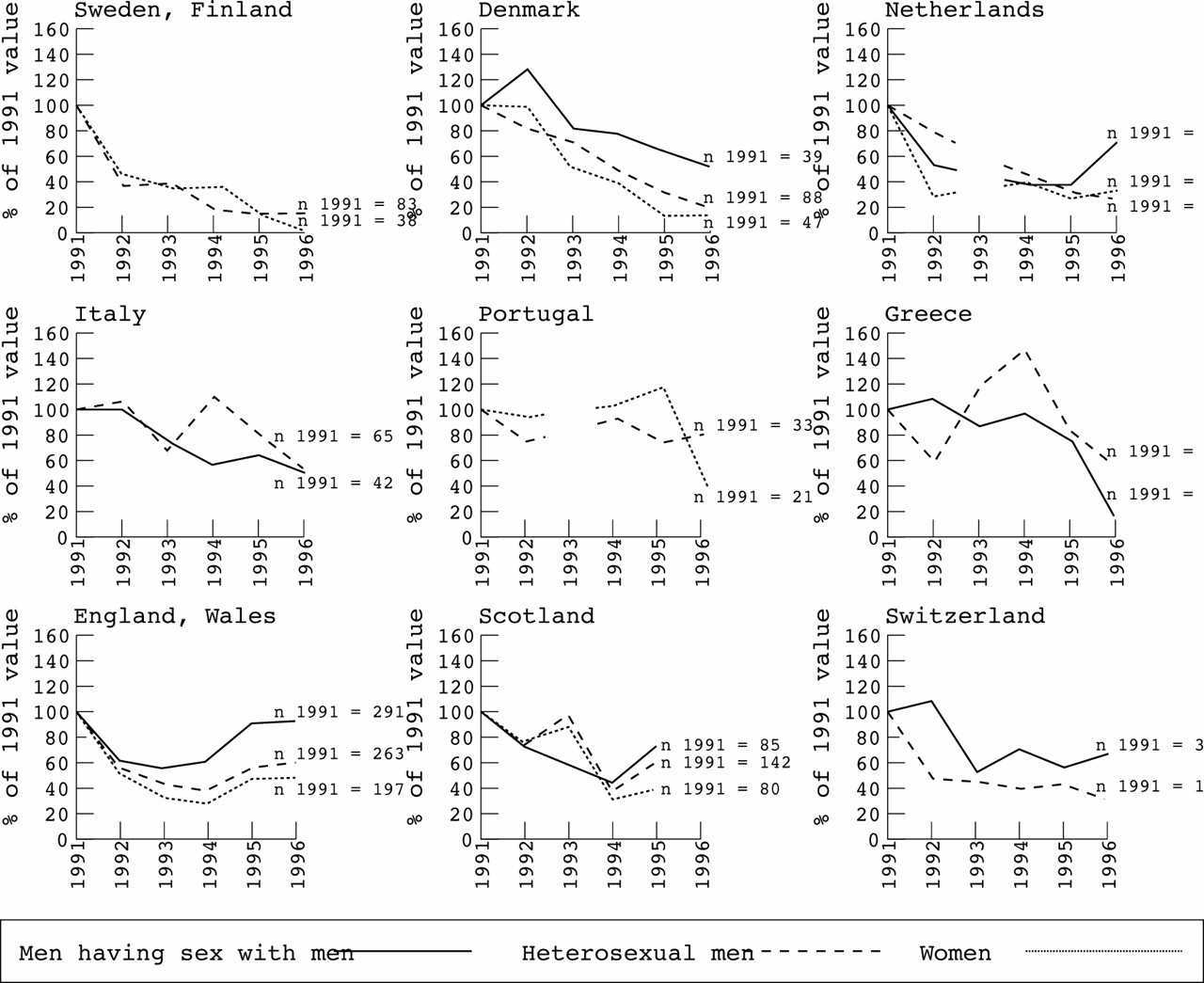
Figure 1 presents gonorrhoea trends by network among men having sex with men, heterosexual men, and women between 1991 and 1996. In most networks, there was a sharp decline in cases in the early 1990s followed by a levelling off, or even an upturn, in cases towards the end of the study period. A continued decline in cases beyond 1994 was only seen in Denmark, Greece, Italy, Portugal, and Sweden and Finland. The declining trend was most marked among heterosexual men and all women. The decrease in the number of cases among heterosexual men between 1991 and 1996 ranged from 87% in the Swedish and Finnish network to 18% in the Portuguese network. The decline was only significant in the two Scandinavian networks (p <0.001 for the Danish network and p = 0.038 for Sweden and Finland). The decrease in the number of cases among women varied from 100% in the Swedish and Finnish network (38 cases in 1991 compared with none in 1996) to 51% in the English and Welsh network. Once again, the decline was only significant in the two Scandinavian networks (p = 0.003 for Denmark and p = 0.012 for Sweden and Finland).

Gonorrhoea cases among men having sex with men, heterosexual men, and women in nine European networks, reported by sexually transmitted infection services during the period 1991–6, relative to the values in 1991. No results are presented for women in the Italian, Greek, and Swiss network and men having sex with men in the Swedish and Finnish and the Portuguese network because the total number of observations over the 6 years for those strata was too small (30 or less).
Two patterns in gonorrhoea trends among men having sex with men could be distinguished. In Denmark, Italy, and Greece a continued decline in cases was observed beyond 1994. These trends were significant in the Danish and Italian networks (p = 0.027 and p = 0.006, respectively). In England and Wales, Netherlands, Scotland, and Switzerland, the number of cases of gonorrhoea among men having sex with men remained stationary or even increased after 1994. This was most marked in Netherlands and England and Wales, where the number of cases in 1996 increased by 90% and 52%, respectively, compared with 1994. Stratification by age group (see fig 2) indicated that this increase was mainly due to an increase in the age group 25 years and above.

Gonorrhoea among men having sex with men in two European networks by age group, reported by sexually transmitted infection services during the period 1991–6, relative to the values in 1991.
COMPARISON OF TRENDS IN THE NETWORKS WITH NATIONAL AVAILABLE DATA
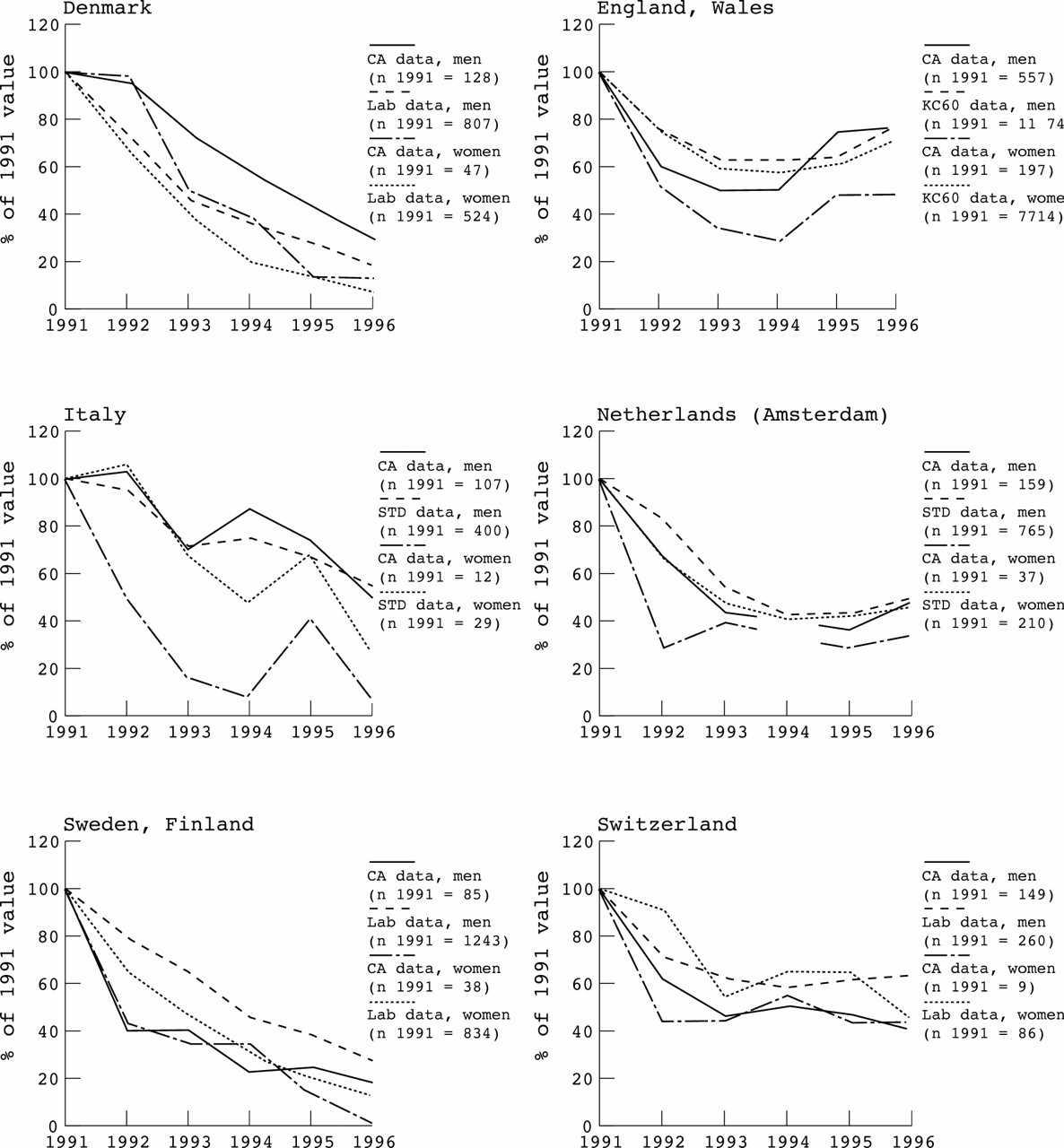
The comparison of trends observed in the concerted action data with trends observed in laboratory reports of Neisseria gonorrhoeae or more extensive clinical reporting or notification data of gonorrhoea in the same country could be carried out for six networks (see fig 3).

{kind=link}
{kind=link}
{kind=link}
Comparison between trends observed in the Concerted Action (CA) project and trends observed in laboratory reports of Neisseria gonorrhoeae or more extensive sexually transmitted infection networks (six networks), relative to the 1991 value. A description of the comparison data sets is presented in the text.
For the Danish, Swedish and Finnish, and Swiss networks, trends were compared with data from laboratory reports.10–15 For the England and Wales network, the trends were compared with aggregated data from all sexually transmitted infection clinics in England and Wales.16 For the Italian and Dutch networks, the comparator was data from the national surveillance system for sexually transmitted diseases.17–19 In Netherlands, however, data between 1991 and 1996, stratified by sex, were only available for the sexually transmitted infection clinic in Amsterdam. Figure 3 reveals that the trends observed in the concerted action are remarkably similar to those observed in the other data sets, even though the number of cases in the concerted action, especially for women, were, for some networks, small.
Discussion
Although the main purpose of the European concerted action was not to monitor trends in sexually transmitted diseases, a major outcome of the project was that a large data bank was created with sexually transmitted infection data from different sentinel networks across Europe. The data were collected according to a standard protocol and validated and collated by the coordinating centre in Brussels.
It is acknowledged that the proportion of patients with gonorrhoeal disease which are covered by the type of health facility participating in this Concerted Action project will vary substantially from one country to another. The primary objective of the concerted action project was, however, to detect changes in the proportion of HIV infected individuals over time. The sentinel populations were not chosen to be representative of the total population of all patients with a sexually transmitted infection in a country. The objective of this analysis, in accordance with the objective of the concerted action, was to assess trends over time. In this respect, representativeness is less important than the stability of the networks over time. Since each network remained stable, in terms of catchment population and patient characteristics, and data were stratified according to sex and sexual orientation, and since other nationally available data indicated similar trends, we believe that it is possible to draw conclusions and make comparisons of the trends that were observed.
A declining trend in cases of gonorrhoea among heterosexual males and all women was observed in the concerted action data between 1991 and 1996 in several European countries. Trends among men having sex with men also showed a decline in the early 1990s, but in the second half of the study period a levelling off, or even an upward trend, was observed in some networks. For those countries with information on laboratory reports of Neisseria gonorrhoea or clinical reports/notifications of gonorrhoea during the same period, trends were similar to those in the concerted action.
The concerted action trends are also in line with previous reports in a number of western European countries during the past two decades.20–23 Several factors may explain the overall decline in gonorrhoea in western Europe during the past two decades.6, 24 These include improved treatment facilities, a wider use of antibiotics for other illnesses that might result in the serendipitous treatment of coincident gonorrhoea, and increased condom use and safer sexual behaviours resulting from sexual health promotion developed in response to the emergence of HIV/AIDS. In Sweden the decline has also been attributed to intensive contact tracing.23, 25
If the trends do reflect changes in sexual behaviour, it would be valuable to get a better insight into the nature of these changes. The notion that the occurrence of gonorrhoea in a population reflects some evenly distributed variable of sexual behaviour is generally not supported. The more accepted concept is that of the core group model, which emphasises that changes in gonorrhoea incidence mainly reflect changes in behaviour among a small number of highly sexually active individuals.26–28 Our data support this concept as an important proportion of the gonorrhoea episodes were observed among individuals who were highly sexually active (data not shown). Figure 1 suggests that trends in gonorrhoea are less favourable among men having sex with men than among heterosexual men and women. Increases of gonorrhoea in men having sex with men were documented at the end of the 1980s both in the United Kingdom and Netherlands,29, 30 and more recently in the United Kingdom,31, 32 and is clearly confirmed by the concerted action trends observed in England and Wales. There were also increases in the absolute number of cases of gonorrhoea in the Dutch network among men having sex with men between 1995 and 1996. A possible explanation for the increase in cases of gonorrhoea among men who have sex with men in England and Wales and Netherlands at the end of the study period is that a group of men, who had previously made appropriate changes towards safer sex, are reverting to unsafe sexual practices. Figure 2 would suggest that in both countries this group is largely made up of men having sex with men above the age of 25. This is in line with a recent study in Greece where a gradual quantitative and qualitative shift toward older ages was observed among gonorrhoea cases in men.33
The correlation between trends in reported gonorrhoea incidence and the effectiveness of disease prevention programmes is not straightforward,34 and it would therefore be incorrect to conclude that the different trends observed in this study represent simple performance measures of different health systems in Europe. None the less, the more pronounced decline in the number of gonorrhoeal cases, especially among heterosexual men and women, in the Scandinavian networks compared to the other European networks is notable. The significance of this phenomenon remains unclear. It may reflect differences of healthcare systems but may also reflect differences in cultural attitudes to the discussion of biology and sexual relations and the effect of that on AIDS and sexually transmitted infection prevention.23
Although the Czech network was not included in our analysis because complete data were only obtained from 1992 onwards and the catchment population changed during the study period, it is worthwhile mentioning that this network was the only network to report an increase in cases of gonorrhoea among women between 1992 and 1996. This is in line with increasing sexually transmitted disease rates among prostitutes that have previously been observed in the Czech Republic.35 The sharp contrast between the declining trends in western Europe and the explosive trends in eastern Europe needs to be emphasised. According to WHO figures, the estimated incidence of gonorrhoea in eastern Europe and central Asia was almost twice the level estimated in western Europe in 1995, among both men and women.1 The increasing incidence of gonorrhoea and other sexually transmitted infections in eastern Europe will be without any doubt a growing public health problem during the coming years and may possibly influence future trends in western Europe.
With the increasing mobility of people within Europe and especially the influx of people from eastern Europe to other European regions, there is greater need to look at changing patterns of sexually transmitted infection at a European level and to compare trends between different areas. A sexually transmitted infection surveillance programme based on a network of sentinel sexually transmitted infection centres in different European countries, including countries in eastern Europe would be a useful tool to reach this objective. The concerted action has shown that such a project is feasible and that it would be possible to integrate the sexually transmitted infection surveillance systems which are already in place in most of the European countries.
The data from the project indicate that in most countries and most exposure categories gonorrhoea in western Europe declined during the first half of the 1990s. Against this positive observation on the sexual health of heterosexuals in western Europe we found less favourable trends among men having sex with men during more recent years, and a possible rise in cases in the one network from eastern Europe. Further investigations are necessary to determine if this observation is due to an increase in risky sexual behaviours in this population group.
Acknowledgments
We wish to thank the European Commission, Directorate General XII, Brussels, Belgium for its financial support (contract number BIOMED 1 Contract PL 941392, formerly BMH1-CT94-1392). We also thank all the study sites and their teams, as well as the international experts who have contributed to this EC project.
The European Study Group
A Stroobant, V Batter, A Sasse, J Van der Heyden, Scientific Institute of Public Health, Brussels; B Kriz, National Institute of Public Health, Prague; A M Worm, E Smith, Statens Serum Institut, Copenhagen; M Catchpole, C McGarrigle, Public Health Laboratory Service, London; A Pönka, Helsinki Centre of the Environment, Helsinki; L Meyer, Institut National de Santé et de la Recherche Médicale, Paris; S Golsch, Dermatologische Klinik der Technischen Universität München; M Hadjivassiliou Pappa, M Vounatsou; National University of Athens; B Suligoi, M Giuliani; Istituto Superiore di Sanita, Rome; J A R van den Hoek, J S A Fennema, Municipal Health Service, Amsterdam; W I Van der Meijden, R Chin-A-Lien, University Hospital Dijkzigt, Rotterdam; H Moi, Olafiaklinikken, Oslo; J Cardoso, I Santo, Centro de Saude da Lapa, Lisbon; G M Allardice, Scottish Centre for Infection and Envrionmental Health, Glasgow; A Scoular, Royal Infirmary, Glasgow; I De la Mata, Hospital de Basurto, Bilbao; C Anagrius, Falu Lasarett, Falun (Sweden); W J Paget, Swiss Federal Office of Public Health, Bern.
Contributors: All members who are listed in the European Study Group had a substantial contribution to the conception of this article, the critical revision for important intellectual content, and the final approval of the version to be published. The four main authors were responsible for the design, the analysis, and the interpretation of the article.
Apart from the authors the following people made a substantial contribution to this project by coordinating the project at national level, by organising the data collection and management of the project, and by contributing to the yearly workshops that were organised to monitor the activities: M Bruckova, National Institute of Public Health, Prague; D Mercey, Mortimer Centre, London; K Visa, Helsinki Centre of the Environment, Helsinki; E Couturier, Centre Collaborateur OMS-SIDA, Saint-Maurice (France); Y Brossard, Hôpital Saint-Antoine, Paris; H J Vogt, R Von Zümbüsch, Dermatologische Klinik der Technischen Universität München; J Stratigos, National University of Athens; P Steegmans, University Hospital Dijkzigt, Rotterdam; A Granholt, Olafiaklinikken, Oslo; DJ Goldberg, Scottish Centre for Infection and Environmental Health, Glasgow; G Scott, Royal Infirmary, Edinburgh; A Arana, V Esteban, T Cisterna, Hospital de Basurto, Bilbao; A K Ruden, Falu Lasarett, Falun (Sweden); A Eichmann, Stadtspital Triemli, Zürich; Th Rufli, Dermotologische Universitätsklinik, Basel.
References
Footnotes
-
↵* Members of the European Study Group are listed at the end of the paper.